
Abstract
Background
For most viral encephalitides, therapy is merely supportive. Intravenous immunoglobulins (IVIG) have been used as a prophylactic and therapeutic approach. We conduct a systematic review on the safety and efficacy of IVIG in viral encephalitis.
Methods
We conducted a systematic review assessing PubMed, Cochrane Database, Biosis Previews and the ClinicalTrials.gov website to identify all reports on patients with viral encephalitis treated with IVIG as of May 31, 2019. The main outcomes assessed were therapeutic efficacy and safety. For an increased homogeneity of the population, atypical viral infections were excluded, as were reports on prophylactic IVIG use, intrathecal application of immunoglobulins, or use of antibody-enriched IVIG-preparations. Data were extracted from published studies. Descriptive statistics were used.
Results
We included a total of 44 studies (39 case reports). The case reports cover a total of 53 patients. Our search retrieved two prospective and three retrospective studies. These show heterogeneous results as to the efficacy of IVIG therapy. Only one study reports a significant association between IVIG-use and death (odds ratio 0.032; 95% confidence interval 0.0033–0.3024; p = 0.0027). None of the studies report significant differences in the number of serious adverse events.
Conclusion
Data on the efficacy of IVIG-therapy is heterogeneous. While it seems generally safe, evident superiority compared to supportive treatment has not been demonstrated so far. Future trials should also investigate the optimal dosing and timing of IVIG and their benefit in the immunosuppressed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Encephalitis is an acute neurological syndrome characterized by altered mental status in combination with two or more secondary diagnostic criteria (fever, new epileptic seizures or neurological deficits, cerebral spinal fluid pleocytosis, specific alterations detected by neuroimaging or electroencephalography). The cause is unknown in approximately half of all cases. In the remainder, up to 50% are due to viral pathogens [1]. While specific antiviral treatment is available for a small subset of viral encephalitides—most notably acyclovir for herpes simplex encephalitis—therapy is merely supportive for most of them.
Patients at particular risk for viral encephalitis are those with congenital, acquired, or iatrogenic immunodeficiencies. Severe courses of viral encephalitides have—among others—been described after therapy with CD20-depleting agents [2, 3]. These agents act via direct depletion of pre-B and mature B-cells, therefore impairing the alloantibody response [4]. Furthermore, this effect may complicate the serological diagnosis, thereby delaying appropriate treatment [3].
In autoimmune encephalitis, the use of intravenous immunoglobulins (IVIG) is backed by controlled trials and has explicitly been recommended [5, 6]. They have also repeatedly been used as a prophylactic and therapeutic approach in viral encephalitides. Their use is mostly safe. Severe side effects are rare and include renal failure, thromboembolic events, and anaphylactic reactions. The latter are usually related to IgA deficiency [7]. However, their therapeutic efficiency in encephalitis is still a matter of debate. We conduct a systematic review on the safety and efficacy of IVIG in an adult and paediatric population with viral encephalitis.
Methods
We conducted a systematic review and report it according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards [8]. The main outcomes assessed were therapeutic efficacy (death/survival) and safety.
We performed a MEDLINE literature search using PubMed to identify all reports as of May 31, 2019 with no restrictions on start date using the search terms [“Encephalitis, Viral” (Mesh)] AND “Immunoglobulins, Intravenous” (Mesh) and [“Encephalitis, Viral” (Mesh)] and “Immunoglobulins, Intravenous/therapeutic use” (Mesh). Other databases searched include the Cochrane Database, Biosis Previews and the ClinicalTrials.gov website (search terms “viral encephalitis” AND “immunoglobulins”). Titles and abstracts of the reports obtained were screened for inclusion in the review using the following criteria: population with viral encephalitis (atypical viral infections such as JC-virus and slow-virus-infections were excluded); outcome and safety of IVIG therapy (reports on prophylactic IVIG use, intrathecal application of immunoglobulins, or use of IVIG-preparations that have been enriched for specific antiviral antibodies were excluded). Exclusion criteria were based on the intention to increase the homogeneity of the population under investigation.
Articles published in languages other than English, German, French or Spanish as well as duplicate studies, preclinical studies, editorials and reviews (except for secondary search) were excluded. Included were all case reports, case series, retrospective and prospective observational studies, and randomized controlled trials. A secondary search for other relevant articles was performed in the articles included after full-text analysis as well as in reviews on the topic.
The main outcomes assessed for observational studies, case series and clinical trials were efficacy and safety of the therapy. Efficacy was defined as survival. Safety was defined as number of severe adverse events. Secondary outcome parameters are listed in the results section if available from the reports. For case reports, the clinical outcome as stated in the respective paper is listed in Table 1.
Statistics were performed by JW using MedCalc®. Descriptive statistics were used. Where available, statistical results from group comparisons were extracted from the paper. If unavailable, odds ratios (OR) including 95% confidence intervals (CI) were calculated using individual patient data reported by the authors. Statistical significance was assessed using Fisher’s exact test.
A systematic assessment of the available evidence was conducted using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) methodology [9, 10]. A meta-analysis was not performed due to the paucity of prospective randomised trials. A review protocol can be obtained from JW.
The study was exempt from ethical approval procedures by the Ethics Committee of Upper Austria.
