
Abstract
Different studies have established that the mineralization stages of the second mandibular molar can be used in forensic age estimation. Nowadays, the estimate’s accuracy is an ethical concern, producing as few false positives (individuals incorrectly classified as older than a determined threshold) and false negatives (individuals incorrectly classified as younger than a determined threshold) as possible. Some have hypothesized that changes in teeth number may influence tooth mineralization, altering the age estimate process. This paper analyzes whether third molar agenesis affects the second mandibular molar mineralization time frame. To do so, 355 orthopantomograms were evaluated for third molar agenesis, and the second mandibular molar mineralization stage was assessed using the Demirjian stages. Student’s t-test was used to compare the difference in the mean age at which the various stages of 37 mineralization were reached in the groups with and without third molar agenesis. The level of statistical significance was set at 5%. The results pointed to a delay in second mandibular molar mineralization in the case of agenesis, suggesting the need to consider this when estimating age using dental techniques.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the last few years, ethical issues involving age estimation have been discussed [1,2,3,4]. Many authors address ethical issues related to the use of radiographic methods [5], but other questions, namely regarding the accuracy of the assessment, may arise. Focardi et al. [1] point out the necessity of the method of assessment being accurate, with as few false positives (individuals incorrectly classified as older than a determined threshold) and false negatives (individuals incorrectly classified as younger than a determined threshold) as possible. These concerns had also been raised by Garamendi et al. [6] who introduced the concept of ethical and technical errors regarding the overestimation and underestimation of age. In this manner, several attempts to enhance the accuracy of age estimation have been performed, and many pieces of research have been performed considering other factors that may affect dental age estimation techniques, namely socioeconomic status, population affinity, chromosomal anomalies, and diseases, among others [7,8,9,10,11]. The presence of agenesis, i.e., the congenital absence of teeth, has also been referred to as a variable to consider in age estimation [12, 13]. Dental agenesis or hypodontia is one of the most common anomalies in the development of human dentition [14] and is frequently associated with several other oral abnormalities [15,16,17]. The incidence of missing teeth may vary considerably depending on dentition and demographic or geographic profiles, and distinct patterns of agenesis have been detected in the permanent dentition (i.e., unilateral agenesis more common than bilateral; third molars (3M) and second pre-molars commonly missing in all quadrants and/or combinations of these two tooth types and the incisors) [14]. Sex also influences the prevalence rates of agenesis in both dentitions, which are significantly higher in females than males (3:2, respectively) [14].
As stated, dental agenesis also seems to be associated with delayed dental development. The permanent second mandibular molar (2M) erupts between 12 and 14 years of age. However, the root development is complete by 14–16 years of age. Multiple studies were carried out and confirmed the validity of the permanent mandibular second molar as an age marker in these age groups [18,19,20,21]. Yet, little is known about how tooth number variation can affect its mineralization process. This study aims to evaluate if the dental development of patients with agenesis is delayed, compared to a control group, particularly if there is an alteration in the pattern of mineralization of tooth 37 in individuals with agenesis of the 3M.
Materials and methods
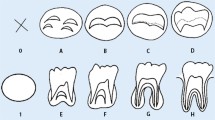
We have assessed 355 orthopantomograms (OPG) from patients from the Faculty of Dental Medicine of the University of Porto clinical services. The inclusion criteria were as follows: age between 9 and 15 years, Portuguese nationality, absence of a clinical history of mandibular third molar extraction, and having at least one intact mandibular second molar. Exclusion criteria were as follows: poor quality of OPG and evidence of pathology, local or systemic, and capable of influencing normal tooth development. OPGs were done for diagnostic purposes only, not specifically for this study. We collect data for two subsamples: S1, with no 3M agenesis, and S2, with individuals with at least one 3M agenesis. We have registered the age and sex of each participant. The total sample consisted of 187 males and 168 females, whose age distribution can be seen in Table 1. The age distribution by age group and sex is described in Table 2. The orthopantomograms were classified, assessing the presence of third molars and recording the mineralization phase using the stages proposed by Demirjian et al. [22].
