
Abstract
Introduction
Vocal loading capacity is an important aspect of vocal health and is measured using standardized vocal loading tests. However, it remains unclear how vocal fold oscillation patterns are influenced by a standardized vocal loading task.
Methods
21 (10 male, 11 female) vocally healthy subjects were analyzed concerning the dysphonia severity index (DSI) and high speed videolaryngoscopy (HSV) on the vowel /i/ at a comfortable pitch and loudness before and after a standardized vocal loading test (10 min standardized text reading, at a level higher than 80 dB (A) measured at 30 cm from the mouth).
Results
Changes in DSI were statistically significant, diminishing by 1.2 points after the vocal loading test, which was mainly caused by an increase of the minimum intensity. However, the pre-post comparison of HSV derived measures failed to show any statistically significant changes.
Conclusion
It seems necessary to analyze the effects of a standardized vocal loading test on vocal fold oscillation patterns with respect to softest phonation and phonation threshold pressure rather than comfortable pitch and loudness.
Level of evidence
2c
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vocal loading capacity is an important aspect of vocal health and a reduction in such capacity might be a sign of dysphonia. Especially for voice professionals, such as teachers, priests, actors, singers or employees in call-centers [1] vocal loading capacity is of special interest and an impairment of the capacity might result in economic problems. However, in clinical circumstances, measurement of vocal loading is not easy to perform.
Studies using accelerometers have been used to estimate the vocal dose representative of realistic daily voicing activity [2,3,4,5,6,7,8,9]. In this context, it was shown that the dose during professional voice use differs from normal voice use outside working hours [8]. Furthermore, the background noise was found to differ during the day [8]. However, in a recent study of teachers, the Lombard effect [10], voice adaptation by means of higher sound pressure level (SPL) during increased background noise, was not verified for all subjects [11]. In addition, it was shown that the level of vocal dose might vary greatly inter-individually. Therefore, such measurements using accelerometers do not necessarily show the extent to which the vocal dose is related to vocal problems or signs of vocal fatigue.
To measure such a relation, vocal loading tests have previously been established for clinical voice measurement. Such tests involve the patient/subject voicing at a minimum sound pressure level (SPL) for a given time. However, they vary in many ways: time intervals (10 min [6, 12,13,14], 16 min [15] up to hours [16] or repetitions such as 5 × 45 min [17]), the minimal sound pressure level (from 65 to 80 dB [12, 17, 18]), the distance to the sound level meter (from 2 m [17], 50 cm [19], 40 cm [20] or 30 cm [6, 12, 15], the spectral weighting of sound pressure level (A [6, 21] or C [18]), the type of vocalization (standardized text [13, 19], reading a text of the subject’s choice [17], counting numbers [22], vocalization of vowels [15, 18]), sitting or standing position [17] and whether the minimal SPL was changing in intervals during the test [13, 15, 19] or not [6, 12, 18]. Furthermore, there is no consistency in the analysis of such tests. In some cases pre-post comparisons were performed which analyzed a stroboscopic recording [16, 23], Phonation Threshold Pressure [24, 25], Voice Handicap Index (VHI [26]) [13], acoustic measures [13, 27, 28], visual analog scale [12] or the Dysphonia Severity Index (DSI [29]) [6, 12, 30]. In other examples the material captured during the test itself was analyzed for changes in fundamental frequency (ƒo), sound pressure level (SPL) and percentage of SPL below the specified level [31].
In previous studies, it was shown that a vocal loading task of reading a standardized text for 10 min whilst maintaining an SPL of more than 80 dB (A), measured at a distance of 30 cm, caused a drop of the DSI by approximately 0.5–1 point [12, 30]. In addition, it was shown that vocally healthy subjects were able to execute the test without breaks or failures to produce the target SPL [12]. Using accelerometers this vocal loading test also showed vocal doses comparable to teaching a 45-min lesson in a school class [6] which assumes transferability for analysis of realistic professional voice use.