Results
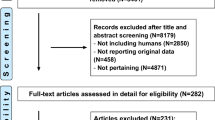
We screened a total of 377 studies, 44 of which were included (see Fig. 1): one prospective trial, one prospective case series, three retrospective observational studies, and 39 case reports. The case reports cover a total of 53 patients (37 adults, 16 children). 31 patients were immunosuppressed (27 adults): 17 post organ transplantation, 11 secondary to hematological malignancy, three due to autoimmune disease. The immunosuppressive drugs most frequently used included steroids (20 patients), calcineurin inhibitors (tacrolimus: 14 patients; ciclosporin: 5 patients), mycophenolic acid (18 patients), and anti-CD20 monoclonal antibodies (rituximab: nine patients; obinutuzumab: one patient). 21 patients had a combination of at least two of these agents.

Flow-chart depicting the selection process of reports included in this review according to PRISMA guidelines
The most common pathogens in adults (case reports) included West Nile virus (17 patients), enterovirus (four patients) and Epstein Barr virus (three patients), whereas, in children, enterovirus (eight patients), parvovirus B19 (three patients) and mumps virus (two patients) were most frequently reported. IVIG was used as monotherapy in seven patients and as add-on therapy in 46 patients in combination with acyclovir (21 patients), steroids (17 patients), interferon alpha-2b (nine patients), and ganciclovir (six patients). Other therapies applied included valganciclovir, plasma exchange, ribavirin, and pleconaril. In 13 patients, reduction of immunosuppression as part of the antiviral treatment was explicitly mentioned.
Modalities of IVIG-administration varied widely. The most frequently reported dose was 400 mg/kg (16 patients). The number of patients in whom this dose was used may have been higher as some authors only report total doses or do not specify the amount of IVIG applied. Application frequency varied between a single infusion and a continuous therapy in patients with ongoing immunosuppression.
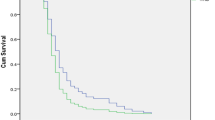
IVIG-therapy was started between one and 101 days after symptom onset. For 28 patients, no information has been provided on the interval between symptom onset and the start of IVIG. For 20 patients, neither the interval between symptom onset nor hospital admission and the start of therapy was reported. Median treatment delay was 6.5 days (from hospitalization) and ten days (from symptom onset) in those patients that died, and 4.5 respectively eight days in those that recovered completely. This difference was even greater for West Nile Virus encephalitis patients with a median treatment delay of ten days from symptom onset in those who died and four days in those in whom symptoms remitted completely. No adverse effects of IVIG were explicitly mentioned.
Intensive care (ICU) dependency was explicitly reported for 26 patients. Most of these had a diagnosis of West Nile Virus encephalitis (13 versus 5 in the non-ICU group; p = 0.02) or enteroviral encephalitis (5 versus 8; p = 0.38). Unsurprisingly, more patients died in the ICU than in the non-ICU group (7 versus 2; p = 0.059). Of 53 patients, 44 were alive at the last follow-up. For 21 patients, full recovery was reported. In 20 patients, there were residual symptoms, in six of them severe ones (estimated modified Rankin scale 4–5). 9 patients had died (7 West Nile Virus encephalitis, 2 enterovirus encephalitis)—all of them had been immunosuppressed. For three patients, no follow-up information was available. For details on all case reports see Table 1.
Our search retrieved one prospective trial and one prospective case series. A prospective, randomized, placebo-controlled trial (RCT) investigated the use of IVIG harvested in a geographical region with high Japanese encephalitis (JE) prevalence (ImmunoRel®, 400 mg/kg/day for 5 days) in Nepalese children with suspected JE [11]. Saline solution was used as a placebo. However, only a small cohort consisting of 11 participants and 11 controls was tested as the study was designed as a pilot feasibility study. Endpoints consisted in survival, clinical outcome as Liverpool Outcome Score, Glasgow Coma Scale, and number of days of hospitalization at discharge, survival and clinical outcome at three to six months follow-up, and frequency of adverse events. Three serious adverse events are reported in JE patients: hypotension (one each in the IVIG and non-IVIG group) and melena (one in the IVIG-group). At discharge, one patient had died in the IVIG group, none in the control group (OR see Table 2). One patient in each group had recovered completely (OR 1, 95% CI 0–43.7). Equally, no significant differences concerning the other outcome parameter and safety endpoints at discharge or at follow-up were reported.
In addition to the prospective trial described in this review, a Cochrane Review on the use of IVIG in childhood encephalitis reports two more randomized trials in children with enteroviral and all-cause viral encephalitis [12]. We excluded these trials as the articles are in Chinese and not listed in any of the databases used for this review. Neither of them reports serious adverse events, nor do they provide data on the neurological outcome at discharge or follow-up. In a pooled analysis of these two trials, the Cochrane Review reports a significant advantage for some of the secondary endpoints (“length of hospital stay, time to resolution of fever, time to stop spasms, time to regain consciousness, time to resolution of neuropathic symptoms”) for those cohorts treated with IVIG. However, the quality of evidence was deemed to be very low.
A prospective case series focused on EV71-infection of the nervous system [13]. It was designed as a placebo-controlled randomized trial on the efficiency of a methylprednisolone pulse (10 mg/kg/d for three days; 40 patients in each of the verum and control group). Steroid treatment was not found to be beneficial in this trial. All patients received IVIG 1 g/kg/d for two days as part of the standard therapy. As all participants received IVIG, no conclusion on the efficacy of this treatment can be made. No IVIG-associated adverse effects were reported by the authors.