S1 (n = 212) had mostly males (55.66%) aged between 10.15 and 14.98 years (mean = 12.47, standard deviation (sd) = 1.32); females’ mean age was 12.50 (sd = 1.33), ranging from 10.01 and 14.81 years.
As for S2, 40.3% had at least one tooth missing, affecting 69 (36.9%) males and 74 (44.0%) females. Table 3 depicts the number of third molar agenesis according to sex.
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) software, version 27.
Intra- and inter-observer errors were analyzed for the second molar mineralization stage, classifying a random sample of 20 OPG twice, by the same observer, with a 24-h gap, and by the two observers separately. Results were assessed using the Cohen’s kappa test. The inter-observer agreement showed substantial and significant agreement (kappa values of 0.882 (p < 0.001), and in the analysis of the intra-observer, the value obtained indicated a very high agreement, with k = 0.888 (p < 0.001).
Descriptive statistics were performed, with categorical variables described using frequencies and percentages and continuous variables using mean, standard deviation, and maximum and minimum values.
The chi-square test was used to verify possible associations between the agenesis of the third molars and the mineralization stage of the lower left second molar (37). The Spearman rank correlation was used to assess the correlation between the 3M agenesis number and 2M. Finally, Student’s t-test was used to compare the difference in the mean age at which the various stages of 37 mineralization were reached in the groups with and without third molar agenesis. The level of statistical significance was set at 5%.
The present study obtained a favorable recommendation from the Ethics Committee for Health of the FMDUP (recommendation n° 17/2022).
Results
At least one 3M agenesis was found in 69 (36.9%) males and 74 females (44%). The frequency of agenesis by 3M is depicted in Table 4. It was found that, in males and females, the most frequent agenesis was the upper 3M (53.47% and 55.55%, respectively).
Table 5 shows the sample distribution concerning the 37 mineralization stages by sex and age. Stage G was the most frequent in males and females (50.8% and 47.0%, respectively). The earliest mineralization stage found was stage D in both sexes (0.5% in males and 1.2% in females). It was found that at 10 years old, stage F is more frequent; between 11 and 13 years, stage G is more recurrent; and at 14 years old, stage H is more common.
Third molar agenesis had a statistically significant association with second molar mineralization stages in both sexes (p = 0.049 and p = 0.028 for males and females, respectively). In both sexes, equal or more advanced maturation stages were seen in individuals without agenesis.
The maxillary 3M agenesis was associated with 37 mineralization stages in the age groups of 13 and 14 years old (p = 0.05 and p < 0.001, respectively) in males. As for females, there was a statistically significant association with 37 stages only in the age group of 11 years old. As for mandibular agenesis, there was a significant association with 37 stages in the 14-year-old males (p = 0.002) and with the 13-year-old age females (p = 0.015).
The number of 3M agenesis had a low but statistically significant negative correlation coefficient with 2M stage attainment in both sexes (Table 6).
As for the difference between the mean age at the different 37 mineralization stages, only stage G attainment, both for boys and girls, depicted differences (p < 0.05) between both groups, with the children with agenesis displaying a higher mean age of stage attainment (Table 7). Stage D was not assessed since both sexes had no S1 (no agenesis) cases.
Discussion
Dental maturity has been considered a suitable indicator of chronological age and regarded as superior to the stature and skeletal methods for evaluating an individual’s somatic maturity. So, it is considered a valuable tool to estimate biological age in forensic or archaeological studies. Yet, for accuracy improvement, other factors have been considered important when applying dental age estimation techniques, and agenesis is thought to be one of those factors.
Our study points to delayed dental maturation of the second mandibular left molar in individuals with at least one 3M agenesis, being this effect more pronounced as the number of 3M agenesis increases. This result agrees with the one obtained by Lebbe et al. [23] pointing out that the total number of agenesis needs to be considered when estimating age, as having more teeth agenesis is negatively correlated with dental age.
