
Abstract
Purpose
The critical force (CF) concept, differentiating steady and non-steady state conditions, extends the critical power paradigm for sport climbing. This study aimed to validate CF for finger flexors derived from the 4 min all-out test as a boundary for the highest sustainable work intensity in sport climbers.
Methods
Twelve participants underwent multiple laboratory visits. Initially, they performed the 4 min intermittent contraction all-out test for CF determination. Subsequent verification visits involved finger-flexor contractions at various intensities, including CF, CF −2 kg, CF −4 kg, and CF −6 kg, lasting for 720 s or until failure, while monitoring muscle-oxygen dynamics of forearm muscles.
Results
CF, determined from the mean force of last three contractions, was measured at 20.1 ± 5.7 kg, while the end-force at 16.8 ± 5.2 kg. In the verification trials, the mean time to failure at CF was 440 ± 140 s, with only one participant completing the 720 s task. When the load was continuously lowered (−2 kg, −4 kg, and −6 kg), a greater number of participants (38%, 69%, and 92%, respectively) successfully completed the 720 s task. Changes of muscle-oxygen dynamics showed a high variability and could not clearly distinguish between exhaustive and non-exhaustive trials.
Conclusions
CF, based on the mean force of the last three contractions, failed to reliably predict the highest sustainable work rate. In contrast, determining CF as the end-force of the last three contractions exhibited a stronger link to sustainable work. Caution is advised in interpreting forearm muscle-oxygen dynamics, lacking sensitivity for nuanced metabolic responses during climbing-related tasks.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sport climbing, a highly technical activity, places significant stress on the forearm flexors. Extensive research has emphasized the critical role of maximal finger-flexor strength and endurance as reliable predictors of climbing ability (Langer et al. 2023; Stien et al. 2022). Notably, research has shown that climbing-specific tests, including both whole-body climbing and isolated finger-flexor tests, demonstrate high predictability for sport climbing performance (Baláš et al. 2021). Various tests involving continuous and intermittent finger-flexor contractions at different intensities have been proposed (Fryer et al. 2015; Limonta et al. 2016; Michailov et al. 2018; Vigouroux and Quaine 2006). Despite efforts to explore the metabolic contributions of sustained and intermittent contractions (Maciejczyk et al. 2022), these tests face limitations in their transferability to prescribing training intensity, as they do not allow for the determination of intensities in metabolic steady and non-steady states.
Understanding maximal exercise intensity steady state is an important threshold concept in exercise performance. The concept of critical power (CP) directly addresses this exercise state defined as the highest exercise intensity that can be sustained for a significant duration of time or physiologically as the highest metabolic rate that can be maintained by supplied oxygen (O2) consumption (Poole et al. 2016). Recent developments in climbing research have introduced the concept of critical force (CF) as a metabolic threshold between steady and non-steady state conditions, and an extension of the CP paradigm for sport climbing (Baláš et al. 2022; Giles et al. 2019, 2021). The application of multisession three tasks to failure and the 4 min all-out test has been employed to determine CF on a hangboard (Giles et al. 2019, 2021). In addition, exhaustive climbs at varying wall angles aimed to establish the critical angle as a parallel concept to CP (Baláš et al. 2022). Climbers performing the ascent 2° under critical angle sustained the task for 20 min with moderate perceived exertion, while those climbing 2° above critical angle failed approximately 16 min with higher perceived exertion. Notably, these validations have not been conducted for CF determined from hangboard tests, with only criterion validity against self-reported climbing ability reported. Given the integral role of hangboard training in climbing-specific strength training (Levernier and Laffaye 2019; Medernach et al. 2015), the prescription of appropriate intensity based on a simple diagnostic like the 4 min all-out test becomes crucial. Therefore, the determination of whether CF from the all-out test represents a boundary between localized steady and non-steady conditions is yet to be elucidated.
The 3 min all-out substitute for conventional CP determination was first introduced by Burnley et al. (2006) providing valid estimate of the maximal steady state in cycling. Most participants managed to complete 30 min of exercise at 15 W below the end-test power. In contrast, exercising at 15 W above the end-test power, blood lactate and O2 uptake rose inexorably until exhaustion, which occurred in approximately 13 ± 7 min. At a localized level, intermittent handgrip contractions at 15% and 30% under CF from the 5 min all-out test were sustained for 15 min, maintaining an apparent steady state of muscle-O2 saturation (StO2) (Hammer et al. 2020). Conversely, contractions at 15% and 30% above the CF led to time failure in 602 s and 342 s, respectively, accompanied by a progressive drop in StO2 (Hammer et al. 2020). However, conflicting research suggests that the 3 min all-out test either fails to provide accurate estimates of CP (Kalva et al. 2017), with a general tendency to overestimates (Bartram et al. 2017; Karsten et al. 2014). The reason for this discrepancy, likely rooted in the impossibility of sustaining maximal effort for extended periods (Dotan 2022), remains unexplored. Recent discussions ponder whether the CP concept reflects the upper boundary of metabolic steady state (Jones et al. 2019) or if it represents a distinct entity, deviating from the original theory that CP is the highest work rate sustainable without fatigue for an extended duration (Dotan 2022).