Considering physiological factors, it could be assumed that vocal fatigue by vocal loading is a consequence of vocal fold oscillatory function. However, there are only a few studies analyzing vocal fold oscillatory characteristics with respect to vocal loading. Using high speed videoendoscopy (HSV) Lohscheller et al. [32] analyzed three subjects and Döllinger et al. [33] a single subject by means of phonovibrograms [34]. Both studies found that vocal loading led to changes in the left–right symmetry as well as opening and closing dynamics. However, in both studies, only a very small number of subjects were analyzed and no standardized vocal loading test was used.
The presented study aims to analyze vocal fold oscillation changes after a standardized vocal loading test in vocally healthy subjects using HSV, audio and electroglottographic (EGG) signals. It was hypothesized that vocal fold stiffness would increase due to the loading and, as a consequence, the glottal area waveform (GAW) derived open quotient (OQ) would increase due to vocal fatigue as measured by the DSI. Furthermore, it was hypothesized that such an increase would also be detectable using EGG signals.
Material and methods
After approval from the local ethical committee. 23 vocally untrained subjects took part (11 female, 12 male, age: 25–45 years), of whom 21 were included in this study. One subject had to be excluded from the dataset because of technical distortions in the audio signal, the other because of distortions in the electroglottographical (EGG) signal. None of the subjects had a medical history of vocal dysfunction or acute voice complaints. All subjects were non-smokers.
All subjects were asked to perform a standardized vocal loading test. Similar to previous studies [12, 30], the subjects were asked to read a standardized text (German Text: Das tapfere Schneiderlein, Grimm brothers) over a 10 min time frame maintaining an SPL higher than 80 dB (A), measured at a distance of 30 cm from the mouth. According to the German Society of Phoniatrics and Pediatric Audiologists the test was not performed in a sound treated environment, but a quasi-living room acoustic setting. The test was performed using the Lingwaves software (Wevosys, Forcheim, Germany). A red arrow on the computer screen was shown when the SPL was lower than the required 80 dB (A). From this vocal loading test, the fundamental frequency (ƒo, Hz), SPL [dB (A)] and the shortfall of the 80 dB criterion were calculated as a mean for each minute during the 10-min performance.
Before and after the vocal loading test, a voice range profile (Wevosys, Forchheim, Germany) with a sound level meter (Voltkraft 322, Hong Kong, China) placed at a distance of 30 cm from the mouth was performed. Furthermore, to establish the DSI, also the maximum phonation time (best of three attempts, vowel /a/, comfortable pitch and loudness) was measured and the audio signal from a sustained phonation was recorded for the calculation of the jitter.
Directly before and directly after the vocal loading test rigid high speed video endoscopy (HSV) was performed (HRES-Endocam 5562, Fa. Wolf, Knittlingen, Germany), recorded at 4000 frames per second. For this recording the subject was asked to sustain phonation on the vowel /i/ at comfortable loudness and pitch. Simultaneously, the audio signal using a standard microphone (Sennheiser KE 4–211-1, Sennheiser, Wedemark, Germany, mounted on the laryngoscope at a distance of approximately 10 cm to the lips) and the EGG signal (EG2- PCX2, Glottal Enterprises, Syracuse, USA) were recorded.
For the analysis of the HSV a time window of 1000 frames was segmented using the Glottis Analysis Tools Software (Division of Phoniatrics, University Hospital Erlangen, Germany). From the segmented glottis phonovibrograms were established, as described in detail in Refs. [35, 36]. After this, the Glottal Area Waveform (GAW) as well as the corresponding audio and EGG signal were analyzed using the Multi Signal Analyzer (Division of Phoniatrics, University Hospital Erlangen, Germany). Using this software, numerous numerical data analogous to the Glottal Analysis Tools could be calculated from the different signal types.
For this particular study, the variables are shown in Table 1. For the estimation of the EGG open quotient the Howard criterion [37] was used.