Furthermore, we found three retrospective observational studies. Wang et al. report on a cohort of 97 children (information on therapy obtained available in 34 patients) with EV71 encephalitis, 14 of whom were treated with IVIG: four of them died, ten survived. This compares to 15 survivors and five dead in the group who received supportive care only (OR 1.2; 95% CI 0.26–5.59). Dosage and timing of IVIG-therapy are not detailed – neither are secondary endpoints, including adverse events.
In a retrospective observational study the authors distinguish a group of 72 patients diagnosed as “viral meningitis, viral encephalitis and viral myelitis” [14]. The most frequent diagnoses included echovirus, (para)influenza, coxsackievirus, varicella virus, herpes simplex virus, and tick-borne encephalitis virus infections. However, the exact distribution of pathogens was not specified. In one-third of patients, the causative agent could not be identified. 58 patients were treated with IVIG (5 g/day for four successive days; treated at the author’s institution between 1975 and 1979) and had a significantly better outcome than the group who had not received IVIG therapy (treated at the same institution between 1970 and 1974). In the treatment group, one patient died and one was left with residual neurological deficits, compared to five patients who died and two who remained with residual deficits out of the 14 patients not treated with IVIG. The odds ratio for a lethal outcome was significantly lower in the group treated with IVIG (p = 0.0027), as was the odds ratio for incomplete neurological recovery (0.036, 95% CI 0.0062–0.207; p = 0.0002). A bias is most likely, not least because the two groups were treated during different time periods and it cannot be excluded from the manuscript that other therapeutic options had emerged in the interval. Furthermore, there is little information to determine the diagnostic accuracy. Hence, some cases may have been misdiagnosed as viral encephalitis.
In another retrospective non-randomized approach, the authors compare two groups of patients with measles encephalitis who received different IVIG-dosages [4 to 16 ml (12 patients) vs. 20 ml (15 patients); mg not specified] with a third group of 14 patients who did not receive IVIG [15]. The authors report that patients treated with IVIG reportedly had a better outcome, shorter hospital stays and lower mortality than the control group. However, the OR for death calculated from the numbers given in the report (two patients died in the control group, three patients in both treatment groups combined) does not reach significance; neither does the OR for incomplete neurological recovery (0.6, 95% CI 0.16–2.21). No adverse effects of IVIG treatment occurred.
Details on the trials, observational studies, and the case series including GRADE ratings are listed in Table 2.
Discussion
Data on the efficacy of IVIG-therapy collected from case reports, case series, observational studies, and one RCT is heterogeneous. A clear superiority compared to supportive treatment could not be demonstrated. The data generated by the case series, observational studies and the RCT is of low-quality due to small and heterogeneous study populations and interventions, incomplete data, and possible selection, allocation, and detection bias. Most patients received IVIG as add-on therapy, thereby obscuring whether therapeutic effects were actually caused by this compound. Furthermore, the generalizability of the results to other pathogens and different socioeconomic settings is questionable. Hence, a general recommendation as to the use of IVIG in viral encephalitis cannot be made at this point.
The case reports reveal a strong association of fatal outcomes with pre-existing immunosuppression. Many patients included received combinations of steroids, calcineurin inhibitors, mycophenolate acid, and anti-CD20 therapeutics, leading to a combined deficiency of the T- and B-cell lines. In these patients, close monitoring of serum immunoglobulin levels to identify those who might benefit from replacement therapy may be advisable. In a cohort study of 8633 patients receiving rituximab, approximately half of patients whose immunoglobulin levels were investigated had hypogammaglobulinaemia [16]. The rate of severe infections in the study group was 28% in the 18 months following rituximab initiation and was highest in the group with hypogammaglobulinaemia. In those patients that received immunoglobulin replacement, a higher cumulative replacement dose was associated with a reduction of serious infections.
Side effects were reported in none of the case reports, case series, observational studies, or the RCT. This may be due to publication bias. In some patients, IVIG side effects may also have been mistaken for symptoms of the underlying disease.
Considering the high mortality and morbidity of encephalitis and the paucity of specific treatment options, more studies are urgently needed. One clinical trial investigating the role of early IVIG treatment in children with encephalitis (NCT02308982) is underway, investigating the effect of this therapy on clinical outcome (primary outcome measure). Future trials should analyze the following parameters as well:
Are IVIG-preparations selected for their content of pathogen-specific antibodies more efficient than unselected preparations?
IVIG are plasma products of pooled IgG derived from multiple donors. They contain immunoglobulins directed at a wide variety of pathogens. Their exact composition depends on the prevalence of infectants in the geographic area of the population that contributed to the pool [17]. A twofold mode of action of IVIG has been proposed. First, IVIG may increase viral clearance due to antibody-dependent neutralization. Second, they have an immunomodulatory effect by mitigating hyperinflammation, which has been associated with a poor clinical outcome in viral encephalitis [18, 19]. This mechanism has been suggested to be independent of the presence of pathogen-specific antibodies [20]. Among the suggested mechanisms are impediment of CNS infiltration by pathogenic leukocytes, blockade of Fc receptors of macrophages, interference with complement activation, and modification of cytokine expression [21,22,23].
