
Abstract
Background
The clinical significance of tertiary lymphoid structure (TLS) in gastric cancer (GC) was uncertain.
Methods
A systematic search was performed in public databases for eligible studies as of April 2, 2023. Meta-analyses were performed to interrogate the associations between TLS levels and prognosis and immunotherapy response of GC. Bioinformatic analyses based on the nine-gene signature of TLS were further conducted to capture the biological underpinnings.
Results
Eleven studies containing 4224 GC cases were enrolled in the meta-analysis. TLS levels positively correlated with smaller tumor size, earlier T stage and N stage. Moreover, higher TLS levels were detected in diffuse and mix subtypes of GC (P < 0.001). Higher TLS levels strongly predicted favorable postoperative overall survival of GC, with HR of 0.36 (95%CI 0.26–0.50, P < 0.001) and 0.55 (95%CI 0.45–0.68, P < 0.001) of univariate and multivariate Cox analysis, respectively. Higher TLS levels were also in favor of the treatment response of anti-PD-1 inhibitors as later-line therapy of GC. TLS levels positively correlated with immune effector cells infiltration, diversity and richness of T cell receptor and B cell receptor repertoire, immune checkpoint genes expression, and immune-related genes mutation of GC in the TCGA-STAD cohort, representing higher immunogenicity and immunoactivity. Moreover, moderate accuracy of TLS levels in predicting benefit from anti-PD-1 inhibitors in the PRJEB25780 cohort was also validated (AUC 0.758, 95%CI 0.583–0.933), higher than the microsatellite instability-score and Epstein-Barr virus status.
Conclusions
TLS levels demonstrated potential in predicting the postoperative prognosis and immunotherapy response of GC.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Gastric cancer (GC) is a major cause of cancer-related mortality globally (Sung et al. 2021), with exceptionally high disease burden in East Asia (Etemadi 2017). GC is featured by high heterogeneity at histological, cellular, (epi)genomic, and proteomic levels, accompanied by distinct clinical outcomes (Wadhwa et al. 2013; Ge et al. 2018). Despite good response to treatment in early-stage GC, advanced GC is highly aggressive, with a median overall survival (OS) time of around 10 months (Smyth et al. 2020). In recent years, immunotherapy has revolutionized the treatment landscape of advanced GC and significantly extended patients’ survival (Li et al. 2021a). However, only a limited population benefited from immunotherapy, and a wide variation of response rates was reported, calling for better biomarkers for stratified treatment (Janjigian et al. 2021; Shitara et al. 2020).
Proteomic markers such as PD-L1 expression (Kim et al. 2018) and molecular markers such as microsatellite instability (MSI) (Kwon et al. 2021) have been established as potential biomarkers of prognosis and responses to immune checkpoint inhibitors (ICIs), whereas findings between different clinical trials were inconsistent. Recently, components in the tumor microenvironment (TME) of GC, such as the contents (Ren et al. 2021) and spatial location (Chen et al. 2022) of different cell types, and specialized structures like tertiary lymphoid structure (TLS) (Yu et al. 2022), have received increasing attention for they could affect prognosis and immunotherapy efficiency.
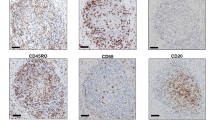
Composed of cellular aggregates in non-lymphoid organs under inflammatory conditions like infection and tumor, TLSs show analogical functional and structural features with lymph nodes (Schumacher and Thommen 2022). Mature TLS is characterized by the B-cell zone that involves the germinal center and is surrounded by the follicular helper T cells. The T-cell zone containing dendritic cells and high endothelial venules is also crucial to TLS (Sautès-Fridman et al. 2019). TLSs signify privileged regions for immune cell maturation and antigen presentation, serving as the crucial milieu for anti-tumor immunity. Emerging evidence indicated that TLS presence strongly correlated with higher immunoreactivity and better clinical outcomes of GC. For instance, Li and colleagues reported that TLS presence was indicative of favorable OS based on a cohort containing 63 GC cases (Li et al. 2020), and Yin et al. further showed that TLS was a promising predictor for longer survival of Epstein-Barr Virus (EBV)-associated GC (Yin et al. 2022). Moreover, Jiang et al. proposed that TLS positively correlated with superior response of ICIs based on a cohort containing 13 GC samples (Jiang et al. 2022). However, some studies were limited by small sample sizes or specific GC subtypes, thus may lack generalizability to some extent. Moreover, associations between TLS and prognosis and therapeutic sensitivity of GC are controversial, probably because samples from different ethnicities and different detecting approaches for TLS were applied.
Consequently, we conducted a meta-analysis to clarify the prognostic and predictive values of TLSs in GC. Simultaneously, we performed bioinformatic validation to capture the biological underpinnings by TLS-related gene signature in external cohorts. Our comprehensive analyses provided the latest evidence for the relationships between TLS and GC, probably conveying a powerful biomarker for clinical practice.
Methods
Guidance and protocol
The present study was conducted based on Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (Liberati et al. 2009), and the protocol was registered at the Prospective Register of Systematic Reviews (PROSPERO ID CRD42023413227).
Search strategy
Two authors (H.X.P. and X.R.W.) independently searched publicly available databases, including the Cochrane Library, Embase, PubMed, and Web of Science, to retrieve suitable studies before April 2, 2023. The references of identified articles were also reviewed to seek potential research. The search strings are presented in Supplementary Table 1.
Included and excluded criteria
Studies were regarded eligible if: (1) focusing on GC populations; (2) examining TLSs in situ of tumor samples by immunohistochemistry (IHC) or hematoxylin–eosin (H&E) staining; (3) evaluating the associations between TLSs and survival or therapeutic response of GC; (4) publishing in English with available full-text. Studies were excluded if: (1) sample size < 10; (2) comments, conference abstracts, or letters to the editor; (3) outcome data could not be obtained or estimated.
