
Abstract
The Infant Gastroesophageal Reflux Questionnaire Revised (I-GERQ-R) is used to score and evaluate gastroesophageal reflux (GER) related symptoms such as regurgitation, irritability and crying. A cut-off of ≥ 16 has been suggested to discriminate between GER and GER-disease. However, age-specific normal values were not assessed. Aim of this study was to determine age-specific normal values in healthy infants. Cross-sectional survey in healthy infants aged 0–24 months during their regular check-ups at well-baby clinics and through an online questionnaire using the I-GERQ-R. Infants with a history of (suspected) GER-disease were excluded. Spearman’s correlation coefficient was calculated to explore age-related trends. A total of 979 healthy infants (47% male, median age 6 [0–24] months) were included. Median I-GERQ-R score, regardless of age, was 6 (range: 0–27). I-GERQ-R scores significantly decreased with age (rs = -0.569, p < 0.001). Of all infants, 49 (5%) had a score of ≥ 16 which previously has been considered ‘suggestive of GER-disease’. Scores of ≥ 16 were most frequently seen in newborns aged 0–4 months (16% in 0–1 months to 4% in 3–4 months) and disappeared after the age of 16 months. High scores in the first months of life were caused by a high prevalence of regurgitation, colic-associated symptoms and hiccup frequency.
Conclusion: Age-dependent normal values for the I-GERQ-R show that reflux symptoms decrease in the first 24 months of life in healthy infants. Scores of ≥ 16 should not necessarily be considered abnormal in young infants. Validation as a diagnostic tool for GER-disease using age-appropriate normal values is needed.
What is Known: • The Infant Gastro Esophageal Reflux Questionnaire Revised (I-GERQ-R) was developed to objectively score and evaluate GER-related symptoms in infants. • Previously a cut off of ≥ 16 has been suggested to differentiate between gastro esophageal reflux (GER) and GER-disease. | |
What is New: • We present age-specific normal values of the I-GERQ-R in healthy infants. • I-GERQ-R scores clearly decrease with age and up to 16% of young healthy infants have a score that is above the previously suggested cut-off score of 16 for GER-disease. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In infants, symptoms of gastroesophageal reflux disease (GER-disease) include regurgitation, irritability, crying, and feeding refusal [1,2,3]. These symptoms are nonspecific, as they are also common in healthy infants and overlap with symptoms of cow’s milk allergy or infant colic.
The Infant GastroEsophageal Reflux Questionnaire Revised (I-GERQ-R), a 12-item multiple-choice questionnaire, was developed to objectively score and evaluate gastroesophageal reflux (GER) related symptoms in infants such as regurgitation, irritability and crying [4]. Previously, a cut off of ≥ 16 points has been suggested to differentiate between healthy infants and those with GER-disease [4]. The I-GERQ-R has however not been validated to discriminate between infants with GER-disease and symptomatic infants without GER-disease. Additionally, potential age-related changes in I-GERQ-R scores were not taken into account [4]. The aim of this study was to determine age-specific normal values for the I-GERQ-R in healthy infants (0–24 months).
Methods
This study is a cross-sectional survey regarding GER related symptoms in healthy infants aged 0–24 months.
Ethical approval
The study was exempted from official approval by our local institutional review board (W19_291#19.344) as the medical research involving human subjects act did not apply.
Study population and recruitment of subjects
Healthy infants (0–24 months) visiting well baby clinics in the greater Amsterdam area between October 2017 and March 2020 were eligible for the study. Additionally, healthy infants that were recruited for a previous study [5] at the same well baby clinics between February and October 2015 were included. Parents or caregivers of healthy infants were approached during their regular check-ups and their infants were checked for exclusion criteria. Healthy infants were additionally recruited through online advertisements until June 2021. Parents that expressed their interest online through a GCP clinical database (Castor Edc) were contacted and if infants did not fulfil exclusion criteria, the I-GERQ-R was surveyed.
Exclusion criteria:
Infants were excluded when
-
parents or care givers had poor understanding of Dutch or English language;
-
gestational age at birth < 34 weeks;
-
current GER symptoms (i.e. excessive crying, regurgitation, poor growth or weight loss) being experienced as ‘moderate’, ‘severe’ or ‘very severe’ by parent/caregiver.