The effect of each tooth is, however, not clear. The maxillary 3M agenesis was associated with 37 mineralization stages in the 13- and 14-year-old males, and in females, only with the 11-year-old. As for mandibular agenesis, there was a significant association in 14-year-old males and 13-year-old females. Thus, maxillary agenesis may have an effect earlier than mandibular agenesis, and the effects of 3M agenesis are perceived in girls first.
This influence is difficult to explain. It may be that, at some ages, mineralization is more susceptible to congenitally absent teeth, making some stages more prone to this influence. The results comparing mean age in both groups (S1 and S2) support this hypothesis as stage G was the only one to depict statistically significant differences. In our case, the more susceptible ages, based on the greater number of associations, are 11 years old for females and 14 years old for males, which, in the Portuguese population, coincides with the pre-puberty ages [24, 25].
As for other studies, to date, to the best of our knowledge, this is the first study analyzing the third molar agenesis impact on second mandibular molar mineralization. Other investigators addressed delayed mineralization of permanent canines, premolars, and second molars in individuals with missing teeth, not including third molars [13, 26]. Daugaard et al. found that the second premolar unilateral absence is associated with a tooth mineralization delay on the same and the contralateral side [13]. Our research did not study the second lower right molar mineralization stages, so we cannot assess the described effect. The same authors also reported a relationship between missing second premolars and delayed second molars in girls but not boys. Our investigation does not confirm their findings, as the effect was seen in both sexes; Ruiz-Mealin et al. [26] did not also report sex differences in dental maturation delay in patients with agenesis. Yet, our results point to more robust differences between groups in females (p = 0.028 and p = 0.049, for females and males, respectively). This latter finding of differential effects in females and males may be of particular interest concerning sex differences in dental development, and the fact that, in our sample, the effects seem to be more pronounced in females suggests that this is most likely a substantial finding and not merely a consequence of multiple statistical tests.
Further studies also account for this effect of delayed teeth mineralization. Tunç et al. [27] reported a mean difference of the estimated dental age of 0.3 years between the agenesis and the control group. Similar results were obtained by other authors [28,29,30], who also reported the differences being more expressive in females.
The relevance of performing this study concerning specifically the second molar mineralization relates to the fact that, in some countries, 14 is the limit of criminal liability. For instance, in Italy, the subject may be liable from 14 to 18 years, depending on the degree of maturity reached [1]. Other reasons may relate to age estimation of victims of sex crimes. In Portugal, the 172nd article of the Portuguese Penal Code determines different sentences for abuse of minors if they are over or under 14 years of age [20, 21]. Regardless, the underestimation or overestimation of age in this age group caused by technical errors may conflict with ethical issues since the penalties applied will be inadequate. The error of the estimated age being different from the real age becomes even more relevant in child abuse or child pornography scenarios since the punishments are more severe in case the victim is younger than 14 years old [20].
Another point we would like to address is the methodology of 37 staging. Being a two-rooted tooth, and because the mineralization process does not happen simultaneously in both roots, we have staged 37 according to the root that displayed the more advanced mineralization stage (i.e., the one that would give the individual the higher age). We recognize that usually, it is the other way around. Yet, in this case, a higher age estimation, i.e., being older, leads to a better (more favorable) penal measure for the offender. In this way, we believe that by doing so, we favored technical and not ethical errors.
As for limitations, we cannot tell if our sample with no agenesis depicts a “normal development rate of the second molar,” but as no other factors were identified, we have assumed it does. Still, other factors can modify stage attainment [7, 9]. Nevertheless, when compared with a study in a similar population [20], our non-agenesis subsample depicted similar Demirjian’s stage attainment ages.