Study selection
Independent authors H.X.P. and X.R.W. screened titles and abstracts to obtain eligible studies, the full texts of which were further reviewed. Disagreements were addressed via discussion with senior investigators (Y.C.).
Data extraction
Researchers (H.X.P. and X.R.W.) independently utilized standardized forms to collect data, such as sample size, clinicopathologic characteristics, and TLS location and detecting approaches. Outcome measures were also extracted, including hazard ratio (HR) with corresponding 95% confidence interval (CI) and number of responders/non-responders to ICIs.
Quality assessment
The Newcastle–Ottawa Scale (NOS), with scores ranging from 0 to 9, was exploited to estimate the quality of the included study. Two independent authors (H.X.P. and X.R.W.) performed the workflow, and differing opinions were resolved by consensus. A study with a NOS score greater than 6 was determined high-quality.
Evaluating correlations between TLSs and clinicopathologic parameters of GC
Clinicopathologic data of GC samples, including age, tumor size, T stage, N stage, pTNM stage, and differentiation status, were extracted and re-classified into a high and low group of each parameter. Specifically, age of 50, tumor size of 5 cm, T1 + T2/T3 + T4 stage, N0/N1 stage, I + II/III + IV pTNM stage, and poor/moderate or well differentiation were used as cut-off values. Then, chi-square and Fisher’s exact tests were exploited to compare differences between groups with or without TLSs.
Data synthesis
Statistical analyses were performed on Stata (version 15) and R (version 4.3.1) software. Considering the between-study differences in detecting and quantifying TLS, TLS levels were utilized uniformly to report the findings. For outcome measures of prognosis, HRs and corresponding CIs were pooled. For ICIs response, outcome measures were expressed and pooled as odds ratio (ORs) and 95%CIs. Inter-study heterogeneity was estimated by I2 statistic, and it was considered notable if I2 ≥ 50% (Higgins and Thompson 2002). The random-effects model was adopted if substantial heterogeneity was observed. Otherwise, the fixed-effects model was utilized. Statistical significance was defined at P < 0.05.
Publication bias and sensitivity analyses
The funnel plot test, Begg’s test, and Egger’s test were employed to assess publication bias, which was further tested and adjusted by the trim-and-fill method (Duval and Tweedie 2000). Sensitivity analysis was performed by removing each study one by one.
Biological validation of TLS signature
The genomic profiles, mRNA expression, T-cell receptor (TCR) and B-cell receptor (BCR) repertoire, and clinical characteristics data of GC samples (n = 443) from the TCGA-STAD cohort were downloaded from the UCSC Xena (https://xena.ucsc.edu/) database. The single-sample Gene Set Enrichment Analysis (ssGSEA) approach was adopted to calculate the enrichment scores of TLS by the nine-gene signature (CCL19, CCR7, CETP, CXCL10, CXCL11, CXCL13, CXCL9, LAMP3, SELL) as previously reported (Cabrita et al. 2020; Hou et al. 2022).
As for immune infiltration estimation, enrichment scores of 29 immune signatures were computed via the ssGSEA method (He et al. 2018), and the abundance of 22 immune cell lineages was quantified through the CIBERSORT algorithm (Newman et al. 2015) based on bulk RNA-seq data.
Predicting ICIs efficacy of the TLS signature
The clinical and transcriptomic data were collected from the PRJEB25780 cohort, in which metastatic GC patients (n = 61) were treated with pembrolizumab monotherapy as later-line therapy (Kim et al. 2018). Forty cases (65.6%) had more than two sites of metastasis and nearly half of them had previously undergone second-line therapy. Twenty-eight (45.9%) and twelve (19.7%) patients had PD-L1 combined positive score of more than 1 and 5, respectively. Moreover, 6 patients were tested to be EBV positivity, and 7 patients held MSI-H status. The TLS-score represented by the nine-gene signature was calculated for each sample in the same manner to discover the predictive effects of TLS-score on ICIs efficacy.
Statistical analysis
Mann–Whitney U test and chi-square test were applied to compare categorical and continuous data, respectively. Correlation analysis was conducted via Spearman’s test. Visualization of survival differences was generated by Kaplan–Meier curves and tested through the log-rank test. The threshold of statistical significance was set as P < 0.05.
Results
Study collection and characteristics
As presented in the PRISMA workflow (Fig. 1), 106 records were identified from public databases in the initial literature search. After carefully screening titles and abstracts, and subsequent full-text review, 11 studies incorporating 4224 GC samples were ultimately enrolled (Yu et al. 2022; Li et al. 2020; Yin et al. 2022; Jiang et al. 2022; Li et al. 2023; Kemi et al. 2023; Mori et al. 2022; Cheng et al. 2021; Mori et al. 2021; Yamakoshi et al. 2021; He et al. 2020). Baseline information and major characteristics are shown in Table 1.

The flow diagram of searching and selecting study process
The majority of studies were from East Asian countries (n = 9, 82%), reflecting the relatively high disease burden of GC. Among the 11 included studies, 8 studies reported the associations between TLS levels and postoperative prognosis of GC, 2 studies additionally reported the predictive values of TLS on immunotherapy response, and the rest one only reported the predictive significance of TLS on immunotherapy (Table 1). Two studies assessed the TLS location within tumor tissue, i.e., intra-/peri-tumor, while the remaining applied global estimation. Seven out of eleven studies enrolled stage IV GC patients, and the total number of stage IV GC cases included in the meta-analysis was 151, accounting for 3.6% of the overall population. Eight studies used IHC to detect TLS, while the residuals applied H&E staining. The NOS scores of the enrolled studies ranged from 5 to 8, with eight studies achieving high-quality (73%) (Supplementary Table 2).
