
Abstract
Maximal oxygen uptake (VO2max) is associated with cardiovascular and metabolic health in the general population. The heart rate (HR) ratio method (HRratio) is a valid, easy and accessible method for estimating VO2max in well-trained subjects. This study examined the validity of using the HRratio to estimate VO2max in recreational football players in the untrained and trained states. Sixty-six participants (age 39.3 ± 5.8 years) were tested pre-training and 28 after 12 weeks, for VO2max assessment, running on a treadmill alternating speed (1 km h−1) and inclination (1%) increments every 30 s until exhaustion. Maximal HR (HRmax) was assessed directly with a multiple approach and estimated with selected equations. Resting HR (HRrest) was measured in supine position, after 15 min of rest. The HRratio method considers the product of HRmax/HRrest ratio by a theoretical proportionality factor (15 ml kg−1 min−1, TPF) to estimate VO2max. This population-specific proportionality factor (SPF) was 14.6 ± 2.6 ml kg−1 min−1. In the untrained state (n = 66), participants’ actual VO2max (41.3 ± 6.2 ml kg−1 min−1) was moderately lower (~ 2 ml kg−1 min−1) than the estimated VO2max using the TPF. A nonsignificant difference (0.7 ml kg−1 min−1) was found when the VO2max was estimated using the SPF. When using HRmax equations and the TPF, a small nonsignificant difference (~ 1.5 ml kg−1 min−1) was reported between actual and estimated VO2max. In the trained state (n = 28), the estimated VO2max values were not significantly different from the actual VO2max (44.2 ± 5.2 ml kg−1 min−1), with large effect sizes when considering TPF and estimated HRmax. The results of this study provide evidence of the applicability of HRratio in estimating VO2max in male adult/middle-aged recreational football players.
Similar content being viewed by others

Introduction
Maximal oxygen uptake (VO2max) is the best measure of cardiorespiratory fitness and is associated with cardiovascular and metabolic health in the general population (Liff et al. 2020; Diaz-Canestro and Montero 2019). Higher levels of VO2max are related to a lower risk of cardiovascular events and all-cause mortality (Nes et al. 2014; Zeiher et al. 2019). Interestingly, in the COVID-19 outbreak VO2max was indicated as a variable for estimating patients’ global physiological reserves (Ahmed 2020). In fact, individual levels of VO2max were suggested for identifying patients’ ability to tolerate intensive care admission and post-admission rehabilitation programmes and as a clinically relevant triage parameter during the COVID-19 emergency (Ahmed 2020). Given the supposed relevance of individual VO2max for guiding treatments in critical health conditions in the general population, easily accessible assessment strategies might have a great impact on public healthcare (Ahmed 2020; Liff et al. 2020).
Cardiopulmonary exercise testing (CPET) is currently the reference for assessing patients’ VO2max (Liff et al. 2020; Nes et al. 2014; Diaz-Canestro and Montero 2019; Zeiher et al. 2019). Unfortunately, the need for skilled personnel, specific expensive devices and individual testing in certified laboratories limits the accessibility of CPET for the general population (Castagna et al. 2020).
The impact of VO2max on fitness and health promoted the interest in valid, reliable and sustainable alternative methods to CPET to estimate VO2max. Field testing, namely the Yo–Yo intermittent tests, were recently proposed as valid, reliable and practically sustainable tools for estimating individual VO2max in recreational football players (Castagna et al. 2020; Póvoas et al. 2019a). However, CPET and field tests both require participants’ maximal effort to obtain valid and satisfactory VO2max estimates. Exhaustive efforts may represent a concern when patients enroll in a training intervention if they have a previous inactive or untrained status and in the presence of chronic morbidity(ies). Alternatively, submaximal field testing may represent a valid and reliable surrogate for exhaustive testing (Póvoas et al. 2019a). However, patients may experience difficulties in adapting to submaximal testing given their reduced familiarisation with testing and their current fitness and health status. Furthermore, inter-individual fitness variability may reduce the validity of the submaximal design of the proposed protocol (Póvoas et al. 2018, 2019a).