Experiments in mice demonstrated a dramatically reduced mortality in mice treated with IVIG-batches obtained from donors from a region endemic for West Nilve virus (WNV) compared to those obtained from US-donors harvested before WNV was introduced in the US [24]. Similar results have been described in a mouse model for tick-borne encephalitis (TBE) [25]. Several authors report successful application of these preparations in human patients.65–67 While their use seems intuitively convincing, data as to their efficiency is controversial: a recently published trial of 62 hospitalized WNV encephalitis patients randomized to receive Omr-IgG-am® (an IVIG containing antibodies specific for WNV), standard IVIG, or normal saline showed no significant differences between groups receiving Omr-IgG-am compared with IVIG or saline for either the safety or efficacy endpoints [26]. Reasons may have included a small study population (the trial was terminated prematurely), delayed enrolment of participants (mean time from admission to infusion of study drug 2.7 days), and dosage (only a single infusion of the trial drug).
Are alternative routes of immunoglobulin application more efficient than the intravenous administration?
Alternative routes of immunoglobulin application that have been described include intramuscular, subcutaneous, and intrathecal administration. Although meningeal inflammation enhances IVIG penetration of the blood–brain barrier, the amount of IVIG entering the CNS is unpredictable. Hence, direct installation of IVIG into the intrathecal space may be more efficient [17]. While some authors report cases successfully treated by these means, data from controlled trials are lacking [27,28,29]. Furthermore, (auto-)inflammatory reactions triggered by IVIG-binding to neuroglial epitopes might be a concern.
What is the ideal dosing and timing of IVIG application?
Most articles included in this review report IVIG doses of 400 mg/kg. However, the approaches vary widely and are somewhat arbitrary as the ideal dosing has not yet been established. The mechanism of actions of IVIGs seems to be dose-dependent, with higher doses needed to obtain an immunomodulating effect, which may be desirable for some infections, but not for others [30]. In a murine WNV-model, the therapeutic effect of IVIG containing high anti-WNV antibodies correlated with its dose [24].
The same uncertainty applies to the timing of IVIG-therapy. We found a wide variation of the time span between symptom onset and therapeutic IVIG in the case reports included in this review. Delays to initiate therapy were most often associated with slowly progressive, unspecific clinical presentations that may occur with enteroviral or parvoviral infections, for example [31, 32]. Several reports suggest that neurotropic viruses are more susceptible to antibody-mediated clearance during the viraemic phase than to cell-mediated immunity once intracerebral spread has taken place. In a murine model, treatment with WNV-specific immunoglobulin was more efficient in the viraemic phase, before the neuroinvasive disease had occurred. IVIG has been postulated to efficiently prevent encephalitis if applied within the first four to six days after infection. Previous studies suggest that flavivirus may invade the brain as early as three days post-inoculation [17, 33,34,35]. Clearance of the virus during the viraemic phase may be the reason for the efficiency of prophylactic IVIG replacement as reported by Barmettler et al.[16]
However, some effect on mortality by inoculation of IVIG was seen even after the virus had reached the brain [24, 36]. Underlying antibody-mediated suppression of intracellular virus replication has been suggested [37, 38]. However, this effect may be pathogen-specific. The degree of postexposure prophylaxis for TBE correlated inversely to the time interval between infection and treatment with virus-specific immunoglobulins in mice. The authors conclude that protection against this disease is only possible before established CNS infection [39]. Data on a murine model of JE showed that the virus enters the brain from two to five days post-inoculation of JEV. This process takes place with the blood–brain barrier (BBB) intact. Disruption of the BBB induced by inflammatory cytokines and chemokines did not occur until day four [40]. Hence, peripheral application of IVIG may be efficient either before the virus enters the brain or after BBB disruption, but not in between. Analysis of the case reports included in this review showed a tendency towards better recovery when IVIG treatment was started earlier. However, controlled data backing this assertion is lacking.
Does the efficiency of IVIG-therapy depend on the virus type?
The data obtained for this review do not permit conclusions as to which kind of viruses are more susceptible to IVIG therapy than others. However, the observations detailed above suggest that IVIG may eradicate those pathogens more efficiently that either remain bloodborne for an extended period and/or cause a significant BBB disruption. Many vector-borne viruses are transmitted via inoculation into the bloodstream where they may be neutralized by IVIG. As discussed above, they only remain bloodborne for a few days, necessitating a high level of suspicion and early commencement of therapy to obtain optimal results. On the other hand, studies on imaging characteristics in tick-borne encephalitis and West Nile virus encephalitis show that intraparenchymal contrast-enhancement as a sign of BBB disruption is uncommon in these diseases [41, 42]. Hence, these flavivirus species may be more difficult to treat with IVIG once they have entered the central nervous system.
Contrasting with the pathophysiology of vector-borne viruses, herpes simplex encephalitis is thought to occur via neuronal transmission. This may render IVIG therapy less efficient if administered early. However, diagnostic imaging frequently shows contrast-enhancement, probably rendering these patients amenable for add-on immunoglobulin treatment at this stage [43]. In this context, it would be interesting to obtain efficiency data on the combined use of acyclovir and IVIG in herpes simplex virus encephalitis.
In conclusion, only very low-quality evidence as to the clinical benefit and adverse effects of IVIG treatment in viral encephalitis exists. While IVIG application seems generally safe, its efficacy is still unclear. Hence, the indication and minutiae of IVIG-therapy in patients with viral encephalitis continue to rest on individual, case-specific decisions. RCTs in selected patient populations are needed to clarify its role in this severely affected cohort. Shortcomings of our review include the low-quality data of the reported studies due to small and heterogenous study populations and a high risk of bias, as well as incomplete data on individual patients and the confounding effect of multiple therapies.
