
Abstract
Purpose
Adenomyosis is a common disease of females during their reproductive age. As of today, histologic examination of the uterus after hysterectomy constitutes the gold standard for diagnosis. The aim of this study was to determine the validity of sonographic, hysteroscopic, and laparoscopic criteria for the diagnosis of the disease.
Methods
This study included data collected from 50 women in the reproductive age of 18–45 years, who underwent a laparoscopic hysterectomy in the gynecology department of the Saarland University Hospital in Homburg between 2017 and 2018. The patients with adenomyosis were compared with a healthy control group.
Results
We collected data of anamnesis, sonographic criteria, hysteroscopic criteria and laparoscopic criteria and compared it with the postoperative histological results. A total 25 patients were diagnosed with adenomyosis postoperatively. For each of these; at least three sonographic diagnostical criteria for adenomyosis were found compared with a maximum of two for the control group.
Conclusion
This study demonstrated an association between pre- and intraoperative signs of adenomyosis. In this way, it shows a high diagnostic accuracy of the sonographic examination as a pre-operative diagnostic method of the adenomyosis.
Similar content being viewed by others


Pre-operative ultrasonography is an accurate diagnostic method for adenomyosis. Intraoperatively the uteri of patients with adenomyosis present specific morphologic features. Combining preoperative with intraoperative findings can have important diagnostic implications for patients with adenomyosis. |
Introduction
Adenomyosis, the presence of endometrial glands and stroma in the myometrium, constitutes a benign entity presenting with dysmenorrhea, pelvic pain, abnormal uterine bleeding, and/or infertility [1, 2]. Of note, adenomyosis and endometriosis are considered two different entities with very much different etiopathologies and treatment strategies, as pointed in the latest guidelines for endometriosis by the European Society of Human Reproduction and Embryology (ESHRE) [3].
Even though a series of mechanisms have been proposed, the etiology of the disease remains enigmatic [4, 5]. Currently, the most accepted theory is that of a disrupted endomyometrial junction resulting in direct invasion of endometrial cells from the basalis layer into the myometrium because of continuous tissue injury signals [4, 5].
Estimating the exact prevalence of adenomyosis is linked with significant limitations [6, 7]. For example, assessing the prevalence at hysterectomy (the diagnostic gold standard) is prone to selection bias [7]. Hysterectomy is performed in patients with complaints, which means that asymptomatic patients are excluded from prevalence estimation [7]. According to a recent review by Upson and colleagues, reported estimates range from 8 to 60%, depending on histologic criteria used by each study [7]. Furthermore, estimating the prevalence of adenomyosis based on diagnosis at hysterectomy increases the mean age of patients diagnosed with the disease, leaving younger women out of the estimation [7].
Regarding treatment, there is controversy regarding the optimal therapy for adenomyosis [8]. An important pillar of treatment is medical treatment with analgesics as well as hormonal therapies being available [9]. These include gonadotropin releasing hormone antagonists (GnRHa), levonogestrel-releasing intrauterine devices (LNG-IUD), dienogest, or ulipristal acetate [9]. Surgical uterus-sparing concepts have also developed in recent years and are being propagated for the treatment of women with infertility [10]. Given the high burden of the disease on the patients and health systems as well as a correlation with deep infiltrating endometriosis, which might require even more extensive surgery (thus increased morbidity), early non-invasive diagnosis is of vital importance [11, 12].
An important part of non-invasive diagnosis is ultrasound [13]. Sonography is becoming a first-line method for diagnosing adenomyosis with comparable diagnostic accuracy as the golden standard [13, 14]. Recently, an international consortium of expert sonographers proposed the use of standardized examination system for the sonographic examination of patients with adenomyosis [15]. These criteria include a series of diagnostic signs as well as standardized examination for diagnosis adenomyosis [15].
What remains uncaptured is the correlation between pre-operative findings, intraoperative signs, and histologic diagnosis of adenomyosis. The aim of this case–control study is to investigate this correlation and compare the presence of known signs indicative of adenomyosis in patients with histologically proven adenomyosis versus healthy controls.
Materials and methods
Setting and participants
We conducted a case–control study of patients with adenomyosis undergoing hysterectomy between January 2017 and December 2018 at the University Hospital of Saarland in Homburg, Germany. Eligibility criteria included known patients being treated at our endometriosis clinic of reproductive age, histologic diagnosis of adenomyosis after hysterectomy, and absence of leiomyomas. Patients should have been operated on hysteroscopic and laparoscopic once before hysterectomy. Exclusion criteria included current ongoing medical treatment, ongoing pregnancy, or incomplete clinical data. Patient selection was conducted after screening of electronic health records of the hospital. Patient data were extracted into a predefined Excel file.