The boundary between the heavy and severe exercise intensity domain is considered to represent the transition between sustainable and unsustainable exercise intensity. Various concepts like maximal lactate steady state, respiratory compensation point, deoxy [heme] and StO2 localized threshold, and CP serve as markers for this transition. While these concepts share mechanistic principles, their alignment is often lacking. The proposed gray zone (Ozkaya et al. 2022) addresses the gap between commonly used maximal intensity thresholds with CP at the top end and maximal lactate steady state at the bottom end. While these thresholds all are correlated (Caen et al. 2022), they are not interchangeable. To address the boundary between sustainable and unsustainable exercise intensity in climbing-specific conditions, systemic variables (maximal lactate steady state, respiratory compensation point) have not proved valid (Baláš et al. 2021), and assessing localized muscle-O2 supply and metabolic O2 demands using NIRS (Hammer et al. 2020; Kirby et al. 2021) appears to be the only method to delineate forearm exercise intensity except for CF.
The use of the all-out test to determine CF of finger flexors in climbing is appealing due to its simplicity, however, this test differs from previous forearm all-out tests (Hammer et al. 2020; Kellawan and Tschakovsky 2014) by incorporating longer static contractions in the work:relief cycles and involving upper limb positions overhead, which may limit blood flow and O2 delivery. Moreover, during repeated 7 s contractions, fatigue associated with partial vascular occlusion may lead to a continuous drop in applied force within each contraction (Sadamoto et al. 1983), and the mean end-force might not represent the best estimate of CF.
Therefore, the study aimed to verify the concept of CF for finger flexors determined from the 4 min all-out test as a boundary for highest sustainable work intensity in sport climbers. In addition, the study seeks to explore, whether NIRS derived muscle oxygenation is useful in delineating this boundary. We hypothesized that CF, determined as the mean force from the last three contractions of the 4 min all-out test, overestimates the highest sustainable intensity in sport climbers. Furthermore, we expected that muscle-O2 dynamics would clearly delineate sustainable and non-sustainable exercise intensities of finger flexors.
Methods
Participants
Twelve intermediate to elite sport climbers (10 males and 2 females, 27.2 ± 7.4 years) volunteered to participate in this study. All participants were healthy nonsmokers, not taking any medications, and were required to refrain from strenuous physical activity 24 h before testing and caffeine 12 h prior to testing to prevent any potential ergogenic effects (Guest et al. 2021; Saraiva et al. 2023). They were instructed to maintain consistent activity, diet, and caffeine habits throughout the study. Anthropometric and training characteristics are detailed in Table 1. The study was approved by institutional Ethics Committee in accordance with the Declaration of Helsinki. All participants were informed of the risks of the experiment and signed an informed consent.
Design
Participants visited the laboratory five to six times separated by 3–6 days. During their first visit, they completed questionnaires concerning their ability level, climbing preferences and experience and undertook anthropometric measurements (body mass, height). After a warm-up procedure similar to that described by Baláš et al. (2016): 5 min of stair walking, 5 min mobilizing exercises, 5 min traversing on the climbing wall and 5 min individual intermittent hanging on wooden rung), participants completed the test of finger-flexor maximal voluntary contraction (MVC) and 4 min finger-flexor all-out test to determine CF. Subsequent visits involved participants performing finger-flexor contractions at various intensities, including CF, CF −2 kg, CF −4 kg, and CF −6 kg, for 12 min or until failure. An additional visit was conducted with CF −8 kg for a participant unable to sustain CF −6 kg.
Finger-flexor tests
All finger-flexor tests were conducted using a climbing-specific handgrip dynamometer (1D–SAC, Spacelab, Sofia, Bulgaria). Participants utilized a half-crimp grip position on a 23 mm deep wooden hold with 10 mm radius, excluding the thumb. Tests were performed in a standing position, with the dominant hand and arms at approximately 180° shoulder flexion, elbow slightly flexed. Participants were instructed to progressively transfer their weight (“hang”) on the wooden rung to develop as much force as possible or to attain the target force as quickly as possible. The detail-testing methodology is described elsewhere (Michailov et al. 2018).
Maximal finger-flexor strength
Maximal finger-flexor strength (in kg) was assessed through the MVC of the finger flexors, involving a 5 s hang on the wooden rung with the dominant hand. The highest peak value from the two trials was considered as maximal finger-flexor strength. The unit kg was used for all finger-strength measurements for easier interpretation of verification trials and comparisons with the original study on CF in climbing (Giles et al. 2021).
All-out test
The four-minute all-out test was conducted at a work:relief ratio of 7:3 s as proposed by Giles et al. (2021). During the work phase, participants were instructed to produce as much force as possible. During the relief phase, participants were allowed to shake their hand near the body to imitate real sport climbing conditions. In order to evaluate the CF, the mean force derived from the last 30 s of the test was defined (Kellawan and Tschakovsky 2014). Moreover, a decline in force is generally observed during the 7 s contractions. The mean force decrease from the last three contractions was labeled as ∆Fmax-min. In addition, the mean lowest force value from the last three contractions was referred as CFmin for further analysis. Impulse from all contractions (W) and impulse over the CF (W’) was calculated to approximate total muscle work and work related to energy store components (Bassan et al. 2019). Rate of force development (RFD) was calculated as the ratio between 50% peak force during a contraction and time to achieve it from the beginning of the contraction. The contraction times during the whole all-out test and last three contractions were computed to identify potential biases.