References
Tyler KL (2018) Acute viral encephalitis. N Engl J Med 379:557–566. https://doi.org/10.1056/NEJMra1708714
Goates C, Tsuha S, Working S et al (2017) Seronegative West Nile virus infection in a patient treated with rituximab for rheumatoid arthritis. Am J Med 130:e257–e258. https://doi.org/10.1016/j.amjmed.2017.01.014
Morjaria S, Arguello E, Taur Y et al (2015) West Nile virus central nervous system infection in patients treated with rituximab: implications for diagnosis and prognosis, with a review of literature. Open Forum Infect Dis 2:136. https://doi.org/10.1093/ofid/ofv136
Levi ME, Quan D, Ho JT et al (2010) Impact of rituximab-associated B-cell defects on West Nile virus meningoencephalitis in solid organ transplant recipients. Clin Transplant 24:223–228. https://doi.org/10.1111/j.1399-0012.2009.01044.x
Dubey D, Britton J, McKeon A et al (2020) Randomized placebo-controlled trial of intravenous immunoglobulin in autoimmune LGI1/CASPR2 epilepsy. Ann Neurol 87:313–323. https://doi.org/10.1002/ana.25655
Zuliani L, Nosadini M, Gastaldi M et al (2019) Management of antibody-mediated autoimmune encephalitis in adults and children: literature review and consensus-based practical recommendations. Neurol Sci 40:2017–2030. https://doi.org/10.1007/s10072-019-03930-3
Růžek D, Dobler G, Niller HH (2013) May early intervention with high dose intravenous immunoglobulin pose a potentially successful treatment for severe cases of tick-borne encephalitis? BMC Infect Dis 13:306. https://doi.org/10.1186/1471-2334-13-306
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Guyatt GH, Oxman AD, Vist GE et al (2008) GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 336:924–926. https://doi.org/10.1136/bmj.39489.470347.AD
Guyatt G, Oxman AD, Akl EA et al (2011) GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol 64:383–394. https://doi.org/10.1016/j.jclinepi.2010.04.026
Rayamajhi A, Nightingale S, Bhatta NK et al (2015) A preliminary randomized double blind placebo-controlled trial of intravenous immunoglobulin for Japanese encephalitis in Nepal. PLoS ONE 10:e0122608. https://doi.org/10.1371/journal.pone.0122608
Iro MA, Martin NG, Absoud M, Pollard AJ (2017) Intravenous immunoglobulin for the treatment of childhood encephalitis. Cochrane Database Syst Rev 10:CD011367. https://doi.org/10.1002/14651858.CD011367.pub2
Zhang G, Wang J, Yao G, Shi B (2016) Efficacy of high-dose methylprednisolone pulse therapy in the treatment of enterovirus 71 encephalitis. Pak J Pharm Sci 29:1421–1427
Neu I (1980) Therapeutic value of immunoglobulins in central nervous system infections. Med Klin 75:554–557
Odessky L, Bedo AV, Jennings KG et al (1953) Therapeutic doses of gamma globulin in the treatment of measles encephalitis and encephalomyelitis. I. A clinical study of forty-one cases with follow-up studies. J Pediatr 43:536–568. https://doi.org/10.1016/s0022-3476(53)80330-6
Barmettler S, Ong M-S, Farmer JR et al (2018) Association of immunoglobulin levels, infectious risk, and mortality with rituximab and hypogammaglobulinemia. JAMA Netw Open 1:e184169. https://doi.org/10.1001/jamanetworkopen.2018.4169
Haley M, Retter AS, Fowler D et al (2003) The role for intravenous immunoglobulin in the treatment of West Nile virus encephalitis. Clin Infect Dis Off Publ Infect Dis Soc Am 37:e88-90. https://doi.org/10.1086/377172
Caramello P, Canta F, Balbiano R et al (2006) Role of intravenous immunoglobulin administration in Japanese encephalitis. Clin Infect Dis Off Publ Infect Dis Soc Am 43:1620–1621. https://doi.org/10.1086/509644
Winter PM, Dung NM, Loan HT et al (2004) Proinflammatory cytokines and chemokines in humans with Japanese encephalitis. J Infect Dis 190:1618–1626. https://doi.org/10.1086/423328
Ramakrishna C, Newo ANS, Shen Y-W, Cantin E (2011) Passively administered pooled human immunoglobulins exert IL-10 dependent anti-inflammatory effects that protect against fatal HSV encephalitis. PLoS Pathog 7:e1002071. https://doi.org/10.1371/journal.ppat.1002071
Srivastava R, Ramakrishna C, Cantin E (2015) Anti-inflammatory activity of intravenous immunoglobulins protects against West Nile virus encephalitis. J Gen Virol 96:1347–1357. https://doi.org/10.1099/vir.0.000079
Wang S-M, Lei H-Y, Liu C-C (2012) Cytokine immunopathogenesis of enterovirus 71 brain stem encephalitis. Clin Dev Immunol 2012:876241. https://doi.org/10.1155/2012/876241
Negi V-S, Elluru S, Sibéril S et al (2007) Intravenous immunoglobulin: an update on the clinical use and mechanisms of action. J Clin Immunol 27:233–245. https://doi.org/10.1007/s10875-007-9088-9
