
Abstract
Repeated exposure to pain and stress in early life may cause alterations in pain sensitivity later in life. Children born preterm are often exposed to painful invasive procedures. This study aimed to explore the relationship between being born preterm and self-report of spinal pain in pre-adolescence. This prospective study was based on the Danish National Birth Cohort and consisted of 47,063 11–14-year-olds. Data from the Danish National Birth Cohort were linked with national registers through Statistics Denmark. Analyses were performed as multiple logistic regression models estimating odds ratios and 95% confidence intervals. Spinal pain (neck, mid back, and/or low back pain) was assessed using a subdivision of the Young Spine Questionnaire. Severe spinal pain was defined as having pain often or once in a while with an intensity of four to six on the Revised Faces Pain Scale. Inverse probability weighting was used to account for potential selection bias. Girls born very preterm (< 34 full weeks of gestation) were less likely to report spinal pain (OR: 0.60; 95% CI: 0.40–0.93) compared with those term-born. The associations were weaker when examining moderate to severe spinal pain and when examining the three spinal regions separately. None of these was statistically significant.
Conclusion: We found no associations for boys. In conclusion, this study indicates that girls born very preterm are seemingly less likely to have severe spinal pain in pre-adolescence than girls born at term.
What is Known: • Spinal pain is one of the largest disease burdens globally, and the evidence regarding the etiology of spinal pain in children and adolescents is limited. • Repeated exposure to pain and stress in early life (i.e., being preterm) may cause alterations in pain sensitivity later in life. | |
What is New: • Girls born very preterm (< 34 full weeks of gestation) seem less likely to report severe spinal pain in pre-adolescence compared with girls born at full term. • There is no association between gestational age and later experience of spinal pain in pre-adolescent boys. |
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Spinal pain (i.e., low back, mid back, and/or neck pain) is one of the largest disease burdens globally [1], with back pain being the leading cause of years lived with disability [2]. Spinal pain in adults is well documented [3]. Even though there have been studies regarding spinal pain in children, the evidence remains limited primarily due to methodological limitations and the lack of comparability across these studies [4]. As a result, the reported prevalence of back pain in children and adolescents varies widely, ranging from 7 to 72% [4]. The wide variability in prevalence can be attributed to several factors, including disparities in study populations, sample size, study period, and methodological approaches which complicate compatibility between studies [4]. The findings regarding several risk factors for spinal pain in children are mixed [4], but studies have shown that risk factors for spinal pain include biological, social, and psychological factors [4, 5]. It is further documented that children who experience low back pain often also experience low back pain later in life [6], and that recurrent episodes of back pain may not be a serious of unrelated episodes, but rather a long-term condition [5].
Experience of early life pain is associated with spinal pain among pre-adolescents [7]. Preterm born children often undergo several invasive procedures. These procedures often occur during a period where the brain is under great development and particularly vulnerable for alterations [8]. Repeated exposure to pain and stress in the first years of life can alter the neurological substrate associated with pain perception, which consequently can affect somatosensory processing of pain and change neurobehavioral responses to pain [7, 9,10,11,12]. Building on these findings, the present study was based on the hypothesis that pre-adolescents born preterm may be more sensitive to pain due to early-life pain experiences, resulting in distinct pain perception compared to their term-born peers. Furthermore, preterm birth is known to affect both short- and long-term health outcomes [13,14,15], and children born preterm are at risk of developing late effects of a physical, mental, motor, social, and cognitive nature [13,14,15], which have likewise been associated with higher risk of spinal pain [4, 5]. However, despite this, findings from an epidemiological cohort study have indicated that adults born preterm had a lower risk of reporting musculoskeletal pain, including spinal pain [16].
The overall aim of this study was to explore the relationship between being born preterm and spinal pain in pre-adolescence (11–14 years old, with the majority being 11-year-olds) taking advantage of the large birth cohort The Danish National Birth Cohort (DNBC) as is one of the few databases including information on spinal pain. Specifically, we aimed to examine the association between preterm birth and severe spinal pain among 11–14-year-old boys and girls, respectively, and further whether the association differed according to severity and localization of pain.