Verification of CF trials
To ensure the feasibility and tolerability of exercising at the CF intensity determined from the 4 min all-out test, a series of trials were conducted based on insights gained from previous piloting. Randomly assigned intensities, corresponding to CF or CF −2, −4, −6 kg, were applied during each of the four scheduled visits, all conducted at the same time of day. Participants were instructed to sustain intermittent finger-flexor 7:3 s contractions at the target intensity for 720 s or until failure. Following the completion of each trial, participants promptly provided their rate of perceived exertion (RPE) on a scale ranging from 6 to 20. The selection of a 720 s duration for the test was guided by previous piloting, considering that longer durations often resulted in mechanical discomfort from repetitive contractions. This factor was deemed significant, especially given that such discomfort is not commonly encountered during actual climbing due to frequent changes in grip positions. The highest force that participants were able to tolerate for 720 s was termed as CF720.
Near infrared spectroscopy
Muscle-O2 dynamics during all tests were assessed using a continuous wave near infrared spectroscopy (NIRS) device (Portamon, Artinis Medical System, BV, Netherlands). The device was placed over the belly of the flexor digitorum profundus of the dominant hand, following the protocol outlined by Fryer et al. (2018). To minimize optode movement during arm movement and limit ambient light penetration, the device was secured with bi-adhesive tape from the interior and black tape and a black sleeve from the exterior. StO2 was used to determine muscle-O2 dynamics during all tests. Specific metrics extracted from the all-out test included the rate of StO2 decrease during the first contraction (StO2 rate), maximal muscle-O2 desaturation (StO2 min), changes in StO2 during relief periods from intermittent contractions during last 30 s (three) contractions (Δ StO2 relief) and mean StO2 from the last 30 s (StO2 end) using 10 Hz sampling frequency. Notably, StO2 rate was computed as % StO2 decrease per second between 0.5 and 6.5 s of the first contraction to avoid possible signal noise at the beginning and the end of the contraction (Fig. 1). Data from verification trials were processed using a 10 s moving average (1 work-relief cycle), and parameters such as StO2 from the whole test (StO2 mean) and last 30 s of the test (StO2 end) were analyzed. In addition, the StO2-delayed slope (%/min) for the delayed phase after the initial drop in StO2 was calculated following the approach proposed by Kirby et al. (2021). Muscle-O2 balance, quantified through the StO2-delayed slope, establishes a dynamic physiologic threshold distinguishing between sustainable and unsustainable exercise, aligning with the concept of a “critical metabolic rate” and predicts depletion and repletion of finite work capacity and time to exhaustion (Kirby et al. 2021). However, the proposed initial starting time 60 s could not be used universally due longer time of the StO2 restoration in some participants and the starting point was determined visually as depicted at Fig. 2. In climbing-specific settings, StO2-delayed slope was successfully used to predict the time to exhaustion during sustained finger-flexor contraction (Gilic et al. 2023).

Illustrative example of the all-out test. Red-dashed line represents critical force (CF) determined by the mean force of last three contractions. Black-dashed line represents critical force (CFmin) determined as the mean of end-force from the last three contractions. The green curve represents muscle-oxygen saturation (StO2) changes during the first two contractions and relief cycles. The calculation of the StO2 decrease (StO2 rate—%/s) was performed using the middle 6 s part of the first 7 s contraction

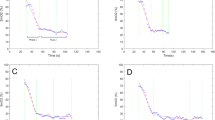
Illustrative examples of muscle-oxygen saturation (StO2) from aggregated StO2 signal (7 s contraction + 3 s rest) during the all-out tests and verification trials with examples of time periods for delayed slope calculations if the 60 s start-point was not used: a the only participant tolerating critical force (CF) for 720 s; b participant completing the whole verification trial at the intensity CF −4 kg; c participant completing the whole verification trial at the intensity CF-6 kg; d the only participant who was able to complete the whole verification trial at the intensity CF −8 kg
Statistical analysis
Descriptive statistics (mean ± SD) were used to characterize anthropometric, training, and performance characteristics in all climbers. The Shapiro–Wilk test and visual data inspection using Q–Q plots were conducted to assess data distribution for all variables. In instances where normal distribution was violated, non-parametric approaches were employed for inferential statistics. Differences between mean- and end-time and RFD at the beginning and end of the all-out tests were assessed using Wilcoxon signed-ranked test and paired t tests, respectively. The effect of intensity on muscle-O2 dynamics (StO2-delayed slope, StO2 mean, StO2 end during all-out and verification tests was assessed using repeated measure ANOVA with pairwise comparisons employing Bonferroni corrections. The assumption of sphericity was assessed using Mauchly’s test. In cases where the assumption was found to be significant, Huynh–Feldt adjustments were applied. To compare consistency between CF, CFmin and CF720, intraclass correlation coefficient (ICC) with 95% confidence interval (95%CI), repeated measures analysis of variance and limits of agreement with 95%CI were calculated. The association between climbing ability and selected variables was assessed using Pearson correlation coefficient. More specifically, the relationship between StO2 rate, CF and fatigue index was computed using linear regression. Cohen’s d for pairwise comparisons and partial eta squared (µp2) were used to assess effect size, statistical significance was set to P < 0.05.