-
any health care professional had been consulted at any time before screening, regarding possible GER-related problems, such as excessive crying, regurgitation, poor growth or weight loss.
-
infants used pharmacological and/or non-pharmacological GER therapies either at screening or before;
Questionnaires
I-GERQ-R [6]
The I-GERQ-R is a 12 item multiple choice questionnaire in which frequency and quantity of GER symptoms in the past 7 days are surveyed [4]. It consists of subscales regarding regurgitation related symptoms and colic related symptoms. A maximum total score of 42 can be achieved. Higher scores point towards a larger burden of GER symptoms.
Clinical survey
A short 4-item clinical survey regarding the child’s current age (months), gestational age and reflux-related history was developed to screen eligible infants for exclusion criteria (see Supplemental file 1).
Statistical analysis
SPSS (IBM Statistical Package for the Social Sciences [SPSS] for Windows, v 26.0 Armonk, NY: IBM Corp) was used for calculation of age-dependent I-GERQ-R scores, regurgitation and colic-related subscores and for analysis of median and P5-95 scores of I-GERQ-R scores.
Spearman’s correlation coefficient (rs) was calculated to explore age-related trends. Spearman’s correlation was also used in order to assess whether there was an association between regurgitation subscores and colic subscores. Strength of the correlation was classified as: rs = 0.00–0.19 “very weak”; rs = 0.20–0.39 “weak”; rs = 0.40–0.59 “moderate”; rs = 0.60–0.79 “strong”; rs = 0.80–1.0 “very strong”.
Results
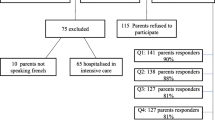
One thousand and four infants were screened for eligibility. Six hundred fifty-five (65.2%) were included at well baby clinics and 349 (34.8%) were recruited through the online advertisement. Twenty-five infants (2.49%) were excluded from analysis because of ex-prematurity (n = 5), consultation of a health care professional for possible GER-related problems (n = 17), or because caregivers considered their child’s GER symptoms as moderate to very severe (n = 4, of which n = 1 also consulted a health care professional for GER symptoms).
A total of 979 infants (47% male, median age 6 [0–24] months) were included in this study. Median I-GERQ-R score of all infants, regardless of age, was 6 (range: 0–27). Of all infants, 49 (5%) had a score of ≥ 16 which is currently considered ‘suggestive of GER-disease’ [4].
Correlations of total I-GERQ-R scores with age
Total I-GERQ-R scores, regurgitation- and colic-related subscores, correlated moderately with age (rs = -0.569, p < 0.001; rs = -0.554, p < 0.001 and rs = -0.380; p < 0.001 respectively) and are displayed in Table 1.
Total I-GERQ-R scores (Fig. 1a), as well as regurgitation- and colic-related subscores (Fig. 1b) significantly decreased with age. A total score of ≥ 16 was most often seen in newborns aged 0–1 month (12/75, 16%). The percentage of cases with scores ≥ 16 rapidly decreased to 4% (3/68) at the age of 4–5 months and disappeared after the age of 15 months (see Fig. 2).

a Median and ranges of total I-GERQ-R scores. Boxes show interquartile ranges; whiskers show range; b Median and ranges of I-GERQ-R subscores scores. Boxes show interquartile ranges; whiskers show range

Percentage of healthy infants with a total I-GERQ-R score of ≥ 16, which is currently considered ‘suggestive of GERD’
Correlations of separate I-GERQ-R items with age
When looking at all I-GERQ-R questions separately, regurgitation frequency, regurgitation quantity and hiccup frequency showed moderate and significant negative correlations with age (rs = -0.517, p < 0.001; rs = -0. 488, p < 0.001 and rs = -0.593; p < 0.001 respectively, see Table 2). The items ‘stopping with eating soon after starting the meal’ and ‘more than usual crying or fussing’ did not show any correlation with age, the remaining I-GERQ-R items showed low or very low correlations with age (Table 2). ‘Feeding refusal’ was the only I-GERQ-R item with a (very weak) positive correlation with age and was most frequently reported in infants aged 15 months and older.
Regurgitation and crying symptoms over time
Regurgitation, for parents or caregivers defined as anything coming out of the mouth, was present in 70–79% of infants in the first 6 months of age (median 1–3 times a day) with a peak prevalence of 79% at the age of 1–2 months (Fig. 3a). Of infants aged 0–6 months (n = 570) old that regurgitate daily (n = 415, 73%), 251 (24%) regurgitated 1–3 times a day, 105 (18%) 3–6 times a day and 59 (10%) > 6 times a day.