Material and methods
Study population
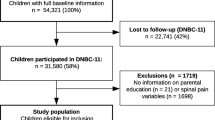
DNBC is a cohort consisting of approximately 100,000 children born from 1996 to 2003 and their mothers, followed by several data collections from early pregnancy through the children’s life [17]. When the children turned 11 years old, they got invited to participate in the 11-year follow-up (DNBC-11), which included questions about spinal pain [17, 18]. The source population consisted of all pre-adolescents included in DNBC. In DNBC-11, a total of 47,063 pre-adolescents contributed with full information on all explanatory measures and spinal pain (Fig. 1); thus, all missing data were excluded. Data from DNBC were linked with nationwide register data on Statistics Denmark through the unique personal identification number assigned to all persons with a permanent residency in Denmark. All data were stored and processed in the secure remote server environment at Statistics Denmark.

Flow chart of study population
Preterm birth
Gestational age at birth was obtained from the Medical Birth Register containing information on all births in Denmark [19]. Gestational age was operationalized into full weeks and further into the following three groups: term (≥ 37 full weeks of gestation), moderate preterm (34–36 full weeks of gestation), and very preterm (< 34 full weeks of gestation).
Spinal pain in pre-adolescence
Spinal pain was assessed in DNBC-11 in which a subdivision of the Young Spine Questionnaire (YSQ) was included. YSQ is a validated questionnaire used to measure the intensity and prevalence of pain in the neck, mid back, and lower back [20]. The original questionnaire consists of 19 questions, of which nine were included in DNBC-11. Frequency was measured by the following options: (1) often, (2) once in a while, (3) once or twice, and (4) never. Intensity was measured by the Revised Faces Pain Scale and ranged from 1 = no pain to 6 = very much pain [20]. There is no verified classification of spinal pain among children but in this study, we used an overall combined measure, which was divided into no pain, moderate pain, or severe pain in the low back, mid back, or neck. This measure was directly adopted from previous work based on the same population [7, 18, 21]. For further detailed information regarding the operationalization of the variable, see the previous study by Joergensen et al. [18]. Thus, severe pain was defined as having pain often or once in a while with an intensity of four or more on the Revised Faces Pain Scale [18, 22]. If the child reported pain in more than one region, the region in which the child reported the most severe pain was included in the outcome. In the main analysis, the outcome was divided into two groups: no pain (including moderate pain) versus severe spinal pain. Secondly, we operationalized a variable in which having experienced spinal pain covered both moderate and severe spinal pain. This variable included having experienced pain once or twice or once in a while or often with an intensity of 3 or more or having pain often with an intensity of 1 or more [18]. The three spinal regions were also investigated separately.
Covariates
With the use of a causal diagram, potential confounders were selected a priori [23] (Supplementary File 1). The selected confounders were parity, maternal age at childbirth, major congenital anomalies, and parental educational level. Information on sex was obtained from DNBC. Age corresponded to the child’s age when responding to DNBC-11. Parity and maternal age at birth were obtained from the Danish Medical Birth Register. Parity was divided into nulliparous or parous. Maternal age at birth was divided into the following groups: < 25, 25–29, 30–34, and > 34 years old. Major congenital anomalies originated from the Medical Birth Register and were defined according to the EuroCAT guidelines [24]. Parental educational level was obtained from The Danish Population’s Education Register [25] and described the highest ongoing or completed educational level of the parents. It was categorized into low (0–2 ISCED), medium (3–4 ISCED), and high (5–8 ISCED) educational level according to the International Standard Classification of Education (ISCED) 2011 [26].
Statistical methods
All statistical analyses were made using STATA V.16.1. Initially, we made descriptive statistics between the exposure of interest and the selected covariables. Categorical variables were reported as proportions and tested for heterogeneity using a chi-squared test. Applying multiple logistic regression models, we examined crude and adjusted associations between preterm birth and severe spinal pain in pre-adolescents aged 11 to 14 years. We estimated odds ratios (OR) and an α-level of 0.05 in the statistical testing was used, corresponding to a 95% confidence interval (95% CI). In all analyses, no spinal pain was considered as the reference outcome. We tested the interaction between preterm birth and sex (p = 0.160) and based on this, we could not definitively reject a possible interaction with sex, and therefore we chose to divide the analyses by sex. The analyses further accounted for the dependency between siblings in the study sample including a robust standard error estimator [27]. Subsequently, we analyzed the association by using the secondary outcomes: “moderate to severe” as well as the spinal regions separately. We performed a loss-to-follow-up analysis to investigate potential selection bias in our analysis population. To this, we used chi-squared tests of heterogeneity to compare study participants with individuals lost to follow-up (Supplementary File 2). In a sensitivity analysis, we further accounted for sample selection (into the cohort and from attrition) by applying inverse probability weighting (IPW) using a reference population consisting of all children born in Denmark between 1996 and 2003 [28, 29]. These analyses were conducted in line with previous spinal pain studies performed in the same study population [7, 18, 30].