Ben-Nathan D, Lustig S, Tam G et al (2003) Prophylactic and therapeutic efficacy of human intravenous immunoglobulin in treating West Nile virus infection in mice. J Infect Dis 188:5–12. https://doi.org/10.1086/376870
Elsterova J, Palus M, Sirmarova J et al (2017) Tick-borne encephalitis virus neutralization by high dose intravenous immunoglobulin. Ticks Tick Borne Dis 8:253–258. https://doi.org/10.1016/j.ttbdis.2016.11.007
Gnann JW, Agrawal A, Hart J et al (2019) Lack of efficacy of high-titered immunoglobulin in patients with West Nile virus central nervous system disease. Emerg Infect Dis 25:2064–2073. https://doi.org/10.3201/eid2511.190537
Kondoh H, Kobayashi K, Sugio Y, Hayashi T (1987) Successful treatment of echovirus meningoencephalitis in sex-linked agammaglobulinaemia by intrathecal and intravenous injection of high titre gammaglobulin. Eur J Pediatr 146:610–612. https://doi.org/10.1007/bf02467368
Dwyer JM, Erlendsson K (1988) Intraventricular gamma-globulin for the management of enterovirus encephalitis. Pediatr Infect Dis J 7:S30-33
Erlendsson K, Swartz T, Dwyer JM (1985) Successful reversal of echovirus encephalitis in X-linked hypogammaglobulinemia by intraventricular administration of immunoglobulin. N Engl J Med 312:351–353. https://doi.org/10.1056/NEJM198502073120605
Bayry J, Lacroix-Desmazes S, Kazatchkine MD, Kaveri SV (2003) Intravenous immunoglobulin for infectious diseases: tailor-made or universal? J Infect Dis 188:1610. https://doi.org/10.1086/379335 (author reply 1610–1611)
Barah F, Vallely PJ, Chiswick ML et al (2001) Association of human parvovirus B19 infection with acute meningoencephalitis. Lancet Lond Engl 358:729–730. https://doi.org/10.1016/S0140-6736(01)05905-0
Akcakaya NH, Tekturk P, Cagatay A et al (2016) Atypical enterovirus encephalitis causing behavioral changes and autism-like clinical manifestations: case report. Acta Neurol Belg 116:679–681. https://doi.org/10.1007/s13760-016-0614-5
Agrawal AG, Petersen LR (2003) Human immunoglobulin as a treatment for West Nile virus infection. J Infect Dis 188:1–4. https://doi.org/10.1086/376871
Morelli MC, Sambri V, Grazi GL et al (2010) Absence of neuroinvasive disease in a liver transplant recipient who acquired West Nile virus (WNV) infection from the organ donor and who received WNV antibodies prophylactically. Clin Infect Dis Off Publ Infect Dis Soc Am 51:e34-37. https://doi.org/10.1086/655146
Roehrig JT, Staudinger LA, Hunt AR et al (2001) Antibody prophylaxis and therapy for flavivirus encephalitis infections. Ann N Y Acad Sci 951:286–297. https://doi.org/10.1111/j.1749-6632.2001.tb02704.x
Engle MJ, Diamond MS (2003) Antibody prophylaxis and therapy against West Nile virus infection in wild-type and immunodeficient mice. J Virol 77:12941–12949. https://doi.org/10.1128/jvi.77.24.12941-12949.2003
Rager-Zisman B, Ben Nathan D (2003) Efficacy of prophylactic and therapeutic human immunoglobulin on West Nile virus infection. Isr Med Assoc J IMAJ 5:691
Levine B, Hardwick JM, Trapp BD et al (1991) Antibody-mediated clearance of alphavirus infection from neurons. Science 254:856–860. https://doi.org/10.1126/science.1658936
Kreil TR, Eibl MM (1997) Pre- and postexposure protection by passive immunoglobulin but no enhancement of infection with a flavivirus in a mouse model. J Virol 71:2921–2927
Li F, Wang Y, Yu L et al (2015) Viral infection of the central nervous system and neuroinflammation precede blood–brain barrier disruption during Japanese encephalitis virus infection. J Virol 89:5602–5614. https://doi.org/10.1128/JVI.00143-15
Wagner JN, Sonnberger M, Troescher A et al (2020) Patients with breakthrough tick-borne encephalitis suffer a more severe clinical course and display extensive magnetic resonance imaging changes. Eur J Neurol 27:1201–1209. https://doi.org/10.1111/ene.14276
Ali M, Safriel Y, Sohi J et al (2005) West Nile virus infection: mr imaging findings in the nervous system. Am J Neuroradiol 26:289–297
Struffert T, Reith W (2000) Herpes simplex virus encephalitis: neuroradiologic differential diagnosis. Radiol 40:1011–1016. https://doi.org/10.1007/s001170050873
Borg SA, Tonkin A, Kleinig T, Waters M (2015) Unusual presentation of Epstein–Barr virus encephalitis in an older patient with a dramatic clinical response to intravenous immunoglobulin. Intern Med J 45:879–881. https://doi.org/10.1111/imj.12834
Caramello P, Canta F, Balbiano R et al (2007) A case of imported JE acquired during short travel in Vietnam. Are current recommendations about vaccination broader? J Travel Med 14:346–348. https://doi.org/10.1111/j.1708-8305.2007.00140.x
Erol I, Alehan F, Yalçin K (2006) Refractory status epilepticus owing to human parvovirus B19 encephalitis in a child. J Child Neurol 21:820–822. https://doi.org/10.1177/08830738060210092301