All statistical analyses were calculated with SPSS 21 (SPSS Inc., Armonk, NY, USA). For the analysis of pre-post differences paired Student’s t-tests were used. The level of significance was set to p = 0.05.
Results
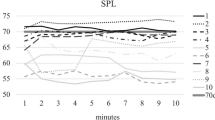
All subjects completed the vocal loading test without interruption. The results of the vocal loading test for SPL and ƒo for each minute of the test are shown in Fig. 1 and 2.

Mean sound pressure level (SPL) and percentage of SPL values below 80 dB (A) for the vocal loading test

Fundamental frequency for the vocal loading test for the female (left) and male (right) subjects
In the pre-post loading test comparison, the DSI showed a drop of the mean of 1.18 points (mean 8.34 vs. 7.16, p < 0.001, median 8.8 vs.7.2, Fig. 3).

Dysphonia Severity Index before (pre) and after (post) the vocal loading test
This drop was caused mainly by an increase of the lowest intensity (pre-post comparison for lowest intensity: 45.42 dB vs 48.21 dB, p < 0.01, highest fundamental frequency: 904.10 Hz vs 861.25 Hz, not significant, MPT: 24.21 s vs 22.41 s, not significant, jitter: 0.15% vs 0.15%, not significant). The lowest intensity change was statistically significant for both males and females. Whilst all other factors establishing the DSI failed to show statistically significant changes, the MPT was lowered in the pre-post comparison for males (27.24 s vs. 23.54 s, p < 0.05).
In both, the GAW open quotient and the EGG derived open quotient, there was no statistically significant change after the loading test (Table 2). Furthermore, other GAW, EGG and audio signal parameters failed to show any statistically significant change (Table 2).
The oscillatory patterns observed through phonovibrograms were not greatly influenced by the vocal loading. Figure 4 shows a representative phonovibrogram from subject Nr. 2.

Pre-post comparison of phonovibrogram for subject 2
There were no statistically significant differences in the pre–post comparison for the Phase Asymmetry Index, Speed Quotient, Speed Index, Stiffness or Amplitude Symmetry.
There was a high level of agreement for the GAW open quotient and the EGG derived open quotient for GAW values lower than 0.7 (trendline: y = 0.6183x + 0.2727, r2 = 0.5093), however no correlation for values above this (trendline: y = 0.0172x + 0.584, r2 = 0.0003, Fig. 5).

Glottal area waveform derived open quotient (OQ GAW) versus electroglottographic open quotient (OQ EGG)
The SPL during the HSV recording, recorded at a distance of 10 cm from the mouth, showed no correlation with the DSI or with the minimum intensity measured at 30 cm from the mouth after the HSV recording.
Discussion
This study analyses the effects of a standardized vocal loading test on vocal fold oscillation characteristics in vocally healthy subjects. In general, it was found that although the DSI diminished after the loading test, no statistically significant changes were found in the parameters representing vocal fold oscillatory characteristics that were considered.
In previous studies, it has been shown that vocal loading is considered an important indicator of vocal health and that vocal loading can be measured using standardized vocal loading tests [12, 13, 19, 22, 31]. Whereas dysphonic patients show interruptions during the loading [31] or short comings during the loading [19], healthy subjects are usually able to fulfil the requirements of such a test [12, 30]. In the present study, no interruptions or breaks occurred during the test and subjects generally maintained a volume above the target 80 dB (A) criterion. Furthermore, a drop of the DSI was present after the loading, indicating a sign of vocal fatigue. The amount of the drop of 1.2 was only slightly greater than in a previous study [12]. Therefore, it can be concluded that the vocal loading test had an effect on the vocal capacity of the subjects.