Approval of the study
Approval of the study was obtained from the Danish Data Protection Agency through the joint notification of The Faculty of Health and Medical Sciences at The University of Copenhagen (SUND-2017–09) and the DNBC Steering Committee (2017–23). All data were stored and processed at Statistics Denmark and no personally identifiable data were accessible.
Results
Table 1 shows characteristics of pre-adolescents born at term, moderate preterm, and very preterm. In this study population, almost 6% of boys and 5% of girls were born moderate or very preterm. Children born preterm were more often the firstborn child, had mothers below 25 years or over 35 years, and had parents of lower educational level compared to children born to term (Table 1). Boys born very preterm were more likely to have a major congenital anomaly compared to boys born moderate preterm or at term.
The prevalence of spinal pain among boys was 9.8% and 14% among girls (data not shown), where neck pain was the prevailing spinal pain site for both boys and girls (Supplementary file 3). We observed no association between moderate nor very preterm birth and severe spinal pain in boys (ORvery preterm: 0.99, 95% CI: 0.66–1.48) (Table 2). For girls, however, we found that those born very preterm were less likely to report severe spinal pain in pre-adolescence compared to those born to term (OR = 0.60, 95% CI: 0.40–0.93). The association with moderate preterm appeared weaker and was not statistically significant.
In addition, we observed no association for neither boys nor girls when the outcome measure consisted of “moderate to severe” spinal pain (Table 3), or when investigating the spinal regions separately (Table 4). However, there was an indication that the observed association between very preterm birth and severe spinal pain seemed mainly driven by neck pain (Table 4).
Information on the pre-adolescents lost to follow-up is shown in supplementary file 2. Pre-adolescents who were lost to follow-up accounted for 48% of the source population. The chi-squared test showed that the study population differed from the population lost to follow-up. Those lost to follow-up were more often boys, born preterm, from a nulliparous mother, and their mothers were more often < 25 years old at birth. Furthermore, their parents were of lower educational background. Even though the results of the loss-to-follow-up analysis revealed signs of selection, the IPW analyses in which we accounted for potential selection into the cohort and from attrition showed no essential changes to the estimates (data not shown).
Discussion
In this study of more than 45,000 individuals aged 11 to 14, we examined the association between preterm birth and spinal pain in pre-adolescence. Contrary to our expectations, this study suggested that girls born very preterm were less likely to report spinal pain in pre-adolescence than girls born at full term. There was no association for boys or for the spinal regions examined separately. When the outcome of spinal pain included both moderate and severe spinal pain, we found no association among boys nor girls.
This study was based on the hypothesis that pre-adolescents born preterm may be pain sensitized in early life due to several exposures to painful experiences and that their experience of pain, therefore, may differ from pre-adolescents born at term. Several studies suggest that pain sensitivity may be affected in early life and that this may affect how pain is experienced later in life [7, 9, 10, 31, 32]. Based on this knowledge, we expected children born preterm to experience spinal pain to a greater extent compared to children born at term; however, we observed the contrary relationship. We identified one study indicating that children who had several pain experiences in early life were more resilient to pain later in life [9]. However, the differences in findings from these studies may be explained by differences in study designs, study populations varying between 26 and 29,861 subjects, and differences in measurements assessing early-life pain and pain sensitivity [7, 9, 10, 31, 32].
Epidemiological studies have shown an association between puberty stage and back pain in teenagers [33, 34]. Puberty-related changes in hormone levels and subsequent physical, mental, and emotional changes [35] and possibly also stress [36] usually begin around the age of 10–11 in girls and a couple of years later in boys. Studies have shown that girls born preterm have a later onset of puberty than girls born at term [37, 38]. This together with the fact that both stress and poor well-being have been associated with spinal pain [21] could partly explain our findings that preterm girls have less spinal pain [39, 40]. Furthermore, a study examining spinal pain trajectories in children aged 6 to 17 years identified five trajectories with more advanced pubertal development being associated with both rare and moderate increasing pain trajectories [41]. Given that girls born preterm may have a later onset of puberty [37, 38], it is possible that they are more likely to follow a lower pain trajectory compared to their term-born peers. Hence, pubertal timing may be on the causal pathway between gestational age and spinal pain which is why we did not adjust for pubertal stage in this study.