Clinical data
All patients completed a standardized clinical questionnaire, which included questions about dysmenorrhea, the pain severity in cases of dysmenorrhea classified using the visual analog scale (VAS) [16], dyspareunia, hypermenorrhea, dyschezia, dysuria (especially during or just before the period), hormone therapy, previous operations for endometriosis and pregnancy and parity.
Ultrasonographic features
All patients were preoperatively examined in a systematic way from experienced gynecologic sonographers using Arietta 65, Hitachi. Eight features of adenomyosis were obtained: an anterior–posterior wall asymmetry of the uterus (Fig. 1A, B) [13], an irregular/blurred junctional zone (Fig. 1C) [13], a question mark shape of the uterus (Fig. 1D) [17], a “Rainforest Phenomenon” (Fig. 1E) [17, 18], intramural lacunae (Fig. 1F) [17, 18], a heterogeneous echogenicity of the myometrium (Fig. 1G) [17, 18], a diffuse vascularisation of the myometrium (Fig. 1H) [17, 18], and an enlarged globular fundus uteri (Fig. 1I) [17, 18].

Adenomyosis-specific sonographic markers. A Asymmetric walls of uterus. B Asymmetric uterus walls. Marked for optimal visualization. C A blurred junctional zone of the endometrium and myometrium. D A question mark form of the uterus. E “Rainforest-Phenomen” of the uterus. F Intramural lacunae of the myometrium. G Heterogenic echogenicity of the myometrium. H Diffuse vascularisation of the myometrium. I Enlarged globular fundus uteri. All images were taken in our clinic
Intraoperative findings
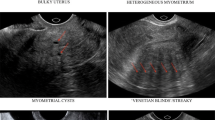
To demonstrate possible correlations between sonographic criteria and intraoperative hysteroscopic and laparoscopic findings in the presence of adenomyosis, the following hysteroscopic and laparoscopic criteria were examined for their presence. The four hysteroscopic features were the “Strawberry Sign” (Fig. 2A), lacunar formations of the endometrium (Fig. 2B), hypervascularisation, and cystic haemorrhagic lesions in the area of the endometrium (Fig. 2C) [19]. Apart from hysteroscopic, five laparoscopic features were obtained; enlargement of the corpus uteri > 9 cm, a spherical shape of the uterus (Fig. 2D), a soft, doughy uterine wall, a marbled serosa over the uterus (Fig. 2E), and brownish cysts on the uterine wall (Fig. 2F) [20]. Additionally, we extracted information on the results of the tubal patency test (with methylene blue) from previous operations (Fig. 2H) [18]. The presence of the “Blue sign”, namely the acquisition of blue color mostly in the posterior wall of the uterus as a result of the altered myometrium and/or disrupted junctional zone seen in adenomyosis, was also extracted (Fig. 2G) [18].

Hysteroscopic and laparoscopic criteria of endometriosis. A Strawberry sign in hysteroscopy. B Lacunar formation in the endometrium in hysteroscopy. C Hypervascularisation and cystic haemorrhagic lesions in the area of the endometrium in hysteroscopy. D Enlargement of the corpus uteri and a spherical shape of the uterus in laparoscopy. E A marbled serosa over the uterus in laparoscopy. F Brownish cysts on the uterine wall in laparoscopy. G The assessment of the tube permeability in laparoscopy. H The “Blue Sign” in laparoscopy. All images are taken in our clinic
For a better assessment of the endometrium, all operations in our department are carried out during the first half of the cycle. Endoscopic operations were conducted using conventional instruments described in the previous publications [21].
The patients with adenomyosis were compared with a control group of 25 age-matched patients. The patients in the control group were premenopausal women who had a hysterectomy for an indication other than adenomyosis or a myoma. These indications included cervical intraepithelial neoplasia, hysterectomy for gender dysphoria, and uterine prolapse. These patients were assessed for the same clinical, sonographical, and intraoperative criteria for adenomyosis as the endometriosis patients. The results between the groups were compared.
Statistical analysis
After consultation with the local Institute for Medical Statistics, we refrained from a statistical analysis with the determination of statistical significance because of the monocentric character of the work. Instead, a descriptive analysis was carried out. The data were analyzed using “Microsoft Excel” program. After complete data extraction, the absolute and relative frequencies of each criterion in the different groups were determined. In this way, the absolute and relative frequencies of the criteria in relation to the parameters could be evaluated. The results are presented in tables and graphics.
