
Abstract
Purpose
To investigate associations between dizziness, hearing loss, medication, and self-perceived health in the region of Lolland-Falster in Denmark.
Methods
A cross-sectional population-based study using data from questionnaires and physical examinations between February 8th, 2016, and February 13th, 2020. Individuals aged 50 years or above in the region of Lolland-Falster were randomly invited to participate.
Results
Of 10,092 individuals (52% female), the mean age was 64.7 and 65.7 years for females and males, respectively. 20% reported dizziness during the past 30 days, and prevalence increased with age. 24% of dizzy females suffered from falls compared to 21% of males. 43% sought treatment for dizziness. Logistic regression revealed a higher odds ratio of dizziness in groups with poor self-perceived health (OR = 2.15, 95% CI [1.71, 2.72]) and very poor self-perceived health (OR = 3.62 [1.75, 7.93]) compared to moderate self-perceived health. A higher OR was found for seeking treatment for dizziness in the group that had experienced falls (OR = 3.21 [2.54, 4.07]). 40% reported hearing loss. Logistic regression revealed a higher OR for dizziness in the group with severe hearing loss (OR = 2.40 [1.77, 3.26]) and moderate hearing loss (OR = 1.63 [1.37, 1.94]) compared to no hearing loss.
Conclusion
One of five participants reported dizziness during the last month. Dizziness was negatively associated with self-perception of good health also after adjusting for comorbidities. Almost half of the dizzy participants sought treatment for dizziness and 21% experienced falls. Identification and treatment of dizziness are important to prevent falls from happening.
Clinical trial registration
http://www.clinicaltrials.gov (NCT02482896).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dizziness and vertigo are among the most common complaints in the healthcare system, affecting an estimated 15–35% of the population at some point in life [1]. Dizziness as a symptom is non-specific and may arise from several organ systems. Some of the most frequent reasons are vestibular, neurological, and cardiovascular disorders. Furthermore, dizziness often arises due to the side effects of medication.
In 2008, a national health interview survey found that 24.2 million adults in America (corresponding to 11.1% of the included individuals) had experienced dizziness during the past 12 months [2]. Among participants aged 65 and above, 19.6% reported a problem with dizziness or unsteadiness in the preceding 12 months [3], and women were more often affected than men (21% vs. 18%). These results have been confirmed by other similar studies [4, 5]. Concerning the quality of life and functional status, 37.3 million elderly individuals corresponding to 27.4% reported that balance problems prevented them from participating in activities such as social events, exercise, and driving [3]. This was also confirmed by a cohort study with 2751 participants reporting that adults affected by dizziness/vertigo generally had lower quality of life scores [6].
The Lolland-Falster Health Study (LOFUS) is a household-based population study based on people living in the two Danish islands of Lolland and Falster. Approximately 103,000 inhabitants live in this region, which is considered one of the most socio-economically disadvantaged areas in Denmark [7]. An analysis of the use of doctors, use of medication, and life expectancy, done in 2010 by the Workers Union, showed that the region has a higher occurrence of sickness and a lower average life expectancy than the rest of Denmark [8].
LOFUS was initiated to gain knowledge on determinants of health in a socio-economically disadvantaged and mainly rural area of Denmark using questionnaires, physical examinations, and biological samples hypothesizing that lifestyle, environment, and heritage together are risk factors for disease [7]. Other similar studies but in highly urbanized areas have been performed in Denmark [9].
In this report, we focus on dizziness, and hearing loss reported by the elderly participants in the LOFUS cohort. We would like to specify that we use dizziness as an umbrella term including vertigo and unsteadiness, as the Danish language does not distinguish between these. We hypothesize that these symptoms are frequent and are associated with poorer health perception and comorbidities. Also, we explore the use of doctors for these complaints.
Methods
Study design
From February 8th, 2016, to February 13th, 2020, 19,000 participants aged 0–96, participated in LOFUS. Participants answered questions concerning both ear-, nose-, and throat problems and socioeconomic status.
Invitation, booking procedure, and visit
Individuals aged 18 years or above in the region of Lolland-Falster were randomly invited to participate in the Health Study. Invited individuals who agreed to participate were booked for an appointment in one of three static sites. The visit included a dialogue concerning written informed consent, followed by a physical examination. Thereafter, participants received a confirmation letter including a link and password to a web-based questionnaire [7].
Eligibility criteria
The focus of the present study was dizziness. Dizziness was used as an umbrella term including vertigo and unsteadiness, as the Danish language does not distinguish between these. Inclusion criteria were age above 50 years and having answered the sub-questionnaire on dizziness. Exclusion criteria were incapacitated people with guardians, individuals without a permanent residence, inhabitants with address protection, and inhabitants unable to understand Danish or English [7].