Studies have found a correlation between height and respectively spinal pain and low back pain, where tall people reported pain to a greater extent [33, 42]. Children born preterm can have impaired height growth [43] which could be a part of the explanation of the reduced risk of reporting severe spinal pain among girls born preterm. This could potentially also be relevant for boys later in life, since they have a later growth spurt than girls. A study has found an increased odds for preterm born children to have impaired fine motor skills compared to a matched comparison group [44] and another study has linked poor motor skills at age 7 to neck and mid back pain at age 11 [45]. This may lead to preterm born children reporting spinal pain to a greater extent than children born to term. This does, however, not explain our results.
In addition to our hypothesis of pain sensitization in pre-adolescents born preterm, we also had an assumption that preterm birth may result in parental modeling of pain due to the parents handling and raising the child in a special way, because of a difficult beginning of life. A study describes that biological, psychological, and sociocultural factors are mechanisms underlying the experience of pain [31]. The child’s pain experience can be affected by their parent’s behavior, such that unnecessary worrying and protection can be a negative factor in children’s perception of pain [31, 46].
Being born preterm can lead to various long-term side effects [13,14,15]. Several of these consequences can be experienced worse than spinal pain and therefore may spinal pain not be in focus. This is supported by a study describing that children who had been admitted to a neonatal care unit reported less pain compared with children born term who had not been admitted to the neonatal care unit [9]. The children perceived pain to the same degree, but children admitted to a neonatal care unit avoided to report their pain, which is why they can be considered more robust or more likely to avoid reporting their pain [9].
Strength and limitations
A strength of this study was the large study population, which provided a high degree of statistical power. Despite the large study population, only a small number of the children were born preterm which may not provide enough statistical power to assess the association between preterm birth and spinal pain. Additionally, it is worth noticing that the small numbers in some of the exposure categories and the many performed tests might have led to chance findings and that some of the statistically significant findings could be type 1 errors [47]. A further strength was the prospective study design ensuring temporality and further minimal risk of recall bias, since exposure data were based on register data and outcome data were collected as point prevalence in DNBC-11. Spinal pain was self-reported and pain experience is by default subjective, which may affect the accuracy of the variable [48]. Self-report has, however, been demonstrated as the best option to measure pain in children [49]. Additionally, data on spinal pain originated from YSQ, included in DNBC-11, which is validated to be used to measure the neck, mid back, and low back pain in 9–11-year-olds [20]. Finally, access to Statistic Denmark registers allowing the application of high-quality Danish population registers to obtain information on health and social conditions to adjust for potential confounders strengthened the validity of the study [19, 24, 25]. However, we can never be sure that we completely cover all variables that may confound the relationship.
As always there is selection into the cohort and from attrition, also demonstrated in the loss-to-follow-up analysis, which may have affected the study findings. However, the fact that children born preterm in this study figure in the same level as in the total Danish population is a strength [50]. In addition, a study investigating whether low participation in cohort studies is inducing bias suggested that non-participation did not affect the risk estimates in the DNBC cohort [51]. Finally, to account for potential selection bias, we performed IPW analyses, and as in previous studies in the same population, IPW did not make any essential changes to the estimates; thus, we believe that selection bias had no or a minimum influence on our results.
Conclusion
In contrast to our hypothesis, this study indicates that girls born very preterm were less likely to have severe spinal pain in pre-adolescence than girls born to term, whereas there is seemingly no association between gestational age at birth and spinal pain in boys aged 11–14 years.
Data availability
Access to data requires permission from the Danish Data Protection Agency and the DNBC Steering Committee. Please see https://www.dnbc.dk/access-to-dnbc-data for further information.
Change history
15 December 2023
The Orcid for Anne Cathrine Falch-Joergensen has been added
Abbreviations
- DNBC:
-
The Danish National Birth Cohort
- DNBC-11:
-
The 11-year follow-up of the Danish National Birth Cohort
- ISCED:
-
The International Standard Classification of Education
- OR:
-
Odds ratio
- YSQ:
-
Young Spine Questionnaire
- 95% CI:
-
95% Confidence intervals
References
Kassebaum NJ, Arora M, Barber RM, Bhutta ZA, Brown J, Carter A, m.fl. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet. 8. oktober 2016;388(10053):1603–58.