Results
All-out test
All participants exhibited a plateau of mean force at the end of the all-out test (Fig. 1). CF, determined from the mean force of last three contractions, was measured at 20.1 ± 5.7 kg, representing 38.8 ± 8.8% of maximal finger-flexor strength. A noticeable drop in force during the 7 s contraction attained 8.1 ± 3.2 kg in the last three contractions, leading the CFmin to be 3.3 kg lower than CF (Table 2). The time of the contraction at the end of the test did not differ (P > 0.05) from the overall mean contraction time ranging around 6.6 s. (Table 2), however a significant decrease of RFD was observed from the start to the end of the test (P < 0.001; d = 1.65).
W and CF normalized to body mass exhibited significant (P < 0.05) relationships with climbing ability (R = 0.661 for both W and CF). W’ did not reach statistical significance (P > 0.05; R = 0.552). Notably, a stronger relationship to climbing ability was observed for CFmin (R = 0.704) and CF720 (R = 0.699) compared to CF. The StO2 rate explained 44% and 50% of the variability in CF and CF min, respectively, and exhibited a moderate correlation with the fatigue index (Fig. 3).

Relationship between muscle oxygen desaturation during the first 7 s contraction of the 4 min all-out test and a critical force (CF) normalized to body mass; b fatigue index calculated as % of initial force decrease
Verification trials
In the verification trials, the mean time to failure at CF was 440 ± 140 s, with only one participant completing the 720 s task. When the load was continuously lowered (−2 kg, −4 kg, and −6 kg), a greater number of participants (38%, 69%, and 92%, respectively) successfully completed the 720 s task. However, one participant achieved completion only with a load at CF −8 kg (67% of his CF) (Fig. 4).

a Mean (± SD) time to failure and rate of perceived exertion (RPE) for intensities at critical force (CF), CF-2 kg, CF−4 kg and CF −6 kg; b individual times to failure. Maximum test time was set to 720 s
CF 720 was found to be significantly lower (−20%, −4 kg; P < 0.001) than CF, with only moderate consistency (ICC = 0.691; 95%CI 0.245 to 0.899) between the two variables. Conversely, no significant differences (0.7 kg; P > 0.05) and excellent consistency (ICC = 0.912; 95%CI 0.735 to 0.974) were observed between CFmin and CF720. The limits of agreement are illustrated at Fig. 5.

Bland–Altman plots of mean differences (green line) between a critical force determined from the mean of the last three all-out test contractions (CF) and minimal force tolerable for 720 s (CF720); b critical force determined from the end-force of the last three all-out test contractions (CFmin) and CF720. Orange lines represent 95% limits of agreement
The StO2 end significantly increased from all-out test to CF−6 kg trial (P = 0.042, µp2 = 0.24). However, pairwise comparisons revealed the only significant difference between CF−6 kg and CF verification trials (6.6%; P = 0.011, d = 1.01). No other pairwise differences were observed for StO2 end (Fig. 6). In addition, the StO2 mean showed a significant increase from the all-out test to CF−6 kg trial (P = 0.006, µp2 = 0.27); however, no pairwise comparisons reached significance (P > 0.05) (Fig. 6). Finally, StO2-delayed slope did not exhibit statistically significant differences (P > 0.05) between verification trials due to high intraindividual variability, although trending to higher values with easier intensity (Fig. 6). In few participants, the StO2 development showed irregular drops or increases (Fig. 2b, c), likely due to incontrollable grip and arm positions changes. The mean StO2 end from the all-out was not related to values from the verification trials to failure at CF (−2.4 ± 7.5%; R = 0.444; P > 0.05) and often, lower StO2 end have been found during verification trials than during the all-out tests (Fig. 2b, c, d). Contrary, in the only participant completing the whole 720 s-long verification trial at CF near exhaustion (RPE = 19), the StO2 end was 13% higher at the exhaustive verification trial than during the all-out test (Fig. 2a).

a Mean (± SD) and b individual muscle-oxygen saturation (StO2) from the whole test (StO2 mean); c, d from the last 30 s (StO2 end) of each test; and e, f delayed StO2 slope from all verification trials at the working intensities at the critical force (CF), CF−2 kg, CF−4 kg and CF −6 kg. * indicates significant (P < 0.05) differences
Discussion
The study reveals several key findings: 1) CF determined as the mean force from the last three contractions of the 4 min all-out test fails to predict the highest sustainable work rate of forearm flexors; 2) CFmin determined as the end-force of the last three contractions shows a stronger correlation with sustainable work rate and better predicts sport climbing ability; 3) the initial-StO2 rate during the all-out test is closely related to CF and inversely related to the fatigue index; 4) mean values or delayed slope of StO2 are not sensitive enough to discriminate intermittent finger-flexor contractions at intensities ranging from ~ 0–40% below CF in a sport-specific setting.
Despite the widespread use of the 4 min all-out test, our study does not support its predictive validity for sustainable exercise intensity, aligning with current research trends (Bartram et al. 2017; Bergstrom et al. 2013; Karsten et al. 2014). Research indicates that exercises at CP /speed intensity typically last from 15 to 25 min, occasionally extending to 45–60 min (Dotan 2022; Jones et al. 2019). In our study, the mean exercise time to exhaustion at CF was ~ 7 min. However, Jones et al. (2019) discourage the verification of the CP concept by exercising at CP intensity due to potential reliability errors in CP determination. Therefore, we employed four intensities at and below CF, using 2 kg as minimal, practically distinguishing intensity steps to monitor exercise sustainability, RPE, and muscle-O2 dynamics. This choice was based on previous reliability data for the forearm flexor 4 min all-out test (Giles et al. 2021; McClean et al. 2023).