Associations between TLS levels and clinicopathologic features
Higher TLS levels positively correlated with smaller tumor size (OR 0.674, 95%CI 0.505–0.901, P = 0.008), earlier T stage (OR 0.187, 95%CI 0.096–0.366, P < 0.001) and N stage (OR 0.758, 95%CI 0.608–0.944, P = 0.013) (Table 2). Higher TLS levels also correlated with a trend of earlier pTNM stage whereas without statistical significance. Interestingly, diffuse (P < 0.001) and mix (P < 0.001) subtypes of GC were positively associated with higher TLS levels. No significant associations between age, gender or differentiation status and TLS levels were observed.
Prognostic effects of TLS levels on GC survival
Meta-analysis was conducted to pool HRs and corresponding CIs for OS (Fig. 2A, Supplementary Fig. 1). In the univariate analyses, TLS levels correlated with significantly better OS of GC (high vs. low: HR 0.36, 95%CI 0.26–0.50, P < 0.001; low vs. high: HR 1.70, 95%CI 1.34–2.06, P < 0.001). However, high heterogeneity was observed, likely caused by heterogeneous GC subtypes and different TLS detecting methods. The favorable prognostic effects of TLS remained significant in the multivariate analyses (high vs. low: HR 0.55, 95%CI 0.45–0.68, P < 0.001; low vs. high: HR 1.62, 95%CI 1.27–1.97, P < 0.001). Details of the covariates used for multivariate analysis of each study are summarized in Supplementary Table 3.

Clinical significance of tertiary lymphoid structures (TLSs) in gastric cancer (GC). The postoperative prognostic effects of TLSs on overall survival of GC, stratified by analytical methods, TLSs location, detected methods, sample size, and median age of the included cases (A). The predictive effects of TLSs on immunotherapy response of GC (B). OR odds ratio; PD progressive disease; PR partial response; SD, stable disease
Subgroup analyses were also performed according to detection methods, sample size, and median age of included patients. The prognostic effects of TLS levels on GC survival stayed salient across different subgroups while slightly attenuated in combined H&E staining and IHC detection subgroup and sample size greater than 200 subgroup. Interestingly, TLS presence was a strong and favorable prognosticator of younger (HR 0.27, 95%CI 0.17–0.42, P < 0.001) than elder (HR 0.66, 95%CI 0.47–0.92, P = 0.015) GC patients. Only two studies assessed the prognostic effects of intratumoral TLS, while insignificant association (HR 0.38, 95%CI 0.07–1.97, P = 0.251) and high heterogeneity (I2 = 92.3, P < 0.001) were found, possibly attributed to limited cases. Collectively, TLS was a strong and favorable postoperative prognosticator of GC.
Publication bias and sensitivity analyses
Despite Begg’s test result being insignificant (P = 0.273), the Funnel plot was not symmetrical, and Egger’s test indicated the existence of publication bias (P = 0.005). The trim-and-fill approach was further employed to test and adjust the publication bias. Results demonstrated the possibility of publication bias (HR 0.72, 95%CI 0.51–1.01), potentially attributed to the high heterogeneity of the included studies (Supplementary Fig. 2). The leave-one-out analysis demonstrated an insignificant impact on the merged effects after excluding any of the enrolled research, implying the stability of the finding.
Predictive effects of TLS levels on ICIs response
Three studies with 33 GC patients receiving anti-PD-1 therapy were enrolled. Two cohorts enrolled GC patients with nivolumab as a third-line or later treatment (Mori et al. 2022; Mori et al. 2021), and the rest did not provide more details (Yin et al. 2022). A total of 6 patients reached partial response (PR), while the residuals were defined as stable disease (SD) and progressive disease (PD) (Schwartz et al. 2016). Meta-analysis showed that higher TLS levels favored ICIs response (OR 20.68, 95%CI 2.94–145.31, P = 0.002), and broad CI may be attributed to the limited sample size (Fig. 2B).
TLS signature in the TCGA-STAD database
The main dilemma for studying TLS lies in the absence of a criterion for detecting and quantifying. Traditional approaches such as IHC and H&E staining were time-consuming and prone to subjective bias. The gene signature of TLS derived from transcriptomic data, primarily representing T cells and B cells in TLS, has been recently proposed and shown to be effective in quantifying TLSs (Sautès-Fridman et al. 2019). The 9-gene TLS signature has been adopted in melanoma (Cabrita et al. 2020), ovarian (Hou et al. 2022), and lung cancer (Feng et al. 2021), conveying notable predictive and prognostic implications.
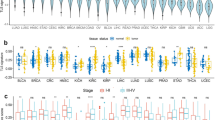
Firstly, considering the heterogeneity of GC, we compared the TLS levels between different GC subtypes (Fig. 3A). Diffuse GC (DGC) conveyed the highest TLS levels, while tubular not otherwise specified. We additionally compared the TLS levels among different molecular subtypes of GC, including EBV-infected, MSI, genomically stable, and chromosomally unstable tumors. Results showed that the EBV-infected subtype held the highest TLS levels, while the chromosomally unstable subtype demonstrated the lowest, conforming to the pathological mechanism associated with TLS formation (Supplementary Fig. 3A). GC samples were then divided into TLS-high/low groups upon the median value of TLS levels as a cutoff point. Insignificant OS difference was observed between TLS-high and TLS-low groups of overall GC (Log-rank P = 0.73) (Fig. 3B). Subgroup analysis showed that a high TLS level indicated longer OS of intestinal GC (Log-rank P = 0.049) (Fig. 3C–G). Multivariate Cox regression analysis adjusting for age, gender, T stage, and N stage further conveyed that TLS level was an independent prognostic factor of intestinal GC (HR 0.289, 95%CI 0.116–0.722, P = 0.008) (Fig. 3H). A trend of favorable prognosis in the TLS-high group of DGC was also shown, despite without statistical significance. Moreover, insignificant associations between TLS levels and prognoses of different molecular GC subtypes were observed (Supplementary Fig. 3B–E).

