
Abstract
Background
In early gastric cancer (EGC) and gastric adenoma, residual tumors may develop despite complete endoscopic resection (ER). To improve the chance of curative resection, we investigated the risk factors of residual tumor development in completely resected gastric epithelial neoplasia after ER.
Methods
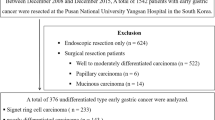
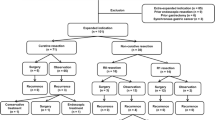
In total, 3,879 gastric epithelial neoplasms showing complete resection after ER were examined; 46 (1.2 %) residual tumors were found upon follow-up endoscopy. Clinicopathological characteristics were evaluated between those with and without residual tumors.
Results
For gastric adenoma, high-grade dysplasia and severe intestinal metaplasia (IM) in the background mucosa were significantly associated with residual tumors. For EGC, poorly differentiated adenocarcinoma (PD), signet ring cell carcinoma (SRC), having a minimum lateral safety margin of <3 mm, and localization in the upper third of the stomach were significantly associated with residual tumors. Multivariate analysis revealed that a lateral safety margin of <3 mm (OR 13.8; p < 0.001), PD (OR 16.3; p = 0.014), and SRC (OR 9.8; p = 0.009) among EGC patients, and severe IM in the background mucosa (OR 9.0; p = 0.024) among gastric adenoma patients, were significantly associated with residual tumors.
Conclusions
For neoplasms with undifferentiated histology (PD or SRC), short-term endoscopic follow-up may help to detect residual tumors that form after complete resection via ER. For EGC, the lateral margin may be considered safe if greater than 3 mm. However, the possibility of satellite lesions should be investigated when the gastric adenoma to be resected is surrounded by severe IM.
Similar content being viewed by others

References
Ono H, Kondo H, Gotoda T, Shirao K, Yamaguchi H, Saito D, Hosokawa K, Shimoda T, Yoshida S (2001) Endoscopic mucosal resection for treatment of early gastric cancer. Gut 48:225–229
Gotoda T (2007) Endoscopic resection of early gastric cancer. Gastric Cancer 10:1–11
Lambert R (2003) Treatment of esophagogastric tumors. Endoscopy 35:118–126
Japanese Gastric Cancer Association. Gastric cancer treatment guidelines 2nd edition. Tokyo: Kanehara 2004. http://www.jgca.jp/PDFfiles/GL2004VER2.PDF.Accessed on February 26, 2010
Gotoda T, Yanagisawa A, Sasako M, Ono H, Nakanishi Y, Shimoda T, Kato Y (2000) Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer 3:219–225
Yoon H, Kim SG, Choi J, Im JP, Kim JS, Kim WH, Jung HC (2013) Risk factors of residual or recurrent tumor in patients with a tumor-positive resection margin after endoscopic resection of early gastric cancer. Surg Endosc 27:1561–1568
Ryu KW, Choi IJ, Doh YW, Kook MC, Kim CG, Park HJ, Lee JH, Lee JS, Lee JY, Kim YW, Bae JM (2007) Surgical indication for non-curative endoscopic resection in early gastric cancer. Ann Surg Oncol 14:3428–3434
Jung H, Bae JM, Choi MG, Noh JH, Sohn TS, Kim S (2011) Surgical outcome after incomplete endoscopic submucosal dissection of gastric cancer. Br J Surg 98:73–78
Park JC, Lee SK, Seo JH, Kim YJ, Chung H, Shin SK, Lee YC (2010) Predictive factors for local recurrence after endoscopic resection for early gastric cancer: long-term clinical outcome in a single-center experience. Surg Endosc 24:2842–2849
Watanabe H, Jass JR, Sobin LH (1990) Histological Typing of Oesophageal and Gastric Tumours: WHO International Histological Classification of Tumours, vol 18, 2nd edn. Springer, Berlin
Lauren P (1965) The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma: an attempt at a histo-clinical classification. Acta Pathol Microbiol Scand 64:31–49
Japanese Gastric Cancer Association (1998) Japanese Classification of Gastric Carcinoma-2nd English Edition. Gastric Cancer 1:10–24
Akahoshi K, Chijiwa Y, Hamada S, Sasaki I, Nawata H, Kabemura T, Yasuda D, Okabe H (1998) Pretreatment staging of endoscopically early gastric cancer with a 15 MHz ultrasound catheter probe. Gastrointest Endosc 48:470–476
Yamashiro K, Suzuki H, Nagayo T (1977) Electron microscopic study of signet-ring cells in diffuse carcinoma of the human stomach. Virchows Arch A Pathol Anat Histol 374:275–284
Maehara Y, Sakaguchi Y, Moriguchi S, Orita H, Korenaga D, Kohnoe S, Sugimachi K (1992) Signet ring cell carcinoma of the stomach. Cancer 69:1645–1650
Mori M, Adachi Y, Kakeji Y, Korenaga D, Sugimachi K, Motooka M, Ooiwa T (1992) Superficial flat-type early carcinoma of the stomach. Cancer 69:306–313
Nonaka K, Kita H (2013) Endoscopic Submucosal Dissection for Early Gastric Cancer. J Cancer Ther 4:26–32
Abraham SC, Montgomery EA, Singh VK, Yardley JH, Wu TT (2002) Gastric adenomas: intestinal-type and gastric-type adenomas differ in the risk of adenocarcinoma and presence of background mucosal pathology. Am J Surg Pathol 26:1276–1285
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2012R1A1A1042417).
Disclosures
Drs. Yun, Kim, Lee, Lee, Shin, Park, Chung, Park, Youn, and Park have no conflict of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yun, G.W., Kim, JH., Lee, Y.C. et al. What are the risk factors for residual tumor cells after endoscopic complete resection in gastric epithelial neoplasia?. Surg Endosc 29, 487–492 (2015). https://doi.org/10.1007/s00464-014-3693-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3693-5