However, at the same time there were no statistically significant changes of the oscillatory characteristics measured from the glottal area waveform in the pre-post design. The DSI was mainly caused by a rise of the minimal intensity for both genders and an additional small drop of MPT for the male subjects only. Because subjects were asked only to produce comfortable pitch and loudness, it might have been the case that the loss of soft phonation after the vocal loading test is not reflected in the HSV derived data. The rise of minimal intensity should be related to increased stiffness of the vocal folds with the consequence of increased subglottic pressure and fundamental frequency [38]. However, the HSV data failed to show any statistically significant changes for comfortable pitch and loudness in the pre-post setting. It might be that an increase in stiffness contributes more to vulnerable parts of voice production, such as the phonation threshold pressure which is closely related to the minimum intensity in the voice range profile as has been shown previously [24, 25]. As a consequence, it should be stated that it is necessary to analyze vocal fold oscillations with respect to softest loudness and phonation threshold pressure rather than comfortable pitch and loudness to verify signs of vocal fatigue associated with a vocal loading test. In this context, it should be mentioned that the analysis of the EGG signal with respect to the open quotient might be problematic. As already stated in previous studies [39] the agreement with the GAW-derived open quotient was great up to a value of approximately 0.7. However, above this value the EGG derived open quotient no longer provides valid data.
Furthermore, this discrepancy in results between the DSI and other parameters suggests that comfortable speaking voice is not greatly affected by this standardized loading task. Although signs of fatigue are present by means of the drop of DSI, people are able to continue maintaining their voice at comfortable loudness and pitch. However, it could be speculated that a greater dose would also affect the mean speaking voice. Therefore, it could be of interest for future studies to analyze how much dose would cause modifications of comfortable pitch and loudness. Furthermore, it could be of interest to observe whether greater drops in the DSI could increase the risk of influencing comfortable pitch and loudness.
There are some important limitations of the presented study. This study included vocally healthy subjects only. It cannot be excluded that dysphonic patients would react differently concerning such a standardized vocal loading test. In this respect, it could also be assumed that the overall "effective vocal load" (i.e. effect of multiple parameters) might be different if there is already another vocally taxing factor that is influencing the glottis (e.g. reflux, smoking, allergies, inhalative medications, etc.), even in non-dysphonic subjects. Although other diseases including reflux or pulmonary diseases and smoking history have been excluded by medical history no control of hydration was performed. In a previous study, it has been shown that hydration might impact vocal loading capacity [40]. Furthermore, the loading with 10 min was rather short. Usually, the realistic vocal loading during the day is in voice professionals much greater. It remains unclarified if oscillation patterns at comfortable pitch could be changed in greater doses of vocal loading. Last, HSV was recorded with a rather low sampling rate of 4000 fps. Additionally, it was performed using a rigid endoscopy, which could influence vocal tract shape by a greater amount. It was shown in physiological studies that HSV is possible with a sampling rate of 20,000 fps using flexible endoscopy [41]. The system used in this study, however, had the great advantage of color images, which improved the segmentation process.
Conclusions
A vocal loading test of text reading at 80 dB(A) or greater measured at 30 cm distance from the mouth influences the dysphonia severity index but not vocal fold oscillations at comfortable pitch in non-dysphonic subjects.