The tertiary lymphoid structures (TLS)-level spectrums of different gastric cancer (GC) subtypes and their prognostic effects. TLS levels varied significantly among different pathological subtypes of GC (A). Overall survival differences between high/low TLS-level groups of overall GC (B), intestinal GC (C), tubular GC (D), diffuse GC (E), mucinous GC (F), and not otherwise specified adenocarcinoma (G). The prognostic value of TLS levels on intestinal GC, as evaluated by multivariate Cox regression analysis (H). NOS not otherwise specified
We subsequently deciphered the TME landscapes concerning TLS levels, aiming at seeking out biological underpinnings responsible for the prognostic values of TLS. Significantly different infiltrated features between high and low TLS-level groups were found. Infiltration of major immune effector cells, including CD8 + T cells, CD4 + T cells, memory B cells, and natural killer cells, were significantly higher in the high TLS-level group than in low ones, indicating an “immune-hot” TME (Fig. 4A, B). TLS-score also positively correlated with the richness and diversity of TCR (Fig. 4D, E) and BCR repertoire (Fig. 4F, G) (R > 0.45, P < 0.001), suggesting higher antigen presentation function. Moreover, the TLS levels were positively associated with the expression levels of major immune checkpoint genes, including LAG3, TIGIT, CD274, and BTLA (Fig. 4C), implying potential benefit from immunotherapy.

Immune landscape differences between high and low tertiary lymphoid structure (TLS)-level groups in the TCGA-STAD dataset. The distribution of TLS-level, overall survival status, and corresponding immune profiles, as evaluated by the ssGSEA method (A). The immune infiltration differences between high and low TLS-level groups, as evaluated by the CIBERSORT approach (B). Correlation heatmap demonstrating the associations between TLS levels and expression of major immune-checkpoint genes (C). Scatter plots indicating the associations between TLS levels and richness and diversity of T-cell receptor (D, E) and B-cell receptor (F, G) repertoire. P values of the Wilcoxon t test, **P < 0.01; ***P < 0.001; ****P < 0.0001; ns non-significant
The mutation landscapes upon TLS levels were also depicted, resulting in significantly different genetic spectrums (Fig. 5A, B). Among the top 25 mutant genes, the mutated frequencies of ARID1A (P < 0.05) (Li et al. 2019), OBSCN (P < 0.05) (Liu et al. 2021), and AHNAK2 (P < 0.01) (Zheng et al. 2021), which were previously reported to correlate with higher immunogenicity, were significantly higher in the TLS-high group (Fig. 5C–I). Moreover, the mutant frequency of PIK3CA (P < 0.05) was significantly higher in the TLS-high group.

Genomic mutation landscapes concerning tertiary lymphoid structure (TLS) levels and their predictive values of immunotherapy response. Gene mutation spectrum differences between low and high TLS-level groups (A, B). Mutational frequencies of ARID1A (C), OBSCN (D), AHNAK2 (E), PIK3CA (F), LRP1B (G), ZFHX4 (H), and DNAH5 (I) differed significantly between high and low TLS-level groups. Response rate differences to anti-PD-1 therapy between low and high TLS-level groups in the PRJEB25780 cohort (J-K). Predictive accuracy of immunotherapy benefits of TLS-level (L) and other established biomarkers (M). P values of the chi-square tests between different groups
Collectively, TLS levels positively correlated with immune effector cells infiltration, TCR and BCR repertoire diversity and richness, immune checkpoint genes expression, and immune-related genes mutation of GC, signifying potential benefit from immunotherapy.
Validation of the predictive effects of TLS in the PRJEB25780 cohort
We then verified whether TLS signature could predict ICIs benefits in an external cohort. A total of 7 (7 out of 15) and 5 (5 out of 30) responders to anti-PD-1 inhibitors in the TLS-high and TLS-low groups were found, respectively. The proportion of responders was strikingly higher in the high than low TLS-score group (P < 0.05) (Fig. 5J, K). TLS levels also showed moderate accuracy in predicting benefit from immunotherapy (AUC 0.758, 95%CI 0.583–0.933) (Fig. 5L), higher than the MSI-score (AUC 0.708, 95%CI 0.563–0.854) and EBV-status (AUC 0.708, 95%CI 0.563–0.854) while slightly lower than mutation load (AUC 0.790, 95%CI 0.632–0.949) (Fig. 5M). In brief, the TLS levels showed potential as a biomarker for immunotherapy response of GC.
Discussion
Through a comprehensive meta-analysis of 11 studies containing 4,224 GC cases, we pinpointed that TLS correlated with favorable prognosis and ICIs sensitivity of GC. Biological validation in the TCGA-STAD and PRJEB25780 cohorts further corroborated that TLS presence signified higher immunoactivity in TME.
The prognosis of GC is known to be affected by tumor- and host-correlated characteristics, such as age, pTNM stage, and histologic subtypes. Consequently, we first interrogated the relationships between TLS levels and clinicopathologic features. Results showed that higher TLS levels correlated with smaller tumor size and earlier T and N stages, consistent with the findings in breast cancer (BC) (Wang et al. 2022) and lung cancer (Rakaee et al. 2021). Interestingly, higher TLS levels were discovered in diffuse and mix than intestinal subtypes of GC. Since TLS is distinguished by B-cell enriched regions, a recent single-cell atlas also documented significantly higher B-cell infiltration as a salient feature of DGC (Kumar et al. 2022). Wang et al. also reported that TLS presence predicted higher tumor-infiltrating lymphocyte (TIL) levels of BC by meta-analysis (Wang et al. 2022). Nonetheless, we could not assess whether TLS levels correlate with higher infiltration of TILs in meta-analysis due to the nature of the data.