With the aim of limiting the constraints associated with exercise testing involving either maximal or submaximal effort, alternative procedures for estimating VO2max were developed. Uth et al. (2004) and Uth (2005) suggested a heart rate (HR)-based procedure for estimating VO2max in well-trained male and female subjects. The proposed method provided practically acceptable estimates of individual VO2max values resulting from the product of a theoretical factor (i.e. 15 ml kg−1 min−1) and subjects’ maximal HR (HRmax) and resting HR (HRrest) ratio (Uth et al. 2004). Popular predictive equations for estimating individual HRmax values were examined with the aim of promoting use of this HR-based (HRratio) procedure (Uth 2005; Uth et al. 2004). However, the reported data were obtained with descriptive studies examining well-trained subjects. The above premises and the procedural simplicity of the proposed HRratio method warrant extending the research to studies with populations of untrained subjects submitted to exercise interventions (Ahmed 2020).
Recreational football has been reported as providing clinically relevant (3.5 ml kg−1 min−1) VO2max improvements in untrained participants (Milanovic et al. 2018). This is across ages, gender and health conditions with limited weekly participation (i.e. ~ 2 training sessions per week) and short-term exposure (10–16 weeks) (Milanovic et al. 2015, 2018). Periodical evaluation of aerobic fitness was suggested to control and regulate the effectiveness of recreational football interventions (Castagna et al. 2020). In this regard, the HRratio VO2max estimating method may be of great practical interest for guiding recreational football interventions. Furthermore, the reported training-induced variations in HRrest and HRmax usually associated with VO2max improvements promote assessment of the predictive validity of the HRratio method during training interventions (Póvoas et al. 2019a, 2019b; Uth et al. 2004).
The aim of this study was; therefore, to examine the applicability of an HRratio method for estimating VO2max in male subjects participating in a recreational football intervention in the trained and untrained states. Method validity and measurements agreement were assumed as applicability construct.
Methods
Participants
In this study, 66 untrained male adults (age 39.3 ± 5.8 years, body mass 81.9 ± 10.8 kg, stature 173.2 ± 6.4 cm) involved in a recreational football training intervention volunteered to participate. The untrained state was defined as the participants having less than 20 min of exercise on 3 or more days a week (Church et al. 2010). Medical clearance for participation was obtained before the commencement of any of this study procedures. All the participants were familiarised with the procedures used in this investigation during the two weeks before the start of the study, performing submaximal versions of the treadmill test for VO2max assessment and the Yo–Yo intermittent tests. The participants gave their written informed consent to participate in the study, which was conducted in accordance with the Declaration of Helsinki and ethical approval was provided by the local Institutional Review Board before commencement of the study data collection. All participants were informed of the risks and benefits of participation and made aware that they could withdraw from the study at any time without penalty.
Design
The HRratio method assumes a linear association between body mass specific VO2max (i.e. ml kg−1 min−1) and HRmax and HRrest (Uth et al. 2004). Estimation of VO2max results from the multiplication of the HRmax and HRrest ratio by a theoretical proportionality factor (TPF), assumed as 15 ml kg−1 min−1. Descriptive studies carried out with well-trained (7–9 h of weekly exercise) male (60.9 ± 5.5 ml kg−1 min−1) and female (50.4 ± 6.9 ml kg−1 min−1) participants found a PF of 14.5 ± 1.2 and 15.3 ± 0.7 ml kg−1 min−1, respectively (Uth et al. 2004; Uth 2005). In this study, PF, HRrest and HRmax were evaluated, in male untrained participants who volunteered to participate in a 12-week recreational football intervention, at baseline (n = 66) and post-intervention (n = 28), i.e. in the untrained and trained states. It was only possible to evaluate all the procedures considered in this study to assess the individual HRmax at the end of the recreational football intervention, i.e. in the trained state, in 28 out of the initial 66 participants (Póvoas et al. 2019b). The resulting VO2max values were compared considering either the population-specific proportionality factor (SPF; 14.6 ± 2.6 ml kg−1 min−1) or the TPF (i.e. 15 ml kg−1 min−1). Agreement between measures was assessed by comparing estimated and actual VO2max values across the intervention using either actual HRmax or estimated HRmax. Participants’ HRmax was assessed using a multiple approach to ensure assessment accuracy (Póvoas et al. 2019b). Population-specific equations were used to obtain estimated HRmax (Póvoas et al. 2020). With the aim to test the population validity of the HRratio method, the participants’ actual VO2max was estimated dividing the HRmax assessed either with the multiple approach or estimated with population valid equations by HRrest. The obtained HRratio was then multiplied by the TPF (15 ml kg−1 min−1) or the SPF for comparisons.