References
Richter B, Echternach M (2010) Stimmärztliche Betreuung und Behandlung von Sängern [Diagnostics and therapy in professional voice-users]. HNO 58:389–398
Mehta DD, Van Stan JH, Zanartu M et al (2015) Using ambulatory voice monitoring to investigate common voice disorders: research update. Front Bioeng Biotechnol 3:155
Mehta DD, Van Stan JH, Hillman RE (2016) Relationships between vocal function measures derived from an acoustic microphone and a subglottal neck-surface accelerometer. IEEE/ACM Trans Audio Speech Lang Process 24:659–668
Svec JG, Titze IR, Popolo PS (2005) Estimation of sound pressure levels of voiced speech from skin vibration of the neck. J Acoust Soc Am 117:1386–1394
Titze IR, Hunter EJ, Svec JG (2007) Voicing and silence periods in daily and weekly vocalizations of teachers. J Acoust Soc Am 121:469–478
Echternach M, Nusseck M, Dippold S, Spahn C, Richter B (2014) Fundamental frequency, sound pressure level and vocal dose of a vocal loading test in comparison to a real teaching situation. Eur Arch Otorhinolaryngol 271:3263–3268
Richter B, Nusseck M, Spahn C, Echternach M (2016) Effectiveness of a voice training program for student teachers on vocal health. J Voice 30:452–459
Sodersten M, Salomao GL, McAllister A, Ternstrom S (2015) Natural voice use in patients with voice disorders and vocally healthy speakers based on 2 days voice accumulator information from a database. J Voice 29(646):e641–649
Hunter EJ (2012) Teacher response to ambulatory monitoring of voice. Logoped Phoniatr Vocol 37:133–135
Lombard E (1911) Signe de l'élévation de la voix. Annales des maladies de l'oreille, du larynx, du nez et du pharynx 37:101–119
Nusseck M, Richter B, Spahn C, Echternach M (2018) Analysing the vocal behaviour of teachers during classroom teaching using a portable voice accumulator. Logoped Phoniatr Vocol 43:1–10
Echternach M, Richter B, Traser L, Nusseck M (2013) Change of vocal capacity due to different vocal loading tests. Laryngorhinootologie 92:34–40
Hanschmann H, Gaipl C, Berger R (2011) Preliminary results of a computer-assisted vocal load test with 10-min test duration. Eur Arch Otorhinolaryngol 268:309–313
Hanschmann H, Wlodarz M, Berger R (2010) Standardisierte Stimmdiagnostik—Erste Erfahrungen mit einem computergestützen Stimmbelastungstest [Standardised voice diagnostics–first experiences with a computer-aided voice strain test]. Laryngorhinootologie 89:544–548
Vertigan AE, Kapela SM, Franke I, Gibson PG (2017) The effect of a vocal loading test on cough and phonation in patients with chronic cough. J Voice 31:763–772
Kelchner LN, Toner MM, Lee L (2006) Effects of prolonged loud reading on normal adolescent male voices. Lang Speech Hear Serv Sch 37:96–103
Vilkman E (2004) Occupational safety and health aspects of voice and speech professions. Folia Phoniatr Logop 56:220–253
Pabst F, Seiler R, Hacki T (1998) Zur Beurteilung der Sprechstimmleistungen nach Stimmbelastungstes mittels Stimmfeldmessung [Evaluation of speaking voice capacity using voice range profile after vocal loading tests]. In: Gross M (ed) Aktuelle phoniatrisch-pädaudiologische Aspekte, pp 73–75
Seidner W (2012) Messung der stimmlichen Belastbarkeit. [Evaluation of vocal loading capacity] In: Seidner W, Nawka T (eds) Handreichungen zur Stimmdiagnostik: Aus der Praxis für die Praxis, pp 91–105
Laukkanen AM, Jarvinen K, Artkoski M et al (2004) Changes in voice and subjective sensations during a 45-min vocal loading test in female subjects with vocal training. Folia Phoniatr Logop 56:335–346
Echternach M (2016) Die Messung der stimmlichen Belastung und Belastbarkeit. Sprache Stimme Gehör 40:188–191
Schneider B, Bigenzahn W (2007) Stimmbelastungstet zur Überprüfung der stimmlichen Belastungsfähigkeit [Vocal loading test for the evaluation of vocal loading capacity]. In: Schneider B, Bigenzahn W (eds) Stimmdiagnostik. Springer, Wien, pp 105–109
Niebudek-Bogusz E, Kotylo P, Politanski P, Sliwinska-Kowalska M (2008) Acoustic analysis with vocal loading test in occupational voice disorders: outcomes before and after voice therapy. Int J Occup Med Environ Health 21:301–308