Systematical meta-analysis indicated that higher TLS levels strongly predicted favorable OS of postoperative GC, with HR of 0.36 and 0.55 of univariate and multivariate Cox analysis, respectively. Sensitivity analyses further validated the stability and robustness of our findings. Noteworthy, high heterogeneity was found between the included studies. Thus, subgroup analyses stratified by the TLS detecting methods, sample size, and median age of the included cases were carried out to interrogate potential heterogeneity. Strikingly, the prognostic value of TLS remained significant across subgroups and was more notable in younger than elder GC cases. The heterogeneity decreased as expected, whereas it remained modest. Moreover, meta-analysis implicated that GC patients with high TLS levels significantly benefited from anti-PD-1 inhibitors as later-line therapy than those with low TLS levels. However, considering the limited included cases and retrospective design of studies, the predictive effects of TLS on ICIs sensitivity need to be interpreted cautiously.
The maturation degree of TLS is postulated to affect its clinical significance by recent work. For instance, mature TLS with GC predicted significantly longer survival than total TLSs, whereas such prognostic effect attenuated when the formation of GC was damaged (He et al. 2023; Ling et al. 2022). Meanwhile, the prognostic value of TLS varied by its location in the tumor tissue. Intratumor TLS seemingly demonstrated a stronger prognostic effect than peritumor TLS, whereas findings were inconsistent between different cancer types (Sofopoulos et al. 2019; Li et al. 2021b). There is evidence that TLS levels remarkably varied from early to advanced stage of cancer (Sautès-Fridman et al. 2019). Additionally, studies showed that TLS levels significantly attenuate in the metastatic sites compared to the primary tumors, and can even be absent (Lee et al. 2019). And patients who hold TLS both in the primary tumor and metastatic site exhibit superior prognosis (Cipponi et al. 2012). However, we could not perform comprehensive subgroup analyses on the maturation degree or spatial location of TLS due to the nature of data. Therefore, future studies characterizing TLS with compositional, spatial, and functional details are imperative and encouraged.
Considering the unique puzzles in identifying and quantifying TLSs via traditional methods like H&E staining and IHC, we further validated the findings from meta-analysis and discovered the underlying biological underpinnings via TLS-relevant gene signature, which has been verified in multiple cancer types (Cabrita et al. 2020; Hou et al. 2022; Feng et al. 2021). Strikingly, higher TLS levels were found in DGC than in other subtypes, in congruence with the meta-analysis. Despite without significance, a trend of better prognosis was also observed in DGC individuals with higher TLS levels. Moreover, TLS level was proven to be an independent prognostic factor of intestinal GC.
The TME landscapes concerning TLS levels were subsequently depicted. Higher immune infiltration of major immune effector cells, such as T and B lymphocytes and natural killer cells, were observed in the high TLS-level group than in low ones, indicative of an “immune-hot” TME. Future studies integrating TLS levels and immune infiltration features within TME may offer a more comprehensive and robust prognosticator. Interestingly, higher mast cell (MC) infiltrates were found in the TLS-low group. Evidence showed that MCs could stimulate regulatory T cells to facilitate GC progression (Lv et al. 2023). Studies also reported that inhibition of the degranulation of MC attenuated the development of GC, signifying a potential target (Gunjigake et al. 2021). We also parsed the relationships between the TLS levels and the diversity and richness of the immune repertoire, which represents the strength and breadth of immune responses and acts a paramount role in anti-tumor immunity (Jiang et al. 2019). Higher diversity and richness of TCR and BCR were discovered in the TLS-high group, representing higher antigen presentation function.
Higher TLS levels also correlated with upregulated immune checkpoint genes expression. This may also partly explain why ICIs boost strong antitumor immunity in cancers with enriched TLSs (Petitprez et al. 2020). Intriguingly, ICIs could also instigate TLS formation. For instance, Sarah et al. reported the accumulation of TLS-correlated B cells in responders after neoadjuvant ICIs of melanoma (Helmink et al. 2020). Moreover, the genetic portraits significantly differed between different TLS-level groups. Elevated mutational frequencies of several genes that correlated with immune infiltration were observed in the TLS-high group. For example, a higher mutation rate of ARID1A, a tumor suppressor gene that is relevant to the MSI feature of cancers (Mullen et al. 2021), was found in the TLS-high group. ARID1A-mutated GC held higher TMB and PDL1 levels and favored higher immune cell infiltrates (Li et al. 2019). In brief, high TLS levels represent high immunogenicity and immunoactivity, possibly driving benefits from immunotherapy.
Eventually, we interrogated whether TLS levels could predict ICIs response in the PRJEB25780 cohort, in which GC patients received later-line pembrolizumab monotherapy. Intriguingly, more responders were identified in the TLS-high group than the low ones. Moderate accuracy in predicting benefit from ICIs of TLS-level was presented (AUC > 0.75), higher than the MSI and EBV-status, which are established biomarkers indicative of immunotherapy response (Bai et al. 2022; Yu et al. 2022).
The present work firstly and comprehensively offered substantial evidence for the clinical significance of TLS in GC by meta-analysis and biological validation. Meanwhile, several limitations should be noted. First, different scoring approaches and thresholds in evaluating high/low TLS levels were utilized in different studies. However, we could not perform corresponding subgroup analyses due to unavailable data, probably leading to bias. Second, the pooled sample size for discovering and validating the predictive effect of TLS on ICIs response was limited, thus may lack robustness. Third, high heterogeneity among studies caused potential publication bias in the meta-analysis. Additionally, all the included researches were retrospectively investigated and may risk intrinsic structural biases. Moreover, findings concerning the biological underpinnings of TLS were still at the speculative and analytic stage based on gene signature, without in vivo and in vitro functional validation.