The recreational football intervention, consisted of 2–3 60-min weekly training sessions in the form of 45-min small-sided games played on an artificial pitch (7v7; 43 × 27 m pitch, 83 m2 per player).
Testing procedures
The participants’ HRmax was assessed using the procedures suggested by Póvoas et al. (2019b). This procedure considered HRmax as the highest value across a treadmill test until exhaustion (TT), field tests (i.e. Yo–Yo intermittent tests) and football matches played by the participants during the recreational football intervention. The field tests were performed at the same time of day, on the same artificial pitch, wearing the same footwear and under neutral environmental conditions. Before the field tests, the participants performed a standardised warm-up consisting of 10 min of running at different intensities including changes of direction. The field and TT tests were performed in a random order with at least a 4-day recovery period in between. No vigorous physical activity was performed on the day before the test procedures took place. Resting HR was measured in a quiet room at a constant temperature, with the participant in a supine position, after 15 min of rest. According to the evidence provided in recreational football interventions, estimations of individual HRmax were performed using the 211 − 0.64 × age and 226 − age equations (Póvoas et al. 2020; Warburton et al. 2006; Nes et al. 2013).
The TT (HP Cosmos Quasar, Nussdorf, Germany) consisted of 3 min of walking at 5 km h−1 and 2 min of running at 8 km h−1, with 0% inclination and then alternating between increases in speed (1 km h−1) and inclination (1%) every 30 s until voluntary exhaustion. Expired respiratory gas fractions were measured using an open-circuit breath-by-breath automated gas analysis system (Quark CPET, Cosmed, Rome, Italy). Attainment of VO2max was assumed when participants achieved a plateau in VO2 despite an increase in exercise intensity and at least one of the following criteria: a respiratory exchange ratio (RER) greater than 1.10 and RPE equal to or higher than 7 (Midgley et al. 2006, 2007). The highest 15-s VO2 during the final stages of the test was considered as the individual VO2max (Midgley et al. 2006, 2007). Data analysis was performed with manual inspection of each TT data file using an Excel file (Microsoft, Redmont, USA). The average TT duration was within the range suggested for VO2max assessment (10.7 ± 1.5 min; 95% CI 9.8–10.7) (Midgley et al. 2006, 2007). Post-test verification was performed for metabolic computations to correct gas analyser drift bias (Garcia-Tabar et al. 2015).
All exercise HRs were recorded in 1-s intervals using Polar Team System 2 HR monitors (Polar Electro Oy, Kempele, Finland). The participants were acquainted with the use of HR monitors in advance. The participants were allowed to drink water ad libitum to ensure proper hydration during all the exercise conditions considered in this study.
Statistical analyses
Results are expressed as means ± standard deviations, 95% confidence intervals (95% CI) and ranges when appropriate. Normality assumption was verified using the Shapiro–Wilk W test. An one-way repeated-measurements analysis of variance (ANOVA) with post hoc Least Significant Difference test was used to compare VO2max values across the considered estimation methods. Practical differences were assessed as partial eta squared (η2p) and magnitudes rated as follows: η2p ≥ 0.14 large effect, 0.14 > η2p ≥ 0.06 medium effect, 0.06 > η2p ≥ 0.01 small effect and η2p < 0.01 trivial effect (Bakeman 2005). Pearson correlation (r) was used to assess the associations between variables. The magnitude of the reported effects was described using the Hopkins et al. (2009) criteria and the Cook’s distance analysis was considered to detect possible influential outliers. The Cohen’s d was used to evaluate the effect size, with values above 0.8, between 0.8 and 0.5, between 0.5 and 0.2 and lower than 0.2 considered as large, moderate, small and trivial, respectively (Cohen 1988). Measurement agreement was assessed using the Bland and Altman approach (Bland and Altman 1986). Significance was set at 5% (p < 0.05).