Initially, Giles et al. (2021) reported excellent test–retest reliability (ICC = 0.96, limits of agreement = −2.45 to 2.4 kg) for a small sample size. However, a recent study by McClean et al. (2023) with a similar population to ours, revealed lower consistency (ICC = 0.848, CV = 21%) The precision of the test for determining CF was questioned due to significant interindividual variability in the latter study. The only divergence from the initial Giles et al. study (2021) was the allowance of lowering the arm during relief periods, similar to our study, enhancing blood flow, muscle-O2 recovery, and performance (Baláš et al. 2016). This modification likely increased CF during the all-out test, however, the effect on reliability is not obvious. The high-interindividual variability in determining CF may be attributed to low hangboarding experience in participants with substantial test–retest CF variability. Familiarization with the exhaustive protocol seems necessary for obtaining reliable data. Although all participants in our study were familiar with the all-out test, we acknowledge the potential reliability error in data interpretation. Considering an ICC of 0.848 and an SD of CF in our sample (SD = 5.7 kg), the standard error of measurement is 2.2 kg, implying that the all-out test may over- or underestimate CF with this value within ~ 68% of the population.
Our results reveal no underestimation of CF. The participant who completed the 720 s CF trial was nearly exhausted at the end. Even considering the reliability error, the intensity of CF −4 kg should be sustainable for nearly all participants, yet only 69% completed the 720 s trial, and the mean RPE was only slightly lower than during the CF trial (18.3 vs 16.3). A significant drop in RPE was observed at CF −6 kg (RPE = 13.8). RPE is generally lower for localized than for whole-body exercise, and research indicates the RPE for the transition between sustainable and non-sustainable climbing to be ~ 14 on the 6–20 scale (Baláš et al. 2022). This suggests that CF, calculated as the mean force from the end of the test, overestimates CF as an indicator of the transition between sustainable and non-sustainable hangboard exercise. Our findings contradict previous forearm studies using the 10 min and 5 min all-out tests to determine CF, which clearly distinguished sustainable and non-sustainable tasks (Hammer et al. 2020; Kellawan and Tschakovsky 2014).
The length of the all-out protocol, particularly the ratio of work-relief cycles, may contribute to these discrepancies. Previous studies utilized short isometric contractions with 1:2 s and 1.5:1.5 s work:relief cycles, respectively (Hammer et al. 2020; Kellawan and Tschakovsky 2014). In such short contractions, there is no force decrease within a contraction, and blood flow restriction is likely smaller compared to longer contraction as showed previously (Broxterman et al. 2014). Partial vascular occlusion begins at ~ 20% of MVC, while full blood occlusion is observed at ~ 50–75% of MVC during handgrip sustained contractions (Barnes 1980; Bergua et al. 2020). Consequently, O2 delivery is highly limited during all-out contractions and predominantly occurs in the short relief periods between contractions.
The primary limitation of intermittent hangboard performance appears to be O2 delivery rather than O2 extraction, as suggested in handgrip exercise with varying work:relief cycles and intensities (Broxterman et al. 2014; Hammer et al. 2020). Enhanced O2 extraction likely compensates for reduced O2 delivery even during low-intensity exercise, explaining the lack of significant differences in StO2 dynamics between all-out tests and verification trials with decreasing intensity in our study. For instance, the StO2-delayed slope could not distinguish exhaustive from non-exhaustive trials. Arm movement during relief periods was allowed, and participants, with fatigue, could instinctively change their grip and arm position, affecting forearm flexor involvement (Schweizer and Hudek 2011). These factors are inherent in real climbing conditions and challenging to control even in a standardized setting. Consequently, we observed more or less pronounced waves during the StO2-delayed slope (Fig. 2), making the interpretation of StO2 data less straightforward. Moreover, the placement of optodes on small forearm muscles may pose an additional challenge compared to voluminous muscles like the vastus lateralis, and even slight rotations of forearm muscles may alter muscle architecture under optodes and StO2 responses.
Although StO2 end did not differ between all-out tests and exhaustive verification trials at CF, suggesting that the lowest StO2 values can predict exhaustion, caution should be exercised due to large intraindividual variability. This is likely attributed to the low reliability of StO2 end during exhaustive forearm flexor tasks (ICC = 0.437, CV = 23.5%) (Baláš et al. 2018). On the other hand, there was a consistent increase in StO2 end from CF to CF−6 kg trials, reaching statistical and practical significance at CF−6 kg (+ 6.6% StO2 end increase). CF−6 kg might represent a group threshold for sustainable and non-sustainable exercise based on O2 dynamics. However, individual increases of StO2 end are not as evident as the whole group means. In summary, due to numerous confounding factors, NIRS may not be sensitive enough to distinguish between steady and non-steady state conditions in climbing-specific conditions at intensities up to 40% below CF.
Another NIRS indicator, the StO2 rate from the beginning of the all-out test, exhibited a close association with CF and an inverse relationship with the fatigue index, calculated as the percentage of force decrease during the test. The rapid decrease in StO2 implies a higher rate of muscle-O2 extraction, given the absence of changes in blood volume expected during the initial maximal forearm contraction overhead, leading to vascular occlusion. Faster O2 extraction is possibly linked to increased mitochondrial respiration capacity, justifying its association with CF, even though it lacks the O2 delivery component (Cardinale et al. 2019). Therefore, we propose considering the initial-StO2 rate during the all-out test as an additional variable when assessing CF and localized endurance of finger flexors.