Wu A, March L, Zheng X, Huang J, Wang X, Zhao J, m.fl. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Ann Transl Med. marts 2020;8(6):299.
Buchbinder R, Blyth FM, March LM, Brooks P, Woolf AD, Hoy DG. Placing the global burden of low back pain in context. Best Practice & Research Clinical Rheumatology. 1. oktober 2013;27(5):575–89.
Kamper SJ, Yamato TP, Williams CM. The prevalence, risk factors, prognosis and treatment for back pain in children and adolescents: an overview of systematic reviews. Best Practice & Research Clinical Rheumatology. 1. december 2016;30(6):1021–36.
Dunn KM, Hestbaek L, Cassidy JD. Low back pain across the life course. Best Practice & Research Clinical Rheumatology. oktober 2013;27(5):591–600.
Hestbaek L, Leboeuf-Yde C, Kyvik KO, Manniche C (2006) The course of low back pain from adolescence to adulthood: eight-year follow-up of 9600 twins. Spine februar 31(4):468–472
Joergensen AC, Lucas R, Hestbaek L, Andersen PK, Andersen AMN (2019) Early-life programming of pain sensation? Spinal pain in pre-adolescents with pain experience in early life. European Journal of Pediatrics december 178(12):1903–1911
Walker SM (2013) Biological and neurodevelopmental implications of neonatal pain. Clinics in Perinatology september 40(3):471–491
Hermann C, Hohmeister J, Demirakça S, Zohsel K, Flor H. Long-term alteration of pain sensitivity in school-aged children with early pain experiences. Pain. 5. december 2006;125(3):278–85.
Grunau RE, Weinberg J, Whitfield MF. Neonatal procedural pain and preterm infant cortisol response to novelty at 8 months. Pediatrics. 1. juli 2004;114(1):e77–84.
Valeri BO, Holsti L, Linhares MB. Neonatal pain and developmental outcomes in children born preterm: a systematic review | Ovid. 2015 [henvist 8. februar 2021]; Tilgængelig hos: https://oce-ovid-com.ep.fjernadgang.kb.dk/article/00002508-201504000-00009/HTML
Vederhus BJ, Eide GE, Natvig GK, Markestad T, Graue M, Halvorsen T (2012) Pain tolerance and pain perception in adolescents born extremely preterm. The Journal of Pain oktober 13(10):978–987
Johnson S. Cognitive and behavioural outcomes following very preterm birth. Seminars in Fetal and Neonatal Medicine. oktober 2007;12(5):363–73.
Marlow N, Wolke D, Bracewell MA, Samara M. Neurologic and developmental disability at six years of age after extremely preterm birth. 6. januar 2005;
Taylor HG (2017) Outcomes of preterm birth: a lifespan perspective. Dev Med Child Neurol 59(5):454–454
Evensen KAI, Tikanmäki M, Heinonen K, Matinolli HM, Sipola‐Leppänen M, Lano A, m.fl. Musculoskeletal pain in adults born preterm: evidence from two birth cohort studies. European Journal of Pain. 2019;23(3):461–71.
Olsen J, Meder K. Better health for mother and child – the Danish National Birth Cohort (DNBC), its structure, history and aims. Nor J Epidemiol. 22. december 2014;24(1–2).
Joergensen AC, Hestbaek L, Andersen PK, Nybo Andersen AM (2019) Epidemiology of spinal pain in children: a study within the Danish National Birth Cohort. Eur J Pediatr maj 178(5):695–706
Bliddal M, Broe A, Pottegård A, Olsen J, Langhoff-Roos J (2018) The Danish Medical Birth Register. Eur J Epidemiol januar 33(1):27–36
Lauridsen HH, Hestbaek L (2013) Development of the young spine questionnaire. BMC Musculoskelet Disord december 14(1):185
Stallknecht SE, Hestbæk L, Strandberg-Larsen K, Andersen AMN, Andersen AMN (2017) Spinal pain and co-occurrence with stress and general well-being among young adolescents: a study within the Danish National Birth Cohort. Eur J Pediatr 176(6):807–814
Hicks CL, van Korlaar I, Goodenough B. The Faces Pain Scale ± Revised: toward a common metric in pediatric pain measurementq. 2001;11.