Results
Pre-intervention
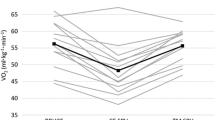
Pre-intervention HRmax and HRrest values were 189 ± 8 beats min−1 (187–191) and 68 ± 12 beats min−1 (65–71), respectively. The average baseline SPF value was 14.6 ± 2.6 ml kg−1 min−1 (13.9–15.2). The participants’ actual VO2max was significantly different from the VO2max (+ 0.6 ml kg−1 min−1, ~ 2%, p = 0.01) estimated using the theoretical TPF (i.e. VO2max EstTPF, TPF = 15) and VO2max (− 1.9 ml kg−1 min−1, ~ 5%, p = 0.01) assessed considering the theoretical HRmax equation (i.e. 211 − 0.64 × age, VO2max EstNes) with a medium effect (Table 1). Nonsignificant small differences were reported between VO2max EstWar (i.e. HRmax using the 226 − age equation), VO2max NesTPF (using the 211 − 0.64 × age equation and 15 as PF), VO2max WarTPF (using the 226 − age equation and 15 as PF) and actual VO2max values. A trivial nonsignificant difference between VO2max Est (using the SPF) and actual VO2max was found.
A moderate and significant (p = 0.008) association was found between pre-intervention VO2max and HRrest (r = − 0.33, from − 0.52 to − 0.09). Pre-intervention HRmax and VO2max were not significantly correlated (r = 0.16, − 0.08 to 0.39, p = 0.20). A moderate significant association was detected between pre-intervention VO2max and TPF (r = 0.46, 0.24–0.63, p = 0.0001). Resting HR was significantly associated with TPF (r = 0.66, 0.49–0.77, p < 0.0001, large). A small nonsignificant association (r = 0.16, − 0.08 to 0.39, p = 0.20) was found between HRmax and PF.
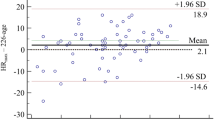
The measurement agreement between pre-intervention VO2max and VO2max estimating variables reported significant bias when considering VO2max EstNes and VO2max EstTPF (Table 2, Figs. 1 and 2).

Bland and Altman plot of pre-intervention VO2max against VO2max estimated using the Nes et al. (2013) equation for maximal heart rate. For estimanting the VO2max was used the theoretical factor (i.e. 15 ml∙kg−1∙min−1)

Bland and Altman plot of pre-intervention VO2max against VO2max estimated using the the theoretical factor (i.e. 15 ml kg−1 min−1) and actual maximal heart rate
Post-intervention
Post-intervention HRrest and HRmax were 61 ± 10 and 181 ± 10 beats min−1, respectively. Significant (p < 0.0001) differences were reported between pre-to-post HRrest (6.7 ± 7.5 beats min−1, 3.9–9.7) and HRmax (4.8 ± 4.1 beats min−1, 3.2–6.4). Nonsignificant associations were detected between VO2max post and HRrest (r = − 0.10, − 0.45 to 0.29, p = 0.63) and HRmax (r = 0.23, − 0.15 to 0.56, p = 0.23). The post-intervention SPF was moderately (r = 0.46, 0.09–0.70, p = 0.02) associated with post-intervention VO2max. Very large and small associations were detected between post-intervention HRrest (r = 0.80, 0.62–0.91, p < 0.0001) and HRmax (r = − 0.21, − 0.54 to 0.17, p = 0.28) with post-intervention SPF, respectively. The VO2max estimation values were not significantly different (form trivial to medium effect) from post-intervention VO2max (Table 3).