We also recognize that by using the Demirjian stages (or any other), we introduce large uncertainties since the assigned stage is attained, and suddenly, it goes from one stage to the next. Still being so widely used, it allows for comparison with other studies; additionally, stages (particularly Demirjian stages) are frequently used as markers or thresholds for given ages [31,32,33], and in this sense, this study can benefit those practices.
Finally, we recognize that the effect is discrete, and the differences in the development of tooth 37 are minor. If a p-value 0.01 instead of 0.05 was adopted, not so much would be significant.
Conclusions
The results indicate a delay in the development and calcification of the second molar when there is agenesis of a third molar. This effect is slight and more pronounced in females, increasing with the number of 3M agenesis. This must be taken into consideration when dealing with the 14-year-old thresholds, as dental age estimates can, in these situations, lead to an underestimation of age and, in child abuse, to a more severe penal measure for the offender.
References
Focardi M, Pinchi V, De Luca F, Norelli GA (2014) Age estimation for forensic purposes in Italy: ethical issues. Int J Legal Med 128(3):515–522
Rudolf E, Comments to Focardi et al (2015) Age estimation for forensic purposes in Italy: ethical issues. Int J Legal Med 129(6):1271–1273
Roberts G, Lucas VS, McDonald F, Camilleri S, Jayaraman J, Davies D, Moze K (2017) In our opinion. Br Dent J 222(12):918–921
Hancocks S (2017) Agreed; but if...? Br Dent J 222(1):1
Aynsley-Green A (2009) Unethical age assessment. Br Dent J 206(7):337
Garamendi PM, Landa MI, Botella MC, Aleman I (2011) Forensic age estimation on digital X-ray images: medial epiphyses of the clavicle and first rib ossification in relation to chronological age. J Forensic Sci 56(Suppl 1):S3–S12
Caldas IM, Cardoso HFV (2021) Socioeconomic differences in permanent teeth mineralization of Portuguese girls and boys from Porto. Portugal Anthropol Anz 78(4):267–277
Cardoso HF, Heuze Y, Julio P (2010) Secular change in the timing of dental root maturation in Portuguese boys and girls. Am J Hum Biol 22(6):791–800
Carneiro JL, Caldas IM, Afonso A, Cardoso HF (2017) Examining the socioeconomic effects on third molar maturation in a Portuguese sample of children, adolescents and young adults. Int J Legal Med 131(1):235–242
Pinchi V, Vitale G, Pradella F, Farese L, Focardi M (2018) Dental age estimation in children with chromosomal syndromes. J Forensic Odontostomatol 36(1):44–52
Nuovo S, Bacigalupo I, Ginevrino M, Battini R, Bertini E, Borgatti R, Casella A, Micalizzi A, Nardella M, Romaniello R, Serpieri V, Zanni G, Valente EM, Vanacore N, Group JSIS (2020) Age and sex prevalence estimate of Joubert syndrome in Italy. Neurology 94(8):e797–e801
Gelbrich B, Hirsch A, Dannhauer KH, Gelbrich G (2015) Agenesis of second premolars and delayed dental maturation. J Orofac Orthop 76(4):338–350
Daugaard S, Christensen IJ, Kjaer I (2010) Delayed dental maturity in dentitions with agenesis of mandibular second premolars. Orthod Craniofacial Res 13(4):191–196
De Coster PJ, Marks LA, Martens LC, Huysseune A (2009) Dental agenesis: genetic and clinical perspectives. J Oral Pathol Med 38(1):1–17
Lourenco Ribeiro L, Teixeira Das Neves L, Costa B, Ribeiro GM (2003) Dental anomalies of the permanent lateral incisors and prevalence of hypodontia outside the cleft area in complete unilateral cleft lip and palate. Cleft Palate Craniofac J 40(2):172–175
Albashaireh ZS, Khader YS (2006) The prevalence and pattern of hypodontia of the permanent teeth and crown size and shape deformity affecting upper lateral incisors in a sample of Jordanian dental patients. Community Dent Health 23(4):239–243