Sample population
The sample population was drawn from the target population of around 103,000 inhabitants in the region of Lolland-Falster from the two municipalities Lolland or Guldborgsund [7].
Questionnaire-data
The questions are shown in Table 1.
Physical measurements
Height, weight, creatinine, eGFR, sodium, potassium, hemoglobin, cholesterol value, and systolic and diastolic blood pressure were obtained.
Sociodemographic data
Age in years, gender, marital status (married, separated/divorced, widowed, single), educational level (less than high school, high school, a bachelor’s degree, advanced degree, other), occupation (unemployed, out of the labor market, in labor, studying or training, work in the home, other), and the number of individuals in the household.
Statistical analyses
All data management and statistical analyses were performed using R, version 4.1.1. Logistic regressions were applied to test for bivariate associations. For ordinal data, we applied the Cochran-Armitage test for trend.
A multivariate binary logistic regression model was fitted to explain binary variables from several quantitative and qualitative covariates. For the logistic regression, the participants answering ‘do not know’ to dizziness were removed. A Hosmer–Lemeshow test was then performed to check for the goodness of fit. Odds-ratio (OR) estimates, 95%-confidence intervals (CI), and p-values were derived from the logistic regression models.
Ethics and dissemination
Region Zealand’s Ethical Committee on Health Research has approved LOFUS (Reg: SJ-421). All data storage and management for this study were approved by the Regional Data Protection Agency of Zealand (REG-065–2021 & REG-24–2015), and the use of data was accepted by the LOFUS steering committee. LOFUS is registered on http://www.clinicaltrials.gov (NCT02482896).
Results
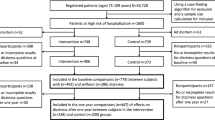
In total, 11,057 individuals above 50 years of age attended the LOFUS study. Of the 11,057 individuals, 10,092 answered the questions regarding dizziness and were eligible for this study. 5279 (52%) were female, and 4813 (48%) were male. The mean age was 64.7 (range: 50.1 to 96.6), and 65.7 (range: 50.0 to 95.6) for females and males, respectively. Of the 10,092 individuals included in this study, almost 20% had experienced dizziness during the past 30 days. For baseline characteristics, see Table 2.
Gender effect
In total, 22% of the females reported dizziness compared with 17% of the males (Table 2). Dizziness was significantly more frequent in females than in males in all age groups. In the logistic regression model, a statistically significant difference in odds of dizziness between the female and male sex was found (OR = 1.52, 95% CI [1.34, 1.74]), see Table 3.
Age effect
The prevalence of dizziness increased with increasing age, being approximately 1.75 times more frequent in > 80 years of age compared with 50–59 years of age. When divided into age groups, a statistically significant difference in odds of dizziness was found for the age range 70–79 years old (OR = 1.19, 95% CI [1.01, 1.41]) and > 80 years old (OR = 1.67, 95% CI [1.30, 2.15]).
Occupation
A univariate analysis showed a statistically significant difference in dizziness between different categories of education (Table 4). When the occupational position was tested in the multivariate logistic regression, only “other forms of retirement”, “long-term sickness” and “student/apprentice” were statistically significant. However, the number of participants answering “student/apprentice” and “long-term sickness” were very small (Table 3).
Antihypertensive and diuretic medicine
Dizziness was significantly more frequent in participants being treated with diuretics or antihypertensive medications (Table 4). In the logistic regression model, the use of antihypertensive medication was statistically significant (OR = 1.15, 95% CI [1.01, 1.30]. As diuretic medicine was included in the category of antihypertensive medicine, the use of diuretic medicine was not tested separately in logistic regression.
Hearing loss
Of 1964 participants suffering from dizziness in the past 30 days, 40% also reported some degree of hearing loss (mild, moderate, or severe). Males reported more frequent hearing loss. The prevalence of hearing loss with dizziness is seen in Table 4. Logistic regression revealed a statistically significant increase in odds of dizziness between individuals with hearing loss and without hearing loss (mild hearing loss: OR = 1.33 [95% CI 1.15, 1.53], moderate hearing loss: OR = 1.63 [95% CI 1.37, 1.94], and severe hearing loss: OR = 2.40 [95% CI 1.77, 3.26]) when adjusting for covariates and suspected confounders such as age.
Self-perception of health
In logistic regression, a significant difference in odds of dizziness was seen between different degrees of self-perceived health. Poor self-perceived health and very poor self-perceived health revealed odds ratios of 2.15 (95% CI 1.71, 2.72), and 3.62 (95% CI 1.75, 7.93), respectively. Oppositely, good- and excellent self-perceived health revealed odds ratios of OR = 0.36, 95% CI (0.32, 0.40), and OR = 0.14, 95% CI (0.10, 0.18).