The force decrease during each contraction is another factor differing from previous handgrip all-out tests, where no decrease during short contractions was reported (Broxterman et al. 2014; Hammer et al. 2020; Kellawan and Tschakovsky 2014). We observed an ~ 8 kg-force decrease during the last three contractions. Therefore, we tested whether the end-force might better estimate sustainable intensity. It was shown that CF min was in excellent agreement with CF 720. Moreover, it more precisely predicted lead climbing ability and was more related to StO2 rate than CF. All this suggests that the end-force from the last contractions likely more precisely reflects the threshold between sustainable and non-sustainable isometric exercise. However, larger sample size is needed to verify this hypothesis.
RFD significantly decreases during the all-out test, with the initial RFD dropping to half of its values by the end. While this information was not initially part of the objectives and was analyzed to monitor the length and course of each contraction, it is interesting to note. Although not presented, the drop in RFD was not associated with any O2 dynamics variables, and due to the low sample size, no assessment of the effect of training status or ability could be performed. Both RFD and force variation during contraction have been linked to specific forearm muscle adaptations in boulder and lead climbers (Fanchini et al. 2013; Limonta et al. 2016). Therefore, these parameters may be further explored to assess neuromuscular fatigue in various ability groups of climbers.
Several limitations and strengths need to be acknowledged. First, the recruited sample size was limited, raising questions about the generalizability of the findings. In addition, testing was conducted throughout different menstrual cycles in two female climbers, which may have contributed to higher variability in strength outcomes (Weidauer et al. 2020). However, within this heterogeneous group of climbers, both time to exhaustion and NIRS responses consistently indicated an overestimation of CF. Furthermore, verification trials employed an absolute load of 2 kg, representing the minimal step, resulting in a slightly varied relative individual intensity under CF for different participants. This pragmatic approach aligns with the feasibility of the study and common practices in hangboard training, where intensity is adjusted by adding or subtracting free weight (Torr et al. 2022). The handgrip contractions were conducted in an ecological setting, enhancing ecological validity while reducing control over all variables (Michailov et al. 2018). This may have contributed to the fluctuation of NIRS signal and reliability of the tests.
Conclusions
Our study challenges the conventional use of CF derived from the 4 min all-out test for forearm flexors. CF, based on the mean force from the last three contractions, does not predict the highest sustainable work rate reliably.
In contrast, determining CF as the end-force of the last three contractions shows a stronger link to sustainable work rate and better predicts sport climbing ability. Focusing on end-force measurement may provide a more accurate representation of sustained effort capacity in climbing.
The initial-StO2 rate during the all-out test correlates closely with CF and inversely with the fatigue index, indicating its potential utility in understanding metabolic demands and fatigue resistance during climbing-specific tasks. However, caution is needed in interpreting mean values or slopes of StO2 as discriminatory tools for intermittent finger-flexor contractions around 0–40% below CF in a sport-specific context. Our findings suggest that these conventional metrics may lack the sensitivity required to distinguish nuanced metabolic responses during climbing-related tasks.
Data availability
The datasets generated during in the current study are available as Electronic supplementary material.
Abbreviations
- ANOVA:
-
Analysis of variance
- CI:
-
Confidence interval
- CF:
-
Critical force calculated as the mean force from the last three contractions
- CF720 :
-
Critical force calculated as the highest force that participants were able to tolerate for 720 s
- CFmin :
-
Critical force calculated as end-force from the last three contractions
- CP:
-
Critical power
- CV:
-
Coefficient of variation
- ICC:
-
Intraclass correlation coefficient
- MVC:
-
Maximal voluntary contraction
- NIRS:
-
Near-infra red spectroscopy
- R:
-
Pearson correlation coefficient
- R2 :
-
Coefficient of determination
- RPE:
-
Rate of perceived exertion
- O2 :
-
Oxygen
- SD:
-
Standard deviation
- StO2 :
-
Muscle oxygen saturation
- W:
-
Impulse from all contractions in the all-out test
- W’:
-
Impulse from all contractions in the all-out test over the critical force
- RFD:
-
Rate of force development
References
Baláš J, Michailov M, Giles D, Kodejška J, Panáčková M, Fryer S (2016) Active recovery of the finger flexors enhances intermittent handgrip performance in rock climbers. Eur J Sport Sci 16(7):764–772. https://doi.org/10.1080/17461391.2015.1119198