Eyckmans T, Wollants E, Janssens A et al (2014) Coxsackievirus A16 encephalitis during obinutuzumab therapy, Belgium, 2013. Emerg Infect Dis 20:913–915. https://doi.org/10.3201/eid2005.131766
Fay AJ, Noetzel MJ, Mar SS (2015) Pediatric hemorrhagic brainstem encephalitis associated with HHV-7 infection. Pediatr Neurol 53:523–526. https://doi.org/10.1016/j.pediatrneurol.2015.06.016
Garzo-Caldas N, Ruiz-Sainz E, Vila-Bedmar S et al (2017) Enteroviral T-cell encephalitis related to immunosuppressive therapy including rituximab. Neurology 89:408–409. https://doi.org/10.1212/WNL.0000000000004148
Geller TJ, Condie D (1995) A case of protracted coxsackie virus meningoencephalitis in a marginally immunodeficient child treated successfully with intravenous immunoglobulin. J Neurol Sci 129:131–133. https://doi.org/10.1016/0022-510x(94)00261-l
Georgescu A, Chiriac C, Tilea B, Kezdi I (2012) Severe enteroviral encephalitis complicated by encephalomalacia–case presentation. Rev Med Chir Soc Med Nat Iasi 116:799–803
Golomb MR, Durand ML, Schaefer PW et al (2001) A case of immunotherapy-responsive eastern equine encephalitis with diffusion-weighted imaging. Neurology 56:420–421. https://doi.org/10.1212/wnl.56.3.420
Greco F, Barbagallo ML, Chiodo DC et al (2008) Severe ataxia as a complication of human parvovirus B19 acute encephalitis in a child. J Child Neurol 23:1078–1080. https://doi.org/10.1177/0883073808315420
Hartmann CA, Vikram HR, Seville MT et al (2017) Neuroinvasive St. Louis encephalitis virus infection in solid organ transplant recipients. Am J Transplant Off J Am Soc Transplant Am Soc Transpl Surg 17:2200–2206. https://doi.org/10.1111/ajt.14336
Hindo H, Buescher ES, Frank LM et al (2005) West Nile virus infection in a teenage boy with acute lymphocytic leukemia in remission. J Pediatr Hematol Oncol 27:659–662. https://doi.org/10.1097/01.mph.0000188111.04459.6f
Hollander H, Schaefer PW, Hedley-Whyte ET (2005) Case records of the Massachusetts general hospital. Case 22–2005. An 81-year-old man with cough, fever, and altered mental status. N Engl J Med 353:287–295. https://doi.org/10.1056/NEJMcpc059017
Kimura E, Goto H, Migita A et al (2010) An adult norovirus-related encephalitis/encephalopathy with mild clinical manifestation. BMJ Case Rep. https://doi.org/10.1136/bcr.03.2010.2784
Kleinschmidt-DeMasters BK, Marder BA, Levi ME et al (2004) Naturally acquired West Nile virus encephalomyelitis in transplant recipients: clinical, laboratory, diagnostic, and neuropathological features. Arch Neurol 61:1210–1220. https://doi.org/10.1001/archneur.61.8.1210
Kleiter I, Jilg W, Bogdahn U, Steinbrecher A (2007) Delayed humoral immunity in a patient with severe tick-borne encephalitis after complete active vaccination. Infection 35:26–29. https://doi.org/10.1007/s15010-006-6614-2
Lau JSY, Low ZM, Abbott I et al (2017) Epstein–Barr virus encephalitis in solid organ transplantation. New Microbiol 40:212–217
Matsumoto Y, Morimoto I, Shibutani T et al (2005) Measles encephalitis in early pregnancy and after delivery. J Infect Chemother Off J Jpn Soc Chemother 11:97–100. https://doi.org/10.1007/s10156-005-0372-4
Miyagi T, Yamaguchi S, Yamamoto Y et al (2014) Varicella zoster virus encephalopathy in a patient with psoriatic arthritis treated with anti-TNFα agents. Eur J Dermatol EJD 24:398–399. https://doi.org/10.1684/ejd.2014.2331
Nakano A, Yamasaki R, Miyazaki S et al (2003) Beneficial effect of steroid pulse therapy on acute viral encephalitis. Eur Neurol 50:225–229. https://doi.org/10.1159/000073864
Nolan MA, Craig ME, Lahra MM et al (2003) Survival after pulmonary edema due to enterovirus 71 encephalitis. Neurology 60:1651–1656. https://doi.org/10.1212/01.wnl.0000066810.62490.ff
Odessky L, Schiff I, Sands IJ, Spielsinger D (1953) Mumps meningoencephalitis treated with gamma globulin. N Y State J Med 53:2672–2674
Padate BP, Keidan J (2006) Enteroviral meningoencephalitis in a patient with non-Hodgkin’s lymphoma treated previously with rituximab. Clin Lab Haematol 28:69–71. https://doi.org/10.1111/j.1365-2257.2006.00751.x
Quartier P, Tournilhac O, Archimbaud C et al (2003) Enteroviral meningoencephalitis after anti-CD20 (rituximab) treatment. Clin Infect Dis Off Publ Infect Dis Soc Am 36:e47-49. https://doi.org/10.1086/345746
Rhee C, Eaton EF, Concepcion W, Blackburn BG (2011) West Nile virus encephalitis acquired via liver transplantation and clinical response to intravenous immunoglobulin: case report and review of the literature. Transpl Infect Dis Off J Transplant Soc 13:312–317. https://doi.org/10.1111/j.1399-3062.2010.00595.x