Training intervention
The participants’ (n = 28) VO2max significantly (p < 0.0001, d = 0.93) improved at post-intervention, by 3.2 ± 3.4 ml kg−1 min−1 (1.9–4.5), with mean values changing from 41.0 ± 5.3 to 44.2 ± 5.2 ml kg−1 min−1. Significant decreases in HRrest (from 68 ± 13 to 61 ± 10 beats min−1, 4–10, p < 0.0001, d = 1.0) and HRmax (from 186 ± 9 to 181 ± 10 beats min−1, 3–6, p < 0.0001, d = 1.3) were observed at post-intervention.
Discussion
The purpose of this study was to examine the applicability of the HRratio method for estimating VO2max in recreational football players in the untrained and trained states. This with the aim of avoiding all the logistical and procedural costs and constraints usually associated with field and laboratory assessments. This study’s results have shown that in the untrained state the participants’ actual VO2max was moderately lower than the estimated VO2max using TPF. A trivial nonsignificant difference was found when VO2max was estimated using SPF. When using estimated HRmax and TPF, a small nonsignificant difference was reported between actual and estimated VO2max. In the trained state, the estimated VO2max values were not significantly different from the post-intervention actual VO2max. Large effect sizes were found when considering TPF for estimating VO2max using actual HRmax (i.e. VO2max EstTPF) and using the Nes et al. (2013) formula (i.e. VO2max NesTPF). The results of this study provide evidence of the applicability of HRratio in estimating VO2max in male adult/middle-aged recreational football players.
In clinical settings, VO2max is used to classify the patient’s physiological reserve and to discipline admission and guide rehabilitation programmes (Ahmed 2020). Uth (2005) and Uth et al. (2004) tested the validity and measurement accuracy of a VO2max estimation method requiring resting and maximal HR values. To facilitate the procedures in the use of their proposed VO2max estimating method, the cited authors proposed the use of age-dependent equations. The satisfactory results reported with trained individuals suggested the use of this HRratio method with untrained participants.
Recreational football has been reported as an effective exercise mode for enhancing participants’ VO2max with low training exposure (i.e. 2 weekly training sessions for 10–12 weeks) (Milanovic et al. 2018). Furthermore, the reported average changes (i.e. 3.5 ml kg−1 min−1) are deemed to be clinically sound and to potentially reduce cardiovascular disease and all-cause death (Aspenes et al. 2011; Nes et al. 2013). The interest in recreational football for cardiovascular fitness promoted its popularity as a training intervention in the general population and the use of objective low-costs tests to estimate VO2max to control and regulate recreational football implementation (Castagna et al. 2020; Póvoas et al. 2019a).
This study’s results clearly indicated that the HRratio method may represent a useful tool for evaluating cardiorespiratory fitness in healthy adult/middle-aged men enrolled in recreational football interventions. The reported differences were practically acceptable by reference to the usual measurement error for VO2max assessment and the supposed clinical importance of variations in cardiorespiratory fitness (Aspenes et al. 2011; Nes et al. 2014). Indeed, this study’s calculations to estimate VO2max produced average differences in the range of ± 2%, corresponding to approximately 2 ml kg−1 min−1. Although lower than the supposed clinical relevance, the use of TBF (i.e. 15) reported overestimations in actual VO2max values that may exceed 1 MET when considering the reported 95% confidence interval limits (Table 1). This suggests that SPF is of interest when dealing with recreational football participants with health and baseline fitness levels like those seen in this study.
The assessment of VO2max under laboratory controlled procedures has been reported to be affected by biological and systematic error that is supposed to result in a ~ 6% measurement error (Katch et al. 1982), with biologically derived variations accounting for 90% of the global variation (Beltz et al. 2016; Balady et al. 2010). In their review, Balady et al. (2010) quantified the biological error in VO2max assessment as 3–4%. Given that the beneficial effects of variations on patients’ cardiorespiratory fitness have been reported in absolute values, the quantification of raw differences assumes clinical relevance (Aspenes et al. 2011; Nes et al. 2014). The absolute test–retest error in VO2max has been reported to be quantified as 2.58 ml kg−1 min−1 (Beltz et al. 2016), a value that is greater than the differences reported across the various estimation approaches used in this study (i.e. 0.7–1.5 ml kg−1 min−1).