Baláš J, Kodejška J, Krupková D, Hannsmann J, Fryer S (2018) Reliability of near-infrared spectroscopy for measuring intermittent handgrip contractions in sport climbers. J Strength Cond Res 32(2):494–501
Baláš J, Gajdošík J, Giles D, Fryer S, Krupková D, Brtník T, Feldmann A (2021) Isolated finger flexor vs. exhaustive whole-body climbing tests? How to assess endurance in sport climbers? Eur J Appl Physiol 121(5):1337–1348. https://doi.org/10.1007/s00421-021-04595-7
Baláš J, Gajdošík J, Giles D, Fryer S (2022) The estimation of critical angle in climbing as a measure of maximal metabolic steady state. Front Physiol 12:2350
Barnes WS (1980) The relationship between maximum isometric strength and intramuscular circulatory occlusion. Ergon 23(4):351–357. https://doi.org/10.1080/00140138008924748
Bartram JC, Thewlis D, Martin DT, Norton KI (2017) Predicting critical power in elite cyclists: questioning the validity of the 3 minute all-out test. Int J Sports Physiol Perform 12(6):783–787. https://doi.org/10.1123/ijspp.2016-0376
Bassan ND, Denadai BS, de Lima LCR, Caritá RAC, Abdalla LHP, Greco CC (2019) Effects of resistance training on impulse above end-test torque and muscle fatigue. Exp Physiol 104(7):1115–1125. https://doi.org/10.1113/ep087204
Bergstrom HC, Housh TJ, Zuniga JM, Traylor DA, Lewis RW, Camic CL, Johnson GO (2013) Responses during exhaustive exercise at critical power determined from the 3 min all-out test. J Sports Sci 31(5):537–545. https://doi.org/10.1080/02640414.2012.738925
Bergua P, Montero-Marin J, Gomez-Bruton A, Casajús JA (2020) The finger flexors occlusion threshold in sport-climbers: an exploratory study on its indirect approximation. Eur J Sport Sci. https://doi.org/10.1080/17461391.2020.1827047
Broxterman RM, Ade CJ, Wilcox SL, Schlup SJ, Craig JC, Barstow TJ (2014) Influence of duty cycle on the power-duration relationship: observations and potential mechanisms. Respir Physiol Neurobiol 192:102–111. https://doi.org/10.1016/j.resp.2013.11.010
Burnley M, Doust JH, Vanhatalo A (2006) A 3 min all-out test to determine peak oxygen uptake and the maximal steady state. Med Sci Sports Exerc 38(11):1995–2003. https://doi.org/10.1249/01.mss.0000232024.06114.a6
Caen K, Bourgois JG, Stassijns E, Boone J (2022) A longitudinal study on the interchangeable use of whole-body and local exercise thresholds in cycling. Eur J Appl Physiol 122(7):1657–1670. https://doi.org/10.1007/s00421-022-04942-2
Cardinale DA, Larsen FJ, Jensen-Urstad M, Rullman E, Sondergaard H, Morales-Alamo D, Boushel R (2019) Muscle mass and inspired oxygen influence oxygen extraction at maximal exercise: role of mitochondrial oxygen affinity. Acta Physiol. https://doi.org/10.1111/apha.13110
Dotan R (2022) A critical review of critical power. Eur J Appl Physiol 122(7):1559–1588. https://doi.org/10.1007/s00421-022-04922-6
Fanchini M, Violette F, Impellizzeri FM, Maffiuletti NA (2013) Differences in climbing-specific strength between boulder and lead rock climbers. J Strength Cond Res 27(2):310–314. https://doi.org/10.1519/JSC.0b013e3182577026
Fryer S, Stoner L, Lucero A, Witter T, Scarrott C, Dickson T, Draper N (2015) Haemodynamic kinetics and intermittent finger flexor performance in rock climbers. Int J Sports Med 36(2):137–142. https://doi.org/10.1055/s-0034-1385887
Fryer S, Giles D, Palomino IG, Puerta AD, España-Romero V (2018) Hemodynamic and cardiorespiratory predictors of sport rock climbing performance. J Strength Cond Res 32(12):3534–3541. https://doi.org/10.1519/jsc.0000000000001860
Giles D, Chidley JB, Taylor N, Torr O, Hadley J, Randall T, Fryer S (2019) The determination of finger-flexor critical force in rock climbers. Int J Sports Physiol Perform 14(7):972–979. https://doi.org/10.1123/ijspp.2018-0809
Giles D, Hartley C, Maslen H, Hadley J, Taylor N, Torr O, Fryer S (2021) An all-out test to determine finger flexor critical force in rock climbers. Int J Sports Physiol Perform 16(7):942–949. https://doi.org/10.1123/ijspp.2020-0637
Gilic B, Feldmann A, Vrdoljak D, Sekulic D (2023) Forearm muscle oxygenation and blood volume parameters during sustained contraction performance in youth sport climbers. J Sports Med Phys Fitness 63(7):819–827. https://doi.org/10.23736/s0022-4707.23.14806-7
Guest NS, VanDusseldorp TA, Nelson MT, Grgic J, Schoenfeld BJ, Jenkins NDM, Campbell BI (2021) International society of sports nutrition position stand: caffeine and exercise performance. J Int Soc of Sports Nutr. https://doi.org/10.1186/s12970-020-00383-4
Hammer SM, Alexander AM, Didier KD, Huckaby LM, Barstow TJ (2020) Limb blood flow and muscle oxygenation responses during handgrip exercise above vs. below critical force. Microvasc Res. https://doi.org/10.1016/j.mvr.2020.104002
Jones AM, Burnley M, Black MI, Poole DC, Vanhatalo A (2019) The maximal metabolic steady state: redefining the “gold standard.” Physiol Reports. https://doi.org/10.14814/phy2.14098
Kalva CA, Zagatto AM, da Silva AS, de Araújo MYC, de Almeida PB, Papoti M (2017) Tethered 3-min all-out test did not predict the traditional critical force parameters in inexperienced swimmers. J Sports Med Phys Fitness 57(9):1126–1131. https://doi.org/10.23736/s0022-4707.16.06461-6