Greenland S, Pearl J, Robins JM (1999) Causal diagrams for epidemiologic research. Epidemiology 10(1):37–48
EUROCAT. EUROCAT Guide 1.4: instruction for the registration of congenital anomalies [Internet]. EUROCAT Central Registry, University of Ulster; 2021. Tilgængelig hos: https://eu-rd-platform.jrc.ec.europa.eu/eurocat_en
Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 1. juli 2011;39(7_suppl):91–4.
UNESCO Institute for Statistics. International standard classification of education: ISCED 2011 [Internet]. Montreal, Quebec: UNESCO Institute for Statistics; 2012 [henvist 14. januar 2022]. Tilgængelig hos: http://www.uis.unesco.org/Education/Documents/isced-2011-en.pdf
Williams RL (2000) A note on robust variance estimation for cluster-correlated data. Biometrics juni 56(2):645–646
Seaman SR, White IR (2013) Review of inverse probability weighting for dealing with missing data - Shaun R Seaman, Ian R White, [Internet]. 2011 [henvist 13. januar 2022]. Tilgængelig hos: https://journals-sagepub-com.ep.fjernadgang.kb.dk/doi/full/10.1177/0962280210395740
Jacobsen TN, Nohr EA, Frydenberg M (2010) Selection by socioeconomic factors into the Danish National Birth Cohort. Eur J Epidemiol maj 25(5):349–355
Joergensen AC, Strandberg-Larsen K, Andersen PK, Hestbaek L, Andersen AMN (2021) Spinal pain in pre-adolescence and the relation with screen time and physical activity behavior. BMC Musculoskelet Disord december 22(1):393
Evans S, Tsao JCI, Lu Q, Myers C, Suresh J, Zeltzer LK. Parent-child pain relationships from a psychosocial perspective: a review of the literature. 2009;12.
Goffaux P, Lafrenaye S, Morin M, Patural H, Demers G, Marchand S. Preterm births: can neonatal pain alter the development of endogenous gating systems? European Journal of Pain. 1. oktober 2008;12(7):945–51.
Hebert JJ, Leboeuf-Yde C, Franz C, Lardon A, Hestbæk L, Manson N, m.fl. Pubertal development and growth are prospectively associated with spinal pain in young people (CHAMPS study-DK). Eur Spine J. juli 2019;28(7):1565–71.
Janssens KAM, Rosmalen JGM, Ormel J, Verhulst FC, Hunfeld JAM, Mancl LA, m.fl. Pubertal status predicts back pain, overtiredness, and dizziness in American and Dutch adolescents. PEDIATRICS. 1. august 2011;peds.2010–2364.
Pfeifer JH, Allen NB (2021) Puberty initiates cascading relationships between neurodevelopmental, social, and internalizing processes across adolescence. Biological Psychiatry januar 89(2):99–108
Marceau K, Dorn LD, Susman EJ. Stress and puberty-related hormone reactivity, negative emotionality, and parent–adolescent relationships. Psychoneuroendocrinology. 1. august 2012;37(8):1286–98.
Hvidt JJ, Brix N, Ernst A, Lauridsen LLB, Ramlau-Hansen CH. Size at birth, infant growth, and age at pubertal development in boys and girls. CLEP. 19. september 2019;11:873–83.
Hui LL, Leung GM, Lam TH, Schooling CM (2012) Premature birth and age at onset of puberty. Epidemiology maj 23(3):415–422
James E, Wood CL, Nair H, Williams TC (2018) Preterm birth and the timing of puberty: a systematic review. BMC Pediatr december 18(1):3
Wehkalampi K, Hovi P, Dunkel L, Strang-Karlsson S, Järvenpää AL, Eriksson JG, m.fl. Advanced pubertal growth spurt in subjects born preterm: the Helsinki study of very low birth weight adults. J Clin Endocrinol Metab. februar 2011;96(2):525–33.
Hébert JJ, Beynon AM, Jones BL, Wang C, Shrier I, Hartvigsen J, m.fl. Spinal pain in childhood: prevalence, trajectories, and diagnoses in children 6 to 17 years of age. Eur J Pediatr. april 2022;181(4):1727–36.
Hershkovich O, Friedlander A, Gordon B, Arzi H, Derazne E, Tzur D, m.fl. Associations of body mass index and body height with low back pain in 829,791 adolescents. American Journal of Epidemiology. 15. august 2013;178(4):603–9.