This recreational football training resulted in a ~ 8% improvement in VO2max, corresponding to 3.2 ml kg−1 min−1. Large and significant decrements were reported in HRrest (~ 10%) and HRmax (~ 3%) post-intervention. Cardiorespiratory fitness improvement was unrelated to the reported variations in HR ratio variables. These changes are in line with previously reported training studies, supporting the contention of football as an effective intervention for improving cardiorespiratory fitness in previously untrained men (Milanovic et al. 2015). In the acquired higher cardiorespiratory fitness condition, i.e. trained state, the variables estimating VO2max used in this study maintained their predictive strength, suggesting the use of the HR ratio method in recreational football interventions to control and regulate the training process. Interestingly, the reported variations at post-training rest and maximal HR did not affect the predictive strength of the proposed metrics.
This study’s findings provide strong supporting evidence for interest in the HRratio method, previously successfully proposed for estimating VO2max in trained individuals (Uth 2005; Uth et al. 2004), for untrained participants. With this study, the practical interest of the HRratio method was confirmed and proved successful for estimating cardiorespiratory fitness in the untrained state. Thus, extending the applicability of this HR-based method to the general population. The precision of the HRratio may be satisfactory even when using the available equations to estimate individual HRmax, which remains the most challenging variable in the calculation involved in this ideally cardiopulmonary test-independent approach (Uth 2005; Uth et al. 2004). However, this study’s findings suggest that the precision of the estimation may be promoted if population-specific equations are considered (Póvoas et al. 2020) and specifically the use of the Nes et al. (2013) equation in the untrained state when considering the theoretical BF.
Perspectives
The robustness of the HRratio approach logically lies in the accuracy of the variables considered. The internal validity of this study was promoted using a validated population-specific (i.e. recreational football) multiple approach for determining participants’ HRmax (Póvoas et al. 2019b). Individual HRmax was determined using maximal laboratory and field tests to confirm the achievement of maximal values (Póvoas et al. 2019b). However, no form of re-test was performed to confirm participants’ VO2max achievement (Poole and Jones 2017). This may be regarded as this study’s main limitation in light of the arguments reported on maximal aerobic scopus of humans and the methods that should be used to achieve it (Poole and Jones 2017; Green and Askew 2018). Even if consideration for a confirmation VO2max test is methodologically sound, the practical effectiveness of this consistency measurement procedure has been challenged when dealing with untrained populations (Azevedo et al. 2018). Although an impeccable procedure, the VO2max confirmation test (i.e. cardiorespiratory re-testing) was reported to not provide the expected measurement accuracy, calling into question the cost/benefit of this practice in untrained individuals (Azevedo et al. 2018).
The interest of the HRratio method due to its a priori potential for categorising the cardiorespiratory fitness of recreational football players warrants further studies with populations of different sex and age from this study’s participants. In addition, future cross-validation studies should confirm this study’s SPF. The robustness of the HRratio validity of the training study should be verified with large-scale randomised controlled trials.