Results
A total of 25 patients with adenomyosis in the histological work-up after hysterectomy fulfilled the eligibility criteria and were enrolled in the study. Clinical characteristics are presented in Table 1. The median age of the patients was 30 years (Range: 18–45 years). Each of the 25 patients with a postoperative diagnosis of adenomyosis had previous surgery for endometriosis (hysteroscopy, laparoscopy with removal of endometriosis lesions, and chromopertubation).
Sonographic features
The minimum sonographic portio-fundus (measured intraoperatively) distance was 7 cm and the maximum 12 cm. The median sonographic portio-fundus distance in adenomyosis was 9.5 cm. In the comparison group, the portio-fundus distance varied between 4 cm (minimum) and 8.5 cm (maximum). The median portio-fundus distance in the patients without adenomyosis was 6 cm.
The uterine width varied between 4 cm (minimum) and 7 cm (maximum) in adenomyosis. In the patients of the comparison group, the median uterine width was 3.5 cm. Twenty of the 25 patients with adenomyosis (80%) had diffuse vascularization of the myometrium on sonography, compared to only 7 of 25 patients (28%) in the comparison group. An anterior–posterior wall asymmetry of > 1/3 was present in 80% of the adenomyosis patients (20 of 25 patients). In the comparison group, only 5 out of 25 patients (20%) had anterior–posterior uterine asymmetry. Intramural lacunae were present in 15 of 25 (60%) patients. In women without adenomyosis, intramural lacunae were found in 5 of 25 cases (20%).
A blurred junctional zone was present in more than half of the patients with adenomyosis in the region of the myometrium (in 13 of 25 patients or 52%). In the comparison group, 3 out of 15 women (12%) were affected. A question mark form of the uterus was present in only about 1/3 of the patients (8 of 25 patients) with adenomyosis. In the control group, 2 out of 25 patients (8%) had a question mark form. An enlarged, spherical fundus was also detected in about 1/3 (8 out of 25 patients) of the adenomyosis patients, but only in 3 out of 25 patients (12%) of the comparison group.
The rainforest sign was detected preoperatively in 7 of 25 adenomyosis patients (28%) and in 2 patients (7%) without adenomyosis. A heterogeneous echogenicity of the myometrium was seen in 8 of 25 (32%) patients with adenomyosis and in 4 of 25 patients (16%) without adenomyosis. In all patients with histologically confirmed adenomyosis, at least three ultrasound criteria of adenomyosis could be detected, while in the control group, the maximum number of sonographic features demonstrated per patient was two.
Hysteroscopic features
The strawberry sign was detected in 15 of the 25 patients with adenomyosis (60%) during hysteroscopy. Thirteen of 25 patients (52%) had hypervascularisation. Lacunae in the endometrium and cystic, haemorrhagic lesions of the endometrium were detected in 7 of 25 patients (28%). All patients with confirmed adenomyosis had at least two hysteroscopic features.
Laparoscopic features
The minimum intraoperative probe length for adenomyosis was 7 cm. Fifteen patients had a probe length > 9 cm. In the comparison group, 16 of 25 patients (64%) had an intraoperative uterine probe length between 6 and 7 cm. The uterus was spherical in 22 of 25 (88%) adenomyosis patients. In the comparison group, three patients (12%) had a spherical shape of the uterus.
Thirteen out of 25 (52%) of the patients with adenomyosis had a doughy uterine wall intraoperatively. Of the patients in the comparison group, only 2 out of 25 patients (8%) had a doughy uterine wall.
A total of 7 out of 15 patients (28%) with adenomyosis had a marbled uterine surface intraoperatively. In contrast, 2 out of 25 patients (8%) without adenomyosis had a marbled uterine surface.
Only 3 out of 25 patients (12%) with adenomyosis had cysts on the uterine wall. Two out of 25 women without adenomyosis (8%) had uterine cysts.
Tubal patency test
Of the 25 patients with adenomyosis, ten had a blue sign intraoperatively. In terms of tubal permeability, in seven (28%) both were patent, in fifteen only one was patent, and in three there was no tubal patency (Table 1).
All adenomyosis patients had at least two intraoperative features. Patients without adenomyosis had a maximum of one laparoscopic finding typical of adenomyosis.
Discussion
This monocentric case–control study has been able to clarify the significance of clinical, sonographic, and operative criteria in the diagnosis of adenomyosis. Patients with adenomyosis present with at least three sonographic signs compared two in healthy controls. Regarding intraoperative signs, these were more common in patients diagnosed with adenomyosis compared with controls.