Derraik JGB, Lundgren M, Cutfield WS, Ahlsson F. Association between preterm birth and lower adult height in women. Am J Epidemiol. 1. januar 2017;185(1):48–53.
Bos AF, Van Braeckel KNJA, Hitzert MM, Tanis JC, Roze E (2013) Development of fine motor skills in preterm infants. Dev Med Child Neurol 55(s4):1–4
Hestbæk L, Kamper SJ, Hartvigsen J, Falch-Joergensen AC (2023) Motor skills at 7 years of age and spinal pain at 11 years of age: a cohort study of 26,000 preadolescents. Eur J Pediatr [Internet]. [henvist 26. april 2023]; Tilgængelig hos: https://link.springer.com/10.1007/s00431-023-04964-8
Grøholt EK, Stigum H, Nordhagen R, Köhler L (2002) Recurrent pain in children, socio-economic factors and accumulation in families. Eur J Epidemiol oktober 18(10):965–975
Rothman KJ, Greenland S, Lash TL. Data analysis. I: modern epidemiology. Third edition. Philadelphia Baltimore New York: Wolters Kluwer Health, Lippincott Williams & Wilkins; 2008. s. 213–418.
HAUGLAND S, WOLD B, STEVENSON J, AAROE LE, WOYNAROWSKA B. Subjective health complaints in adolescence: a cross-national comparison of prevalence and dimensionality. European Journal of Public Health. 1. marts 2001;11(1):4–10.
Thrane SE, Wanless S, Cohen SM, Danford CA. The assessment and non-pharmacologic treatment of procedural pain from infancy to school age through a developmental lens: a synthesis of evidence with recommendations. Journal of Pediatric Nursing. 1. januar 2016;31(1):e23–32.
Nyfødte og fødsler (1997-) [Internet]. [henvist 22. november 2022]. Tilgængelig hos: https://www.esundhed.dk/Emner/Graviditet-foedsler-og-boern/Nyfoedte-og-foedsler-1997-
Nohr EA, Frydenberg M, Henriksen TB, Olsen J (2006) Does low participation in cohort studies induce bias? Epidemiology juli 17(4):413–418
Acknowledgements
The Danish National Birth Cohort was established with a significant grant from the Danish National Research Foundation. Additional support was obtained from the Danish Regional Committees, the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation, the Health Foundation, and other minor grants. The DNBC Biobank has been supported by the Novo Nordisk Foundation and the Lundbeck Foundation. Follow-ups of mothers and children have been supported by the Danish Medical Research Council (SSVF 0646, 271-08-0839/06-066023, O602-01042B, 0602-02738B), the Lundbeck Foundation (195/04, R100-A9193), the Innovation Fund Denmark 0603-00294B (09-067124), the Nordea Foundation (02-20132014), the Aarhus Ideas (AU R9-A959-13-S804), the University of Copenhagen Strategic Grant (IFSV 2012), and the Danish Council for Independent Research (DFF 4183-00594 and DFF 4183-00152).
Funding
Open access funding provided by Royal Library, Copenhagen University Library The study was supported by the Danish Council for Independent Research (DFF-7016-00344).
Author information
Authors and Affiliations
Contributions
All authors conceptualized and designed the study, contributed to method devolvement, analyses, and interpretation of the results. Anne-Marie Nybo Andersen designed the data collection and instruments, supervised, and did a critical revision of the manuscript. Anne Cathrine Falch-Joergensen carried out data management and supervised the statistical analyses and did a critical revision of the manuscript. Jane Lykke Nielsen and Klara Kaltoft drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical accordance
Approval of the study was obtained from the Danish Data Protection Agency through the joint notification of The Faculty of Health and Medical Sciences at The University of Copenhagen (SUND-2017–09) and the DNBC Steering Committee (2017–23). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Content to participate
Parents of the participants (< 18 years) signed an informed consent before participating in the study. No personal identifiable information was accessible.
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Gregorio Milani
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kaltoft, K., Nielsen, J.L., Andersen, AM.N. et al. The relation between preterm birth and self-reported spinal pain in pre-adolescence—a study of 47,063 subjects from the Danish National Birth Cohort. Eur J Pediatr 183, 203–211 (2024). https://doi.org/10.1007/s00431-023-05264-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-023-05264-x