a Regurgitation frequency displayed as percentages of the four different categories of regurgitation frequency; b Crying frequency displayed as percentages of the four different categories of crying time a day
Between 7–12 months old, prevalence of regurgitation ranged between 44 and 15% and dropped further to 0% afterwards.
Crying symptoms in infants decreased faster than regurgitation symptoms: infants aged 0–4 months cried the most (median crying times of 10 min up to an hour, Fig. 3b).
Fifty-five percent of infants aged 4 months and older had a reported crying time of less than 10 min a day.
Association between regurgitation and colic subscores
The regurgitation subscore showed a significant weak correlation with colic-associated subscore of the I-GERQ-R (rs = 0.393; p < 0.001).
Association between regurgitation and feeding problems
The regurgitation subscore did not correlate with the frequency of feeding refusal (rs = -0.049, p = 0.125).
Discussion
To our knowledge, this is the largest study documenting age-dependent I-GERQ-R scores in a cohort of healthy infants aged 0–24 months. It shows that I-GERQ-R normal values are age-dependent and that up to 16% of young healthy infants have a score that is above the previously suggested cut-off score of 16 for GER-disease [4].
In this study [4], symptomatic patients might have been incorrectly attributed to the GER-disease group while in fact, their symptoms might have not been due to GER-disease [4].
Furthermore, by excluding symptomatic patients in the control group, the study did not evaluate the difference between patients with- and without GER-disease but the difference between subjects with and without symptoms [4, 7]. Last, age-related differences in the I-GERQ-R were not taken into account. These may all be reasons why previous attempts to validate the I-GERQ-R questionnaire for clinical use as a diagnostic tool failed.
Our results are in line with other, yet smaller studies with different study-populations [8, 9]. These studies reported I-GERQ-R scores > 16 in 26% and 19% of infants aged 1 month old [8, 9]. I-GERQ-R scores decreased with age and similar to our results, one of these studies showed that only 2% of infants aged 12 months had scores above the cut-off of ≥ 16 [9].
Overall, GER symptoms as measured with the I-GERQ-R, decreased significantly with age, mostly in the first 12 months of life. The strong decline in I-GERQ-R score in the first year of life was mainly caused by a reduction of regurgitation and crying symptoms and hiccup frequency. After the age of 1 year, these symptoms disappeared in nearly all infants.
After the age of 12 months, the overall I-GERQ-R score stabilized. While regurgitation prevalence further decreased, feeding refusal increased from the age of 15 months onwards. It should be noted that this concerns parent-reported feeding problems in a group of healthy subjects. It could thus well be that a developmental change in behavior in older infants and toddlers may have impacted feeding behavior, which was conceived to be problematic by parents. In fact, an increase in feeding problems after infancy was described by others as well and feeding problems in pre-school children are reported to occur in the normal population in up to 50% and are often considered part of normal development in toddlers [10, 11].
Regurgitation in infants is common and has, similar to our results, been shown to decrease significantly with age in multiple studies [8, 9, 12,13,14,15,16,17]. Due to the different definitions of regurgitation used in these studies, peak prevalence and peak age of regurgitation differed. Only one study assessed regurgitation symptoms beyond the age of 12 months and reported that symptoms diminished with age, with only 5% of infants ‘spilling more than half of their feeds’ at the age of 14 months [13].
The age-dependent normal values reported in this study should not be mistaken for diagnostic cut-off values to differentiate infants with and without GER-disease. Evaluation of I-GERQ-R values in a large cohort of patients with well characterized GER-disease is needed, after which validation as a diagnostic instrument should take place. While such studies may be difficult to perform, a validated age-dependent non-invasive tool to distinguish infants with GER-disease from those with symptoms related to physiological GER is highly needed.
The high outliers in our study show that the I-GERQ-R may not prove to be a perfect test to diagnose GER-disease after all, but even if it could be validated to rule out GER-disease with certainty, this would be a large step forward in reducing the overprescription of PPI [18,19,20].