References
Ahmed I (2020) COVID-19—does exercise prescription and maximal oxygen uptake (VO2 max) have a role in risk-stratifying patients? Clin Med (lond). https://doi.org/10.7861/clinmed.2020-0111
Aspenes ST, Nilsen TI, Skaug EA, Bertheussen GF, Ellingsen Ø, Vatten L, Wisløff U (2011) Peak oxygen uptake and cardiovascular risk factors in 4631 healthy women and men. Med Sci Sports Exerc 43(8):1465–1473. https://doi.org/10.1249/MSS.0b013e31820ca81c
Azevedo P, Bhammar DM, Babb TG, Bowen TS, Witte KK, Rossiter HB, Brugniaux JV, Perry BD, de Lucas RD, Turnes T, Sabino-Carvalho JL, Lopes TR, Zacca R, Fernandes RJ, McKie GL, Hazell TJ, Helal L, da Silveira AD, McNulty CR, Roberg RA, Nightingale TE, Alrashidi AA, Mashkovskiy E, Krassioukov A, Clos P, Laroche D, Pageaux B, Poole DC, Jones AM, Schaun GZ, de Souza DS, de Lopes TOB, Vagula M, Zuo L, Zhao T (2018) Commentaries on viewpoint: VO2peak is an acceptable estimate of cardiorespiratory fitness but not VO2max. J Appl Physiol (1985) 125(1):233–240. https://doi.org/10.1152/japplphysiol.00319.2018
Bakeman R (2005) Recommended effect size statistics for repeated measures designs. Behav Res Methods 37(3):379–384
Balady GJ, Arena R, Sietsema K, Myers J, Coke L, Fletcher GF, Forman D, Franklin B, Guazzi M, Gulati M, Keteyian SJ, Lavie CJ, Macko R, Mancini D, Milani RV (2010) Clinician’s guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Circulation 122(2):191–225. https://doi.org/10.1161/CIR.0b013e3181e52e69
Beltz NM, Gibson AL, Janot JM, Kravitz L, Mermier CM, Dalleck LC (2016) Graded exercise testing protocols for the determination of VO2max: historical perspectives, progress, and future considerations. J Sports Med 2016:3968393. https://doi.org/10.1155/2016/3968393
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1(8476):307–310
Castagna C, Krustrup P, Povoas S (2020) Yo–Yo intermittent tests are a valid tool for aerobic fitness assessment in recreational football. Eur J Appl Physiol 120(1):137–147. https://doi.org/10.1007/s00421-019-04258-8
Church TS, Blair SN, Cocreham S, Johannsen N, Johnson W, Kramer K, Mikus CR, Myers V, Nauta M, Rodarte RQ, Sparks L, Thompson A, Earnest CP (2010) Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: a randomized controlled trial. JAMA 304(20):2253–2262. https://doi.org/10.1001/jama.2010.1710
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates, Hillsdale
Diaz-Canestro C, Montero D (2019) Sex dimorphism of VO(2max) trainability: a systematic review and meta-analysis. Sports Med 49(12):1949–1956. https://doi.org/10.1007/s40279-019-01180-z
Garcia-Tabar I, Eclache JP, Aramendi JF, Gorostiaga EM (2015) Gas analyzer’s drift leads to systematic error in maximal oxygen uptake and maximal respiratory exchange ratio determination. Front Physiol 6:308. https://doi.org/10.3389/fphys.2015.00308
Green S, Askew C (2018) V̇O2peak is an acceptable estimate of cardiorespiratory fitness but not V̇O2max. J Appl Physiol 125(1):229–232. https://doi.org/10.1152/japplphysiol.00850.2017
Hopkins WG, Marshall SW, Batterham AM, Hanin J (2009) Progressive statistics for studies in sports medicine and exercise science. Med Sci Sports Exerc 41(1):3–13. https://doi.org/10.1249/MSS.0b013e31818cb278
Katch VL, Sady SS, Freedson P (1982) Biological variability in maximum aerobic power. Med Sci Sports Exerc 14:21–25
Liff MH, Hoff M, Fremo T, Wisløff U, Videm V (2020) An estimation model for cardiorespiratory fitness in adults with rheumatoid arthritis. Med Sci Sports Exerc 52(6):1248–1255. https://doi.org/10.1249/mss.0000000000002250
Midgley AW, McNaughton LR, Wilkinson M (2006) Criteria and other methodological considerations in the evaluation of time at VO2max. J Sports Med Phys Fit 46(2):183–188