Peck S, Peck L, Kataja M (1996) Prevalence of tooth agenesis and peg-shaped maxillary lateral incisor associated with palatally displaced canine (PDC) anomaly. Am J Orthod Dentofac Orthop 110(4):441–443
Lee SS, Byun YS, Park MJ, Choi JH, Yoon CL, Shin KJ (2010) The chronology of second and third molar development in Koreans and its application to forensic age estimation. Int J Legal Med 124(6):659–665
Almeida MS, Pontual Ados A, Beltrao RT, Beltrao RV, Pontual ML (2013) The chronology of second molar development in Brazilians and its application to forensic age estimation. Imaging Sci Dent 43(1):1–6
Fins P, Pereira ML, Afonso A, Perez-Mongiovi D, Caldas IM (2017) Chronology of mineralization of the permanent mandibular second molar teeth and forensic age estimation. Forensic Sci Med Pathol 13(3):272–277
Marques MR, Pereira MD, Caldas IM (2015) Forensic age estimation using the eruption of the second permanent mandibular molar: determining age over 14 years-old. Aust J Forensic Sci 47(3):306–312
Demirjian A, Goldstein H, Tanner JM (1973) A new system of dental age assessment. Hum Biol 45(2):211–227
Lebbe A, Cadenas de Llano-Perula M, Thevissen P, Verdonck A, Fieuws S, Willems G (2017) Dental development in patients with agenesis. Int J Legal Med 131(2):537–546
Reis M, Ramiro L, Godeau E, Matos M (2016) Age at menarche in Portuguese adolescents: a cross-sectional study with HBSC portuguese survey. Glob Adv Res J Educ Res Rev 5(4):55–62
Cardoso HF (2008) Secular changes in body height and weight of Portuguese boys over one century. Am J Hum Biol 20(3):270–277
Ruiz-Mealin EV, Parekh S, Jones SP, Moles DR, Gill DS (2012) Radiographic study of delayed tooth development in patients with dental agenesis. Am J Orthod Dentofac Orthop 141(3):307–314
Tunc ES, Bayrak S, Koyuturk AE (2011) Dental development in children with mild-to-moderate hypodontia. Am J Orthod Dentofac Orthop 139(3):334–338
Ardini YD, Bakar NA, Kamalul’lail NF, Rasdi NSM (2015) Assessment of dental development in children with hypodontia and hyperdontia: a case control study. IMJM 17(2):205–212
Rune B, Sarnas KV (1974) Tooth size and tooth formation in children with advanced hypodontia. Angle Orthod 44(4):316–321
Uslenghi S, Liversidge HM, Wong FS (2006) A radiographic study of tooth development in hypodontia. Arch Oral Biol 51(2):129–133
Guo YC, Chu G, Olze A, Schmidt S, Schulz R, Ottow C, Pfeiffer H, Chen T, Schmeling A (2018) Age estimation of Chinese children based on second molar maturity. Int J Legal Med 132(3):807–813
Zeng DL, Wu ZL, Cui MY (2010) Chronological age estimation of third molar mineralization of Han in southern China. Int J Legal Med 124(2):119–123
Gaeta-Araujo H, Oliveira-Santos N, Nascimento EHL, Nogueira-Reis F, Oenning AC, Groppo FC, Oliveira-Santos C (2021) A new model of classification of third molars development and its correlation with chronological age in a Brazilian subpopulation. Int J Legal Med 135(2):639–648
Acknowledgements
The authors would like to thank the anonymous reviewers for all the comments and suggestions that have greatly improved this manuscript.
Funding
Open access funding provided by FCT|FCCN (b-on).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by FC and CIM. The first draft of the manuscript was written by FC, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ferreira, C., Caldas, I. Does third molar agenesis influence the second lower molar mineralization?. Int J Legal Med 138, 911–916 (2024). https://doi.org/10.1007/s00414-023-03128-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-023-03128-5