Karsten B, Jobson SA, Hopker J, Passfield L, Beedie C (2014) The 3-min test does not provide a valid measure of critical power using the SRM isokinetic mode. Int J Sports Med 35(4):304–309. https://doi.org/10.1055/s-0033-1349093
Kellawan JM, Tschakovsky ME (2014) The single-bout forearm critical force test: a new method to establish forearm aerobic metabolic exercise intensity and capacity. PLoS ONE. https://doi.org/10.1371/journal.pone.0093481
Kirby BS, Clark DA, Bradley EM, Wilkins BW (2021) The balance of muscle oxygen supply and demand reveals critical metabolic rate and predicts time to exhaustion. J Appl Physiol 130(6):1915–1927. https://doi.org/10.1152/japplphysiol.00058.2021
Langer K, Simon C, Wiemeyer J (2023) Physical performance testing in climbing—a systematic review. Front Sports Act Living. https://doi.org/10.3389/fspor.2023.1130812
Levernier G, Laffaye G (2019) Four weeks of finger grip training increases the rate of force development and the maximal force in elite and top world ranking climbers. J Strength Cond Res 33(9):2471–2480. https://doi.org/10.1519/jsc.0000000000002230
Limonta E, Ce E, Gobbo M, Veicsteinas A, Orizio C, Esposito F (2016) Motor unit activation strategy during a sustained isometric contraction of finger flexor muscles in elite climbers. J Sports Sci 34(2):133–142. https://doi.org/10.1080/02640414.2015.1035738
Maciejczyk M, Michailov ML, Wiecek M, Szymura J, Rokowski R, Szygula Z, Beneke R (2022) Climbing-specific exercise tests: energy system contributions and relationships with sport performance. Front Physiol. https://doi.org/10.3389/fphys.2021.787902
McClean ZJ, MacDougall KB, Fletcher JR, Aboodarda SJ, Macintosh BR (2023) Test-retest reliability of a 4 minute all-out critical force test in rock climbers. Int J Exerc Sci 16(4):912–923
Medernach JPJ, Kleinoder H, Lotzerich HHH (2015) Fingerboard in competitive bouldering: training effects on grip strength and endurance. J Strength Cond Res 29(8):2286–2295. https://doi.org/10.1519/jsc.0000000000000873
Michailov M, Baláš J, Tanev SK, Andonov HS, Kodejška J, Brown L (2018) Reliability and validity of finger strength and endurance measurements in rock climbing. Res Q Exerc Sport 89(2):246–254. https://doi.org/10.1080/02701367.2018.1441484
Ozkaya O, Balci GA, As H, Cabuk R, Norouzi M (2022) Grey zone: a gap between heavy and severe exercise domain. J Strength Cond Res 36(1):113–120. https://doi.org/10.1519/jsc.0000000000003427
Poole DC, Burnley M, Vanhatalo A, Rossiter HB, Jones AM (2016) Critical power: an important fatigue threshold in exercise physiology. Med Sci Sports Exerc 48(11):2320–2334. https://doi.org/10.1249/mss.0000000000000939
Sadamoto T, Bondepetersen F, Suzuki Y (1983) Skeletal muscle tension, flow, pressure, and EMG during sustained isometric contractions in humans. Eur J Appl Physiol 51(3):395–408. https://doi.org/10.1007/bf00429076
Saraiva SM, Jacinto TA, Gonçalves AC, Gaspar D, Silva LR (2023) Overview of caffeine effects on human health and emerging delivery strategies. Pharm. https://doi.org/10.3390/ph16081067
Schweizer A, Hudek R (2011) Kinetics of Crimp and Slope Grip in Rock Climbing. J Appl Biomech 27(2):116–121
Stien N, Saeterbakken AH, Andersen V (2022) Tests and procedures for measuring endurance, strength, and power in climbing-a mini-review. Front Sports and Act Living. https://doi.org/10.3389/fspor.2022.847447
Torr O, Randall T, Knowles R, Giles D, Atkins S (2022) Reliability and validity of a method for the assessment of sport rock climbers’ isometric finger strength. J Strength Cond Res 36(8):2277–2282. https://doi.org/10.1519/jsc.0000000000003548
Vigouroux L, Quaine F (2006) Fingertip force and electromyography of finger flexor muscles during a prolonged intermittent exercise in elite climbers and sedentary individuals. J Sports Sci 24(2):181–186
Weidauer L, Zwart MB, Clapper J, Albert J, Vukovich M, Specker B (2020) Neuromuscular performance changes throughout the menstrual cycle in physically active females. J Musculoskelet Neuronal Interact 20(3):314–324
Funding
Open access publishing supported by the National Technical Library in Prague. This work was supported by Charles University Program Cooperatio—Sport Sciences—Biomedical & Rehabilitation Medicine.
Author information
Authors and Affiliations
Contributions
JB and JG conceived and designed the research; JG, JB conducted experiments; JB and JG analyzed and evaluated data; JB, TJ, PB, AF prepared the manuscript. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare and assert that the results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. The authors declare no conflict of interest.
Additional information
Communicated by Guido Ferretti.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jiří, B., Jan, G., Tomáš, J. et al. Measuring critical force in sport climbers: a validation study of the 4 min all-out test on finger flexors. Eur J Appl Physiol (2024). https://doi.org/10.1007/s00421-024-05490-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00421-024-05490-7