Future studies should focus on establishing a common standard for identifying and quantifying TLS and future prospectively validating it in randomized trials for better clinical applications. Second, pinpointing dynamic changes of cellular components and location within TLS during immunotherapy leads to better comprehending its biological implications. Moreover, inducing the formation of TLS, like by intratumoral injection of vital cytokines such as CXCL13 (Delvecchio et al. 2021), administration of engineered cells (GeurtsvanKessel et al. 2009) and tumor vaccines (Zhang et al. 2021), may provide a neoteric perspective for synergistic immunotherapeutic method.
Conclusions
In brief, higher TLS levels positively correlate with higher immunogenicity and immunoactivity in TME, demonstrating potential in predicting postoperative prognosis and immunotherapy response of GC. Future studies with prospective design are needed to validate the clinical significance of TLS, individually or jointly with other markers, across different cancer types.
Availability of data and material
Data used to support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- BCR:
-
B-cell receptor
- CI:
-
Confidence interval
- DGC:
-
Diffuse gastric cancer
- EBV:
-
Epstein-Barr virus
- GC:
-
Gastric cancer
- H&E:
-
Hematoxylin–eosin
- HR:
-
Hazard ratio
- ICI:
-
Immune checkpoint inhibitor
- IHC:
-
Immunohistochemistry
- MSI:
-
Microsatellite instability
- MC:
-
Mast cell
- NOS:
-
Newcastle–Ottawa Scale
- OR:
-
Odds ratio
- OS:
-
Overall survival
- PD:
-
Progressive disease
- PR:
-
Partial response
- ssGSEA:
-
Single-sample gene set enrichment analysis
- SD:
-
Stable disease
- TCR:
-
T-cell receptor
- TLS:
-
Tertiary lymphoid structure
- TMB:
-
Tumor mutation burden
- TME:
-
Tumor microenvironment
References
Bai Y, Xie T, Wang Z, Tong S, Zhao X, Zhao F et al (2022) Efficacy and predictive biomarkers of immunotherapy in Epstein-Barr virus-associated gastric cancer. J Immunother Cancer. 10(3):e004080
Cabrita R, Lauss M, Sanna A, Donia M, Skaarup Larsen M, Mitra S et al (2020) Tertiary lymphoid structures improve immunotherapy and survival in melanoma. Nature 577(7791):561–565
Chen Y, Jia K, Sun Y, Zhang C, Li Y, Zhang L et al (2022) Predicting response to immunotherapy in gastric cancer via multi-dimensional analyses of the tumour immune microenvironment. Nat Commun 13(1):4851
Cheng N, Li P, Cheng H, Zhao X, Dong M, Zhang Y et al (2021) Prognostic value of tumor-infiltrating lymphocytes and tertiary lymphoid structures in Epstein-Barr virus-associated and -negative gastric carcinoma. Front Immunol 12:692859
Cipponi A, Mercier M, Seremet T, Baurain J-F, Théate I, van den Oord J et al (2012) Neogenesis of lymphoid structures and antibody responses occur in human melanoma metastases. Cancer Res 72(16):3997–4007
Delvecchio FR, Fincham REA, Spear S, Clear A, Roy-Luzarraga M, Balkwill FR et al (2021) Pancreatic cancer chemotherapy is potentiated by induction of tertiary lymphoid structures in mice. Cell Mol Gastroenterol Hepatol 12(5):1543–1565
Duval S, Tweedie R (2000) Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 56(2):455–463
Etemadi A, Safiri S, Sepanlou SG, Ikuta K, Bisignano C, Shakeri R, Amani M, Fitzmaurice C, Nixon M, Abbasi N, Abolhassani H (2020) The global, regional, and national burden of stomach cancer in 195 countries, 1990-2017: a systematic analysis for the Global Burden of Disease study 2017. Lancet Gastroenterol Hepatol. 5(1):42–54
Feng H, Yang F, Qiao L, Zhou K, Wang J, Zhang J et al (2021) Prognostic significance of gene signature of tertiary lymphoid structures in patients with lung adenocarcinoma. Front Oncol 11:693234
Ge S, Xia X, Ding C, Zhen B, Zhou Q, Feng J et al (2018) A proteomic landscape of diffuse-type gastric cancer. Nat Commun 9(1):1012
GeurtsvanKessel CH, Willart MAM, Bergen IM, van Rijt LS, Muskens F, Elewaut D et al (2009) Dendritic cells are crucial for maintenance of tertiary lymphoid structures in the lung of influenza virus-infected mice. J Exp Med 206(11):2339–2349
Gunjigake K, Kinoshita J, Yamaguchi T, Saito H, Fujimori D, Horiike T et al (2021) Interleukin-17A derived from mast cells contributes to fibrosis in gastric cancer with peritoneal dissemination. Gastric Cancer 24(1):31–44
He Y, Jiang Z, Chen C, Wang X (2018) Classification of triple-negative breast cancers based on Immunogenomic profiling. J Exp Clin Cancer Res 37(1):327
He W, Zhang D, Liu H, Chen T, Xie J, Peng L et al (2020) The high level of tertiary lymphoid structure is correlated with superior survival in patients with advanced gastric cancer. Front Oncol 10:980
He M, He Q, Cai X, Liu J, Deng H, Li F et al (2023) Intratumoral tertiary lymphoid structure (TLS) maturation is influenced by draining lymph nodes of lung cancer. J Immunother Cancer. 11(4):e005539
Helmink BA, Reddy SM, Gao J, Zhang S, Basar R, Thakur R et al (2020) B cells and tertiary lymphoid structures promote immunotherapy response. Nature 577(7791):549–555
Higgins JPT, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21(11):1539–1558
Hou Y, Qiao S, Li M, Han X, Wei X, Pang Y et al (2022) The gene signature of tertiary lymphoid structures within ovarian cancer predicts the prognosis and immunotherapy benefit. Front Genet 13:1090640