Saquib R, Randall H, Chandrakantan A et al (2008) West Nile virus encephalitis in a renal transplant recipient: the role of intravenous immunoglobulin. Am J Kidney Dis Off J Natl Kidney Found 52:e19-21. https://doi.org/10.1053/j.ajkd.2008.03.042
Schilthuizen C, Berenschot HWA, Levin M-D (2010) Enteroviral encephalitis in a patient with a marginal zone lymphomatreated with rituximab. Neth J Med 68:221–223
Shaheen N, Mussai F (2019) Enteroviral Encephalitis in a Child With CNS Relapse of Burkitt Leukemia Treated With Rituximab. J Pediatr Hematol Oncol 41:e27–e29. https://doi.org/10.1097/MPH.0000000000001077
Smudla A, Gerlei Z, Gergely L et al (2011) West Nile virus encephalitis in kidney transplanted patient, first case in Hungary: case report. Interv Med Appl Sci 3:80–83. https://doi.org/10.1556/IMAS.3.2011.2.8
Suga K, Goji A, Shono M et al (2015) Mumps encephalitis with akinesia and mutism. Pediatr Int Off J Jpn Pediatr Soc 57:721–724. https://doi.org/10.1111/ped.12581
Ueno S, Sekimoto-Tsuboi S, Ishiguro Y et al (2015) Good’s syndrome with opportunistic infection of the central nervous system: a case report. BMC Neurol 15:150. https://doi.org/10.1186/s12883-015-0406-1
Villacé P, Navarro M, Font B, Segura F (2008) Acute cerebellar ataxia complicating infectious mononucleosis. Enferm Infecc Microbiol Clin 26:672–673. https://doi.org/10.1016/s0213-005x(08)75287-x
Winston DJ, Vikram HR, Rabe IB et al (2014) Donor-derived West Nile virus infection in solid organ transplant recipients: report of four additional cases and review of clinical, diagnostic, and therapeutic features. Transplantation 97:881–889. https://doi.org/10.1097/TP.0000000000000024
Xu X, Bergman P, Willows T et al (2012) CMV-associated encephalitis and antineuronal autoantibodies—a case report. BMC Neurol 12:87. https://doi.org/10.1186/1471-2377-12-87
Yango AF, Fischbach BV, Levy M et al (2014) West Nile virus infection in kidney and pancreas transplant recipients in the Dallas-Fort Worth Metroplex during the 2012 Texas epidemic. Transplantation 97:953–957. https://doi.org/10.1097/01.TP.0000438621.81686.ab
Zaganas I, Prinianakis G, Xirouchaki N, Mavridis M (2007) Opsoclonus-myoclonus syndrome associated with cytomegalovirus encephalitis. Neurology 68:1636. https://doi.org/10.1212/01.wnl.0000262766.50747.27
Wang SM, Liu CC, Tseng HW et al (1999) Clinical spectrum of enterovirus 71 infection in children in southern Taiwan, with an emphasis on neurological complications. Clin Infect Dis Off Publ Infect Dis Soc Am 29:184–190. https://doi.org/10.1086/520149
Funding
Open access funding provided by Johannes Kepler University Linz.
Author information
Authors and Affiliations
Contributions
JW designed and conceptualized study, acquired and analyzed the data, and drafted the manuscript. AL analyzed the data and drafted the manuscript. AT analyzed the data and revised the manuscript. JP acquired the data and revised the manuscript. TvO analyzed the data and revised the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
JW reports personal fees from Boehringer Ingelheim, personal fees from UCB, outside the submitted work. AL reports grants from Roche GmbH, outside the submitted work. Dr. von Oertzen reports grants, personal fees and non-financial support from Novartis Pharma, personal fees from Roche Pharma, personal fees from Biogen Idec Austria, personal fees from Liva Nova, grants from Grossegger and Drbal GmbH, grants from Merck, personal fees from Indivior Austria GmbH, personal fees and non-financial support from gtec GmbH Austria, personal fees and non-financial support from Boehringer-Ingelheim, personal fees from Philips, personal fees and non-financial support from UCB Pharma, personal fees from Almirall, personal fees from Eisai, outside the submitted work; and he is webeditor in chief of the European Academy of Neurology (EAN), co-chair of the EAN scientific panel for epilepsy, and vice president of the Österreichische Gesellschaft für Epileptologie (Austrian ILAE chapter). JP and AT report no disclosures.
Ethics approval
Ethics approval was waived by the Ethics Committee of Upper Austria. The manuscript does not contain clinical studies or patient data.
Availability of data and material
All data are included in the manuscript.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wagner, J.N., Leibetseder, A., Troescher, A. et al. Efficacy and safety of intravenous immunoglobulins for the treatment of viral encephalitis: a systematic literature review. J Neurol 269, 712–724 (2022). https://doi.org/10.1007/s00415-021-10494-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-021-10494-w