The significance of sonographic signs in adenomyosis has been studied by various working groups. Nevertheless, no superiority has been demonstrated for one specific sign. For example, Sun and colleagues demonstrated that subendometrial echogenic striae (equivalent to the rainforest sign) had the best sensitivity for diagnosis adenomyosis among various other sonographic markers [22]. A recent meta-analysis by Anders et al. demonstrated that myometrial heterogeneity was associated with highest sensitivity and a globular uterus with the highest specificity [17]. Of note, both parameters were increased when the question mark sign was incorporated in the analysis [17]. In a cohort of young women solely with adenomyosis, the asymmetrical myometrial wall morphology was the most common sonographic sign [23]. In our study, the validity of the sonographic parameters is underlined by the fact that all sonographic parameters were detected significantly less frequently in women of the comparison group.
An important advantage of our study was the completeness of the data as well as the systematic evaluation of patient history, ultrasonographic findings, and intraoperative findings. Structured reports and their role in the diagnosis of adenomyosis have been studied by Ribeiro da Silva et al. [24]. According to the researchers, structured ultrasound reports (as the ones used in our studies) are more effective in diagnosing adenomyosis compared with non-structured ones [24].
All patients in our study underwent standardized procedure by expert sonographers and laparoscopists. Furthermore, our study investigated signs obtained during hysteroscopy, laparoscopy, and chromopertubation (e.g., the blue sign), and correlated them with pre-operative findings and definitive histology.
Despite its strengths, the present study has methodological limitations. The strongest limiting factor is the small number of patients included in the study. Small number statistics and inference can be prone to limitations, as a few patients can cause a considerable effects in the data analysis as pointed out by Button and colleagues [25]. Therefore, in consultation with the local Institute for Medical Statistics, we did not determine the statistical significance and limited ourselves to a descriptive analysis. Furthermore, the data stem exclusively from one center, which might have implication for extrapolation. Finally, the retrospective nature of the study might pose limitations in terms of generalization in other cohorts.
In addition to sonography, magnetic resonance imaging can also be used in the non-invasive diagnosis of adenomyosis [26, 27]. Studies have demonstrated sensitivity of almost 90% making MRI comparable and sometimes more reliable than ultrasound (i.e., patients with increased body mass index) [26, 27]. Its comparability with ultrasound has already been studied [28]. The advantages of MRI are the low inter-examiner variability, the high sensitivity and specificity, and the almost unsurpassed soft-tissue contrast [26, 27]. However, due to its lower availability, longer examination time, and higher equipment and maintenance costs, MRI is far less suitable for widespread use than sonography under everyday conditions, especially in the outpatient setting [26, 27]. Future prospective studies incorporating MRI findings as well as ultrasonographic signs with intraoperative and histologic criteria could be more insightful.
Conclusions
This study shows a high diagnostic accuracy of the sonographic examination as a pre-operative diagnostic method of the adenomyosis. Furthermore, it demonstrates an important association between intraoperative signs (both hysteroscopic and laparoscopic), histologic diagnosis, and pre-operative assessment. Taken together, these signs can play an important role in coining the diagnosis of adenomyosis.
Data availability
The dataset used and analyzed for th study is available from the corresponding author on reasonable request.
References
Struble J, Reid S, Bedaiwy MA (2016) Adenomyosis: a clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol 23:164–185. https://doi.org/10.1016/j.jmig.2015.09.018
International working group of AAGL, ESGE, ESHRE and WES, Tomassetti C, Johnson NP et al (2021) An international terminology for endometriosis, 2021. J Minim Invasive Gynecol 28:1849–1859. https://doi.org/10.1016/j.jmig.2021.08.032
The members of the Endometriosis Guideline Core Group, Becker CM, Bokor A et al (2022) ESHRE guideline: endometriosis†. Human Reprod Open 2022:hoac009. https://doi.org/10.1093/hropen/hoac009