Janjigian YY, Shitara K, Moehler M, Garrido M, Salman P, Shen L et al (2021) First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet 398(10294):27–40
Jiang N, Schonnesen AA, Ma K-Y (2019) Ushering in integrated T cell repertoire profiling in cancer. Trends Cancer 5(2):85–94
Jiang Q, Tian C, Wu H, Min L, Chen H, Chen L et al (2022) Tertiary lymphoid structure patterns predicted anti-PD1 therapeutic responses in gastric cancer. Chin J Cancer Res 34(4):365–382
Kemi N, Ylitalo O, Väyrynen JP, Helminen O, Junttila A, Mrena J et al (2023) Tertiary lymphoid structures and gastric cancer prognosis. APMIS 131(1):19–25
Kim ST, Cristescu R, Bass AJ, Kim K-M, Odegaard JI, Kim K et al (2018) Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat Med 24(9):1449–1458
Kumar V, Ramnarayanan K, Sundar R, Padmanabhan N, Srivastava S, Koiwa M et al (2022) Single-cell atlas of lineage states, tumor microenvironment, and subtype-specific expression programs in gastric cancer. Cancer Discov 12(3):670–691
Kwon M, An M, Klempner SJ, Lee H, Kim K-M, Sa JK et al (2021) Determinants of response and intrinsic resistance to PD-1 blockade in microsatellite instability-high gastric cancer. Cancer Discov 11(9):2168–2185
Lee M, Heo S-H, Song IH, Rajayi H, Park HS, Park IA et al (2019) Presence of tertiary lymphoid structures determines the level of tumor-infiltrating lymphocytes in primary breast cancer and metastasis. Mod Pathol 32(1):70–80
Li L, Li M, Jiang Z, Wang X (2019) ARID1A mutations are associated with increased immune activity in gastrointestinal cancer. Cells. 8(7):678
Li Q, Zhang D, He W, Chen T, Yan Z, Gao X et al (2020) CD8+ T cells located in tertiary lymphoid structures are associated with improved prognosis in patients with gastric cancer. Oncol Lett 20(3):2655–2664
Li K, Zhang A, Li X, Zhang H, Zhao L (2021a) Advances in clinical immunotherapy for gastric cancer. Biochim Biophys Acta Rev Cancer 1876(2):188615
Li H, Liu H, Fu H, Li J, Xu L, Wang G et al (2021b) Peritumoral tertiary lymphoid structures correlate with protective immunity and improved prognosis in patients with hepatocellular carcinoma. Front Immunol 12:648812
Li Z, Jiang Y, Li B, Han Z, Shen J, Xia Y et al (2023) Development and validation of a machine learning model for detection and classification of tertiary lymphoid structures in gastrointestinal cancers. JAMA Netw Open 6(1):e2252553
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med 151(4):W65–W94
Ling Y, Zhong J, Weng Z, Lin G, Liu C, Pan C et al (2022) The prognostic value and molecular properties of tertiary lymphoid structures in oesophageal squamous cell carcinoma. Clin Transl Med 12(10):e1074
Liu Z, Wang L, Guo C, Liu L, Jiao D, Sun Z et al (2021) TTN/OBSCN ‘double-hit’ predicts favourable prognosis, ‘immune-hot’ subtype and potentially better immunotherapeutic efficacy in colorectal cancer. J Cell Mol Med 25(7):3239–3251
Lv Y, Tian W, Teng Y, Wang P, Zhao Y, Li Z et al (2023) Tumor-infiltrating mast cells stimulate ICOS+ regulatory T cells through an IL-33 and IL-2 axis to promote gastric cancer progression. J Adv Res. 57:149–162
Mori T, Tanaka H, Suzuki S, Deguchi S, Yamakoshi Y, Yoshii M et al (2021) Tertiary lymphoid structures show infiltration of effective tumor-resident T cells in gastric cancer. Cancer Sci 112(5):1746–1757
Mori T, Tanaka H, Deguchi S, Yamakoshi Y, Miki Y, Yoshii M et al (2022) Clinical efficacy of nivolumab is associated with tertiary lymphoid structures in surgically resected primary tumors of recurrent gastric cancer. PLoS ONE 17(1):e0262455
Mullen J, Kato S, Sicklick JK, Kurzrock R (2021) Targeting ARID1A mutations in cancer. Cancer Treat Rev 100:102287
Newman AM, Liu CL, Green MR, Gentles AJ, Feng W, Xu Y et al (2015) Robust enumeration of cell subsets from tissue expression profiles. Nat Methods 12(5):453–457
Petitprez F, de Reyniès A, Keung EZ, Chen TW-W, Sun C-M, Calderaro J et al (2020) B cells are associated with survival and immunotherapy response in sarcoma. Nature. 577(7791):556–60
Rakaee M, Kilvaer TK, Jamaly S, Berg T, Paulsen E-E, Berglund M et al (2021) Tertiary lymphoid structure score: a promising approach to refine the TNM staging in resected non-small cell lung cancer. Br J Cancer 124(10):1680–1689
Ren F, Zhao Q, Zhao M, Zhu S, Liu B, Bukhari I et al (2021) Immune infiltration profiling in gastric cancer and their clinical implications. Cancer Sci 112(9):3569–3584
Sautès-Fridman C, Petitprez F, Calderaro J, Fridman WH (2019) Tertiary lymphoid structures in the era of cancer immunotherapy. Nat Rev Cancer 19(6):307–325
Schumacher TN, Thommen DS (2022) Tertiary lymphoid structures in cancer. Science. 375(6576):eabf9419
Schwartz LH, Litière S, de Vries E, Ford R, Gwyther S, Mandrekar S et al (2016) RECIST 1.1-Update and clarification: from the RECIST committee. Eur J Cancer. 62:132–7
Shitara K, Van Cutsem E, Bang Y-J, Fuchs C, Wyrwicz L, Lee K-W et al (2020) Efficacy and safety of pembrolizumab or pembrolizumab plus chemotherapy vs chemotherapy alone for patients with first-line, advanced gastric cancer: the KEYNOTE-062 phase 3 randomized clinical trial. JAMA Oncol 6(10):1571–1580
Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, Lordick F (2020) Gastric cancer. Lancet 396(10251):635–648
Sofopoulos M, Fortis SP, Vaxevanis CK, Sotiriadou NN, Arnogiannaki N, Ardavanis A et al (2019) The prognostic significance of peritumoral tertiary lymphoid structures in breast cancer. Cancer Immunol Immunother 68(11):1733–1745