The rapid decrease of the I-GERQ-R score in young infants should be taken into account not only for the further development of diagnostic cut off values for the presence or absence of GER-disease, but also be considered when interpreting results in therapeutic trials. Our study suggests that a decrease of 5 points, which is currently considered clinically relevant [4], has a different clinical relevance for young infants as compared to older ones and may also simply be attributed to increasing age.
Strengths of our study are the large number of subjects and the strict inclusion criteria to ensure that our cohort consists of healthy infants without GER-disease. To reduce selection bias, we visited well-baby clinics in urban neighborhoods with different socio-economic statuses. The well-baby clinics in the Netherlands are visited by nearly all healthy infants and toddlers in the country [21, 22].
Limitations of our study include the relatively low inclusion numbers of infants aged > 16 months. Additionally, we did not survey tobacco exposure and infant’s diets. Whether these parameters may potentially have an impact on GER symptoms, is still under debate [8, 13, 23,24,25,26].
Conclusion
Gastroesophageal reflux symptoms measured by the I-GERQ-R, decrease in the first 24 months of age in healthy infants. Our results show that total scores of ≥ 16 should not necessarily be considered pathological in young infants. Future studies in infants with- and without GER-disease are needed to validate age-dependent I-GERQ-R cut-off values and to evaluate whether these can discriminate between infants with physiological GER and GER-disease.
Abbreviations
- GER:
-
Gastroesophageal Reflux
- GER-disease:
-
Gastroesophageal reflux disease
- I-GERQ-R:
-
Infant Gastroesophageal Reflux Questionnaire Revised
References
Vandenplas Y, Salvatore S, Hauser B (2005) The diagnosis and management of gastro-oesophageal reflux in infants. Early Hum Dev 81(12):1011–1024
Rosen R, Vandenplas Y, Singendonk M, Cabana M, DiLorenzo C, Gottrand F et al (2018) Pediatric gastroesophageal reflux clinical practice guidelines: Joint recommendations of the North American society for pediatric gastroenterology, hepatology, and nutrition and the European society for pediatric gastroenterology, hepatology, and nutrition. J Pediatr Gastroenterol Nutr 66(3):516–554
Nelson SP, Chen EH, Syniar GM, Christoffel KK (2000) Prevalence of symptoms of gastroesophageal reflux during childhood: a pediatric practice-based survey. Pediatric Practice Research Group. Arch Pediatr Adolesc Med 154(2):150–154
Kleinman L, Rothman M, Strauss R, Orenstein SR, Nelson S, Vandenplas Y et al (2006) The infant gastroesophageal reflux questionnaire revised: development and validation as an evaluative instrument. Clin Gastroenterol Hepatol 4(5):588–596
Woodland P, Singendonk MMJ, Ooi J, Nikaki K, Wong T, Lee C et al (2019) Measurement of salivary pepsin to detect gastroesophageal reflux disease is not ready for clinical application. Clin Gastroenterol Hepatol 17(3):563–565
I-GERQ, Orenstein S (2004) Infant Gastroesophageal Reflux Questionnaire Revised (I-GERQ-R). University of Pittsburgh. Used under license from the University of Pittsburgh
Orenstein SR (2010) Symptoms and reflux in infants: Infant Gastroesophageal Reflux Questionnaire Revised (I-GERQ-R)–utility for symptom tracking and diagnosis. Curr Gastroenterol Rep 12(6):431–436
Van Howe RS, Storms MR (2010) Gastroesophageal reflux symptoms in infants in a rural population: longitudinal data over the first six months. BMC Pediatr 10:7
Curien-Chotard M, Jantchou P (2020) Natural history of gastroesophageal reflux in infancy: new data from a prospective cohort. BMC Pediatr 20(1):152
Cardona Cano S, Hoek HW, van Hoeken D, de Barse LM, Jaddoe VW, Verhulst FC et al (2016) Behavioral outcomes of picky eating in childhood: a prospective study in the general population. J Child Psychol Psychiatry 57(11):1239–1246
Nelson SP, Chen EH, Syniar GM, Christoffel KK (1998) One-year follow-up of symptoms of gastroesophageal reflux during infancy. Pediatric Practice Research Group. Pediatrics 102(6):E67