Chang A, Karnell MP (2004) Perceived phonatory effort and phonation threshold pressure across a prolonged voice loading task: a study of vocal fatigue. J Voice 18:454–466
Enflo L, Sundberg J, McAllister A (2013) Collision and phonation threshold pressures before and after loud, prolonged vocalization in trained and untrained voices. J Voice 27:527–530
Jacobson BH, Johnson A, Grywalski C et al (1997) The Voice Handicap Index (VHI). Am J Speech Lang Pathol 6:66–70
Mann EA, McClean MD, Gurevich-Uvena J et al (1999) The effects of excessive vocalization on acoustic and videostroboscopic measures of vocal fold condition. J Voice 13:294–302
Laukkanen AM, Kankare E (2006) Vocal loading-related changes in male teachers' voices investigated before and after a working day. Folia Phoniatr Logop 58:229–239
Wuyts FL, De Bodt MS, Molenberghs G et al (2000) The dysphonia severity index: an objective measure of vocal quality based on a multiparameter approach. J Speech Lang Hear Res 43:796–809
Richter B, Nusseck M, Spahn C, Echternach M (2016) Effectiveness of a voice training program for student teachers on vocal health. J Voice 30:452–459
Kramer H, Perez Alvarez JC, Hacki T (1999) Stimmleistungscharakterisierende Kurventypen im Stimmbelastungstest [Vocal loading curve types characterizing vocal capacity]. In: Gross M (ed) Aktuelle phoniatrisch-pädaudiologische Aspekte, pp 75–79
Lohscheller J, Döllinger M, McWhorter AJ, Kunduk M (2008) Preliminary study on the quantitative analysis of vocal loading effects on vocal fold dynamics using phonovibrograms. Ann Otol Rhinol Laryngol 117:484–493
Döllinger M, Lohscheller J, McWhorter A, Kunduk M (2009) Variability of normal vocal fold dynamics for different vocal loading in one healthy subject investigated by phonovibrograms. J Voice 23:175–181
Döllinger M (2009) The next step in voice assessment: high-speed digital endoscopy and objective evaluation. Curr Bioinform 4:101–111
Lohscheller J, Eysholdt U (2008) Phonovibrogram visualization of entire vocal fold dynamics. Laryngoscope 118:753–758
Lohscheller J, Eysholdt U, Toy H, Döllinger M (2008) Phonovibrography: mapping high-speed movies of vocal fold vibrations into 2-D diagrams for visualizing and analyzing the underlying laryngeal dynamics. IEEE Trans Med Imaging 27:300–309
Howard DM (1995) Variation of electrolaryngographically derived closed quotient for trained and untrained adult female singers. J Voice 9:163–172
Titze IR (1994) Principles of voice production. Prentice Hall, New Jersey
Echternach M, Burk F, Koberlein M, Burdumy M, Dollinger M, Richter B (2017) The influence of vowels on vocal fold dynamics in the Tenor's Passaggio. J Voice 31:424–429
Yiu EM, Chan RM (2003) Effect of hydration and vocal rest on the vocal fatigue in amateur karaoke singers. J Voice 17(2):216–227
Echternach M, Döllinger M, Sundberg J, Traser L, Richter B (2013) Vocal fold vibrations at high soprano fundamental frequencies. J Acoust Soc Am 133:EL82–EL87
Acknowledgements
Open Access funding provided by Projekt DEAL. Part of the dataset is used for Mr. Huseynov`s MD thesis at the University of Freiburg. Matthias Echternach’s work is supported by Deutsche Forschungsgemeinschaft (DFG, Grant 409/1-2). The authors thank Patrick Schlegel, Erlangen University, for improving the Multi Signal Analyzis Software. The authors thank Helena Daffern, PhD, for native corrections.
Funding
DFG, Grant 409/1-2.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There are no financial interests, nor is there any conflict of interest for the authors to declare.
Ethical standards
The study was performed in agreement to the Hesiniki declaration standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Echternach, M., Huseynov, J., Döllinger, M. et al. The impact of a standardized vocal loading test on vocal fold oscillations. Eur Arch Otorhinolaryngol 277, 1699–1705 (2020). https://doi.org/10.1007/s00405-020-05791-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-020-05791-5