Midgley AW, McNaughton LR, Polman R, Marchant D (2007) Criteria for determination of maximal oxygen uptake: a brief critique and recommendations for future research. Sports Med 37(12):1019–1028
Milanovic Z, Pantelic S, Covic N, Sporis G, Krustrup P (2015) Is recreational soccer effective for improving VO2max a systematic review and meta-analysis. Sports Med 45(9):1339–1353. https://doi.org/10.1007/s40279-015-0361-4
Milanovic Z, Pantelic S, Covic N, Sporis G, Mohr M, Krustrup P (2018) Broad-spectrum physical fitness benefits of recreational football: a systematic review and meta-analysis. Br J Sports Med. https://doi.org/10.1136/bjsports-2017-097885
Nes BM, Janszky I, Wisloff U, Stoylen A, Karlsen T (2013) Age-predicted maximal heart rate in healthy subjects: the HUNT fitness study. Scand J Med Sci Sports 23(6):697–704. https://doi.org/10.1111/j.1600-0838.2012.01445.x
Nes BM, Vatten LJ, Nauman J, Janszky I, Wisloff U (2014) A simple nonexercise model of cardiorespiratory fitness predicts long-term mortality. Med Sci Sports Exerc 46(6):1159–1165. https://doi.org/10.1249/MSS.0000000000000219
Poole DC, Jones AM (2017) Measurement of the maximum oxygen uptake V̇O2max: V̇O2peak is no longer acceptable. J Appl Physiol 122(4):997–1002. https://doi.org/10.1152/japplphysiol.01063.2016
Póvoas SCA, Krustrup P, Castagna C, da Silva PMR, Coelho ESMJ, Pereira RLM, Larsen MN (2018) Reliability of submaximal Yo–Yo tests in 9- to 16-year-old untrained schoolchildren. Pediatr Exerc Sci 30(4):537–545. https://doi.org/10.1123/pes.2017-0139
Póvoas SC, Krustrup P, Castagna C (2019a) Submaximal field testing validity for aerobic fitness assessment in recreational football. Scand J Med Sci Sports. https://doi.org/10.1111/sms.13606
Póvoas SCA, Krustrup P, Pereira R, Vieira S, Carneiro I, Magalhaes J, Castagna C (2019b) Maximal heart rate assessment in recreational football players. A study involving a multiple testing approach. Scand J Med Sci Sports. https://doi.org/10.1111/sms.13472
Póvoas S, Krustrup P, Castagna C (2020) Estimation of maximal heart rate in recreational football: a field study. Eur J Appl Physiol 120(4):925–933. https://doi.org/10.1007/s00421-020-04334-4
Uth N (2005) Gender difference in the proportionality factor between the mass specific VO2max and the ratio between HR(max) and HR(rest). Int J Sports Med 26(9):763–767. https://doi.org/10.1055/s-2005-837443
Uth N, Sorensen H, Overgaard K, Pedersen PK (2004) Estimation of VO2max from the ratio between HRmax and HRrest–the Heart Rate Ratio Method. Eur J Appl Physiol 91(1):111–115. https://doi.org/10.1007/s00421-003-0988-y
Warburton D, Nicol C, Bredin SSD (2006) Prescribing exercise as preventative therapy. CMAJ 174(7):961–974
Zeiher J, Ombrellaro KJ, Perumal N, Keil T, Mensink GBM, Finger JD (2019) Correlates and determinants of cardiorespiratory fitness in adults: a systematic review. Sports Med Open 5(1):39. https://doi.org/10.1186/s40798-019-0211-2
Author information
Authors and Affiliations
Contributions
CC devised the study. SP: collected the data. CC and SP analysed the data and wrote the first draft of the paper. PK supervised data analyses and edited the manuscript until the submitted version. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors do not have any conflict of interests and state that the results of the present study do not constitute endorsement by EJAP. The authors alone are responsible for the content and writing of the manuscript.
Additional information
Communicated by Kirsty Elliott Sale.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Castagna, C., Krustrup, P. & Póvoas, S. Estimation of maximal oxygen uptake using the heart rate ratio method in male recreational football players. Eur J Appl Physiol 122, 1421–1428 (2022). https://doi.org/10.1007/s00421-022-04928-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-022-04928-0