Experiencing falls and seeking treatment due to dizziness
Of the 1964 participants answering “yes” to dizziness during the past 30 days, 1951 participants answered the question about the occurrence of falls in relation to their dizziness (Table 5). 24% of the women suffering from dizziness in the past 30 days had experienced falls compared to 21% of men. An increase in the occurrence of falls was seen with increasing age in both sexes. In logistic regression, the best predictors of falls were very poor, poor, and good self-perceived health with an OR = 3.09, 95% CI (1.27–7.57), OR = 1.58, 95% CI (1.13, 2.21), and OR = 0.52, 95%- CI (0.4–0.67), respectively. Furthermore, increasing age also increased the odds ratio of falls, see Table 6.
A total of 1,953 participants suffering from dizziness during the past 30 days answered the question about seeking treatment for their dizziness. 43% of both females and males stated that they had sought treatment for their dizziness (Table 5). Seeking treatment for dizziness increased with increasing age for men, however, the biggest increase for females was seen in the age group of 60–70 years, where almost 50% sought treatment for their dizziness.
Logistic regression for “seeking treatment for dizziness” as an outcome showed that the occurrence of falls due to dizziness was the best predictor of seeking treatment for dizziness with an OR = 3.21, 95% CI (2.53, 4.08), please see Table 7. Furthermore, good or excellent self-perceived health decreased the odds of seeking treatment (good self-perceived health OR = 0.8, 95% CI (0.65–0.99), excellent self-perceived health OR = 0.44, 95% CI (0.24–0.85).
Discussion
Dizziness is among the most common complaints in populations. Dizziness is associated with a significant degree of handicap, perception of low health, and occupational disability. Approximately one in five of the population in our study reported dizziness during the past month which is consistent with other studies reporting the monthly prevalence of dizziness [10, 11]. However, the mean age in our study was 65 years, which is not comparable to the mean age in other studies. In the United Kingdom, Yardley et al. found that 23% experienced dizziness during the past month (mean-age for females was 38.7) [10]. In Norway, Wiltink et al. found that 15.8% experienced dizziness during the past month in a population with a mean age of 48.8 [11].
The prevalence of dizziness increased with age, and there was a female predominance in our data. These findings are supported by several other studies [12, 13]. If a dizzy individual seeks treatment from a medical doctor, it may indicate that dizziness is severe and possibly influences the quality of life. This was the case in 43% of the participants in our study.
We demonstrated that a good predictor for seeking treatment for dizziness was the occurrence of falls in relation to dizziness. This was not unexpected. However, if many dizzy individuals only seek help after experiencing falls in relation to dizziness, it may be difficult to prevent falls. Various reasons could explain why individuals suffering from dizziness do not seek treatment from a medical doctor. One reason among others could be that the individual does not feel that the dizziness complaint is being taken seriously by their general practitioner or other health professionals. This could be due to the fact that many find it difficult to diagnose and treat dizziness but also that comorbidities often are present. Another reason could be relatives who think that it is normal to get dizzy with increasing age and therefore do not respond to the complaint. One might argue that an invitation for vestibular rehabilitation could help at least some of the patients as well as society by preventing fractures, especially hip fractures, and other events to happen.
We found that hearing loss and dizziness are often associated. This is probably mainly due to age-related factors like neurodegenerative processes in the elderly. The association is not surprising.
As regards subjective general health, we found that 13% experienced a “very poor” or “poor” subjective general health with a statistically significant difference between the dizzy and non-dizzy groups. This is congruent with data from Sweden where 18% reported “very poor” or “poor” health [14]. However, the data from Sweden reporting “very poor” or “poor” health might be a bit higher compared to our data because included patients were 79 years of age compared to our sample with a mean age of 65 years. Data from Brazil conclude the same: that self-perception of health was rated lower in dizzy- than in non-dizzy individuals [13].
As dizziness as a symptom is non-specific and may arise from several organ systems, it is not surprising that a correlation was found with general health, use of medication, and hearing loss. Consequently, the findings do not allow any specific conclusions on the contributing factors to dizziness and falls. Furthermore, the directionality of causalities may be in two or multiple ways.
Limitations and strengths
This is a cross-sectional questionnaire survey that only allows for possible associations but does not allow for causative explanations. In addition, participants who answered this questionnaire may be subject to bias by indication. A study investigating the degree of bias in LOFUS with logistic regression found that odds ratios for participation increased with income, education level, and employment status, among married individuals, Danish citizens, middle-aged individuals (aged 50–69 years), and female gender. Briefly, significantly higher participation of women and individuals of higher socioeconomic status was found, implying that people of lower socioeconomic status were underrepresented in LOFUS, in line with other cohort studies [15].