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A et al (2021) Global Cancer Statistics 2020: GLOBOCAN estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71(3):209–249
Wadhwa R, Song S, Lee J-S, Yao Y, Wei Q, Ajani JA (2013) Gastric cancer-molecular and clinical dimensions. Nat Rev Clin Oncol 10(11):643–655
Wang B, Liu J, Han Y, Deng Y, Li J, Jiang Y (2022) The presence of tertiary lymphoid structures provides new insight into the clinicopathological features and prognosis of patients with breast cancer. Front Immunol 13:868155
Yamakoshi Y, Tanaka H, Sakimura C, Mori T, Deguchi S, Yoshii M et al (2021) Association between the preoperative neutrophil-to-lymphocyte ratio and tertiary lymphoid structures surrounding tumor in gastric cancer. Mol Clin Oncol 14(4):76
Yin Y-X, Ling Y-H, Wei X-L, He C-Y, Wang B-Z, Hu C-F et al (2022) Impact of mature tertiary lymphoid structures on prognosis and therapeutic response of Epstein-Barr virus-associated gastric cancer patients. Front Immunol 13:973085
Yu J-S, Huang W-B, Zhang Y-H, Chen J, Li J, Fu H-F et al (2022) The association of immune cell infiltration and prognostic value of tertiary lymphoid structures in gastric cancer. Neoplasma 69(4):886–898
Yu H-Y, Li C-P, Huang Y-H, Hsu S-J, Wang Y-P, Hsieh Y-C et al (2022) Microsatellite instability, epstein-barr virus, and programmed cell death ligand 1 as predictive markers for immunotherapy in gastric cancer. Cancers (Basel). 14(1):218
Zhang Y, Xu J, Fei Z, Dai H, Fan Q, Yang Q et al (2021) 3D printing scaffold vaccine for antitumor immunity. Adv Mater 33(48):e2106768
Zheng L, Li S, Zheng X, Guo R, Qu W (2021) AHNAK2 is a novel prognostic marker and correlates with immune infiltration in papillary thyroid cancer: Evidence from integrated analysis. Int Immunopharmacol 90:107185
Funding
This work was supported by the National Key Research and Development Program of China (No. 2022YFC2505006), the National Natural Science Foundation of China (No. U22A20327, No. 82272858, No. 82203881, No. 91959205), the Beijing Natural Science Foundation (No. 7222021, No. Z200015, No. Z230008), Beijing Hospitals Authority Youth Program (QML20231115).
Author information
Authors and Affiliations
Contributions
Conception and design: HXP, XRW and YC. Administrative support: LS, and CZ. Provision of study materials or patients: all authors. Data analysis and interpretation: HXP, XRW, and YC. Manuscript writing: HXP, XRW and YC. Final approval of manuscript: all authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no potential conflicts of interest.
Ethical approval and consent to participate
The present meta-analysis was registered at the Prospective Register of Systematic Reviews (PROSPERO ID CRD42023413227) and reported in line with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and AMSTAR (Assessing the methodological quality of systematic reviews) Guidelines. Consequently, ethical approval is not available for this study.
Consent for publication
All authors consent to publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
432_2024_5672_MOESM2_ESM.docx
Supplementary Supplementary table 2. Newcastle-Ottawa Quality Assessment Scale evaluating the quality of the included studies. file2 (DOCX 19 KB)
432_2024_5672_MOESM3_ESM.docx
Supplementary Supplementary table 3. Details of covariates used for multivariate analysis of the included studies file3 (DOCX 17 KB)
432_2024_5672_MOESM4_ESM.pdf
Supplementary Supplementary figure 1. Meta-analyses investigating the associations between tertiary lymphoid structures (TLS) levels and overall survival of gastric cancer after radical resection. Forest plots demonstrating the results in the univariate analysis (A-C), multivariate analysis (B-D), hematoxylin-eosin (H&E) staining detection (E), H&E and immunohistochemistry staining detection (F), sample size ≥ 200 (G), sample size < 200 (H), median age ≥ 60 (I), and median age < 60 (J) subgroups. Each result was displayed by the hazard ratio with corresponding 95% confidence interval. file4 (PDF 266 KB)
432_2024_5672_MOESM5_ESM.pdf
Supplementary Supplementary figure 2. Publication bias and sensitivity tests of meta-analyses. The funnel plot examined the publication bias (A). Trim-and-fill method tested and adjusted the publication bias (B-C). Sensitivity analysis as evaluated by the leave-one out-test (D) file5 (PDF 152 KB)
432_2024_5672_MOESM6_ESM.pdf
Supplementary Supplementary figure 3. The tertiary lymphoid structures (TLS)-level profiles of different molecular subtypes of gastric cancer (GC) and their prognostic effects. TLS levels varied significantly among different molecular subtypes of GC (A). Overall survival differences between high/low TLS-level groups of EBV-infected (B), genomically stable (C), microsatellite instability (MSI)-H (D), and chromosomally unstable (E) of GC file6 (PDF 225 KB)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Peng, H., Wu, X., Zhang, C. et al. Analyzing the associations between tertiary lymphoid structures and postoperative prognosis, along with immunotherapy response in gastric cancer: findings from pooled cohort studies. J Cancer Res Clin Oncol 150, 153 (2024). https://doi.org/10.1007/s00432-024-05672-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00432-024-05672-y