Nelson SP, Chen EH, Syniar GM, Christoffel KK (1997) Prevalence of symptoms of gastroesophageal reflux during infancy. A pediatric practice-based survey. Pediatric Practice Research Group. Arch Pediatr Adolesc Med 151(6):569–572
Martin AJ, Pratt N, Kennedy JD, Ryan P, Ruffin RE, Miles H et al (2002) Natural history and familial relationships of infant spilling to 9 years of age. Pediatrics 109(6):1061–1067
Hegar B, Boediarso A, Firmansyah A, Vandenplas Y (2004) Investigation of regurgitation and other symptoms of gastroesophageal reflux in Indonesian infants. World J Gastroenterol 10(12):1795–1797
Hegar B, Dewanti NR, Kadim M, Alatas S, Firmansyah A, Vandenplas Y (2009) Natural evolution of regurgitation in healthy infants. Acta Paediatr 98(7):1189–1193
Miyazawa R, Tomomasa T, Kaneko H, Tachibana A, Ogawa T, Morikawa A (2002) Prevalence of gastro-esophageal reflux-related symptoms in Japanese infants. Pediatr Int 44(5):513–516
Osatakul S, Sriplung H, Puetpaiboon A, Junjana CO, Chamnongpakdi S (2002) Prevalence and natural course of gastroesophageal reflux symptoms: a 1-year cohort study in Thai infants. J Pediatr Gastroenterol Nutr 34(1):63–67
Barron JJ, Tan H, Spalding J, Bakst AW, Singer J (2007) Proton pump inhibitor utilization patterns in infants. J Pediatr Gastroenterol Nutr 45(4):421–427
Aznar-Lou I, Reilev M, Lødrup AB, Rubio-Valera M, Haastrup PF, Pottegård A (2019) Use of proton pump inhibitors among Danish children: A 16-year register-based nationwide study. Basic Clin Pharmacol Toxicol 124(6):704–710
De Bruyne P, Christiaens T, Vander Stichele R, Van Winckel M (2014) Changes in prescription patterns of acid-suppressant medications by Belgian pediatricians: analysis of the national database, [1997-2009]. J Pediatr Gastroenterol Nutr 58(2):220–225
Centraal Bureau voor de Statistiek. (2022) Available from https://opendata.cbs.nl/#/CBS/nl/dataset/83716NED/table?searchKeywords=consultatiebureau
Centraal Bureau voor de Statistiek. (2014) Available from https://www.cbs.nl/nl-nl/nieuws/2014/44/ouders-geven-consultatiebureau-gemiddeld-een-ruime-7
Alaswad B, Toubas PL, Grunow JE (1996) Environmental tobacco smoke exposure and gastroesophageal reflux in infants with apparent life-threatening events. J Okla State Med Assoc 89(7):233–237
Orenstein SR, Shalaby TM, Cohn JF (1996) Reflux symptoms in 100 normal infants: diagnostic validity of the infant gastroesophageal reflux questionnaire. Clin Pediatr (Phila) 35(12):607–614
Salvatore S, Hauser B, Vandemaele K, Novario R, Vandenplas Y (2005) Gastroesophageal reflux disease in infants: how much is predictable with questionnaires, pH-metry, endoscopy and histology? J Pediatr Gastroenterol Nutr 40(2):210–215
Campanozzi A, Boccia G, Pensabene L, Panetta F, Marseglia A, Strisciuglio P et al (2009) Prevalence and natural history of gastroesophageal reflux: pediatric prospective survey. Pediatrics 123(3):779–783
Acknowledgements
We thank students Anass Errami, Betül Atalik, Sanjay Thakoerdin, Melissa Rosiers and Romy Koning for their help with taking the I-GERQ-R questionnaires. We thank Veronique van Erp, Irene Aartsen and their colleagues from Stichting Amsterdamse Gezondheidscentra for enabling us to collect our questionnaires in the waiting room of their well-baby clinics in Amsterdam.
Funding
No external funding for this manuscript.
Author information
Authors and Affiliations
Contributions
MvW conceptualized and designed the study, coordinated and supervised data collection, reviewed and revised the manuscript. MB supervised data collection, and critically reviewed the manuscript for important intellectual content. MvL and FL collected data, carried out the analyses, drafted the initial manuscript and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Peter de Winter
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van Lennep, M., Lansink, F., Benninga, M.A. et al. Age-dependent normal values for the ‘Infant Gastroesophageal Reflux Questionnaire Revised’. Eur J Pediatr 183, 445–452 (2024). https://doi.org/10.1007/s00431-023-05281-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-023-05281-w