The strength is that the survey includes more than 10,000 participants in the age group for dizziness. Also, participants were not asked questions concerning possible associated items in the same section as dizziness. This makes it quite speculative that participants were skewed in their answers.
Conclusions
The prevalence of dizziness in citizens aged 50 years and above and participating in the Lolland-Falster Health Study was 20% which is in line with other similar studies. Citizens suffering from dizziness were negatively associated with self-perception of health also after adjusting for other comorbidities. 43% of dizzy patients sought treatment for their dizziness. 23% of the dizzy citizens experienced falls due to dizziness. The occurrence of falls was an indicator of seeking medical examination. Identification of dizziness, as well as treatment such as vestibular rehabilitation, is important to prevent falls from happening in the nearby future.
Data Availability
The data that support the findings of this study are available on request from the corresponding author, CG. The data are not publicly available as it contains information that could compromise the privacy of research participants.
References
Neuhauser HK (2016) The epidemiology of dizziness and vertigo. Handb Clin Neurol 137:67–82
Lin HW, Bhattacharyya N (2014) Impact of dizziness and obesity on the prevalence of falls and fall-related injuries. Laryngoscope 124(12):2797–2801
Lin HW, Bhattacharyya N (2012) Balance disorders in the elderly: epidemiology and functional impact. Laryngoscope 122(8):1858–1861
Olsson Möller U, Midlöv P, Kristensson J, Ekdahl C, Berglund J, Jakobsson U (2013) Prevalence and predictors of falls and dizziness in people younger and older than 80 years of age–a longitudinal cohort study. Arch Gerontol Geriatr 56(1):160–168
Stevens KN, Lang IA, Guralnik JM, Melzer D (2008) Epidemiology of balance and dizziness in a national population: findings from the English Longitudinal Study of Ageing. Age Ageing 37(3):300–305
Gopinath B, McMahon CM, Rochtchina E, Mitchell P (2009) Dizziness and vertigo in an older population: the Blue Mountains prospective cross-sectional study. Clin Otolaryngol 34(6):552–556
Jepsen R, Egholm CL, Brodersen J, Simonsen E, Grarup J, Cyron A et al (2020) Lolland-Falster Health Study: study protocol for a household-based prospective cohort study. Scand J Public Health 48(4):382–390
Juul JS, Holme A (2010) Pilskæv fordeling i sundheden - yderkantsdanmark holder for Arbejderbevægelsens erhvervsråd. https://www.ae.dk/files/dokumenter/analyse/ae_pilskaev-fordeling-i-danskernes-sundhed-yderkantsdanmark-holder-for.pdf. Accessed 26 March 2021
Kårhus LL, Møllehave LT, Osler M, Jørgensen T, Linneberg A (2022) Population-based epidemiology: the Glostrup population studies 1964–2021. Scand J Public Health 50(7):1007–1011
Yardley L, Owen N, Nazareth I, Luxon L (1998) Prevalence and presentation of dizziness in a general practice community sample of working age people. Br J Gen Pract 48(429):1131–1135
Wiltink J, Tschan R, Michal M, Subic-Wrana C, Eckhardt-Henn A, Dieterich M et al (2009) Dizziness: anxiety, health care utilization and health behavior–results from a representative German community survey. J Psychosom Res 66(5):417–424
Murdin L, Schilder AG (2015) Epidemiology of balance symptoms and disorders in the community: a systematic review. Otol Neurotol 36(3):387–392
de Moraes SA, Soares WJ, Rodrigues RA, Fett WC, Ferriolli E, Perracini MR (2011) Dizziness in community-dwelling older adults: a population-based study. Braz J Otorhinolaryngol 77(6):691–699
Lindell E, Kollén L, Johansson M, Karlsson T, Rydén L, Fässberg MM et al (2021) Dizziness and health-related quality of life among older adults in an urban population: a cross-sectional study. Health Qual Life Outcomes 19(1):231
Jepsen R, Wingstrand A, Abild SL, Ellervik C, Simonsen E, Rasmussen K et al (2020) Socio-economic determinants of participation in the Lolland-Falster health study. J Public Health 28(6):657–664
Acknowledgements
We would like to thank statistician Anna Mejldal from OPEN for reviewing the data analysis.
Funding
Open access funding provided by Zealand Region
Author information
Authors and Affiliations
Contributions
All authors contributed to the writing of the manuscript. Analysis of data were performed by CG. The first draft of the manuscript was written by CG and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors would like to disclose that we have no financial or non-financial interests that are directly or indirectly related to the work submitted for publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Grønlund, C., Djurhuus, B.D., Holm, E.A. et al. Self-reported dizziness, falls, and self-rated health in a rural population in Denmark. Eur Arch Otorhinolaryngol 280, 5329–5337 (2023). https://doi.org/10.1007/s00405-023-08061-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-023-08061-2