Khan KN, Fujishita A, Mori T (2022) Pathogenesis of human adenomyosis: current understanding and its association with infertility. J Clin Med 11:4057. https://doi.org/10.3390/jcm11144057
Bulun SE, Yildiz S, Adli M, Wei J-J (2021) Adenomyosis pathogenesis: insights from next-generation sequencing. Hum Reprod Update 27:1086–1097. https://doi.org/10.1093/humupd/dmab017
Taran FA, Stewart EA, Brucker S (2013) Adenomyosis: epidemiology, risk factors, clinical phenotype and surgical and interventional alternatives to hysterectomy. Geburtshilfe Frauenheilkd 73:924–931. https://doi.org/10.1055/s-0033-1350840
Upson K, Missmer SA (2020) Epidemiology of adenomyosis. Semin Reprod Med 38:89–107. https://doi.org/10.1055/s-0040-1718920
Sharara FI, Kheil MH, Feki A et al (2021) Current and prospective treatment of adenomyosis. J Clin Med 10:3410. https://doi.org/10.3390/jcm10153410
Vannuccini S, Luisi S, Tosti C et al (2018) Role of medical therapy in the management of uterine adenomyosis. Fertil Steril 109:398–405. https://doi.org/10.1016/j.fertnstert.2018.01.013
Osada H (2018) Uterine adenomyosis and adenomyoma: the surgical approach. Fertil Steril 109:406–417. https://doi.org/10.1016/j.fertnstert.2018.01.032
Lazzeri L, Di Giovanni A, Exacoustos C et al (2014) Preoperative and postoperative clinical and transvaginal ultrasound findings of adenomyosis in patients with deep infiltrating endometriosis. Reprod Sci 21:1027–1033. https://doi.org/10.1177/1933719114522520
Yu O, Schulze-Rath R, Grafton J et al (2020) Adenomyosis incidence, prevalence and treatment: United States population-based study 2006–2015. Am J Obstet Gynecol 223:94.e1-94.e10. https://doi.org/10.1016/j.ajog.2020.01.016
Van den Bosch T, de Bruijn AM, de Leeuw RA et al (2019) Sonographic classification and reporting system for diagnosing adenomyosis. Ultrasound Obstet Gynecol 53:576–582. https://doi.org/10.1002/uog.19096
Munro MG (2020) Classification and reporting systems for adenomyosis. J Minim Invasive Gynecol 27:296–308. https://doi.org/10.1016/j.jmig.2019.11.013
Harmsen MJ, Van den Bosch T, de Leeuw RA et al (2022) Consensus on revised definitions of morphological uterus sonographic assessment (MUSA) features of adenomyosis: results of modified Delphi procedure. Ultrasound Obstet Gynecol 60:118–131. https://doi.org/10.1002/uog.24786
Aitken RC (1969) Measurement of feelings using visual analogue scales. Proc R Soc Med 62:989–993
Andres MP, Borrelli GM, Ribeiro J et al (2018) Transvaginal ultrasound for the diagnosis of adenomyosis: systematic review and meta-analysis. J Minim Invasive Gynecol 25:257–264. https://doi.org/10.1016/j.jmig.2017.08.653
Graziano A, Lo Monte G, Piva I et al (2015) Diagnostic findings in adenomyosis: a pictorial review on the major concerns. Eur Rev Med Pharmacol Sci 19:1146–1154
Gordts S, Grimbizis G, Campo R (2018) Symptoms and classification of uterine adenomyosis, including the place of hysteroscopy in diagnosis. Fertil Steril 109:380-388.e1. https://doi.org/10.1016/j.fertnstert.2018.01.006
Guerriero S, Saba L, Pascual MA et al (2018) Transvaginal ultrasound vs magnetic resonance imaging for diagnosing deep infiltrating endometriosis: systematic review and meta-analysis. Ultrasound Obstet Gynecol 51:586–595. https://doi.org/10.1002/uog.18961
Stotz L, Joukhadar R, Hamza A et al (2018) Instrument usage in laparoscopic gynecologic surgery: a prospective clinical trial. Arch Gynecol Obstet 298:773–779. https://doi.org/10.1007/s00404-018-4867-5
Sun Y-L, Wang C-B, Lee C-Y et al (2010) Transvaginal sonographic criteria for the diagnosis of adenomyosis based on histopathologic correlation. Taiwan J Obstet Gynecol 49:40–44. https://doi.org/10.1016/S1028-4559(10)60007-1
Pinzauti S, Lazzeri L, Tosti C et al (2015) Transvaginal sonographic features of diffuse adenomyosis in 18–30-year-old nulligravid women without endometriosis: association with symptoms. Ultrasound Obstet Gynecol 46:730–736. https://doi.org/10.1002/uog.14834
da Silva JR, Andres MP, Leite APK et al (2021) Comparison of sensitivity and specificity of structured and narrative reports of transvaginal ultrasonogaphy for adenomyosis. J Minim Invasive Gynecol 28:1216–1224. https://doi.org/10.1016/j.jmig.2020.11.001
Button KS, Ioannidis JPA, Mokrysz C et al (2013) Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci 14:365–376. https://doi.org/10.1038/nrn3475
Tellum T, Matic GV, Dormagen JB et al (2019) Diagnosing adenomyosis with MRI: a prospective study revisiting the junctional zone thickness cutoff of 12 mm as a diagnostic marker. Eur Radiol 29:6971–6981. https://doi.org/10.1007/s00330-019-06308-3
Celli V, Dolciami M, Ninkova R et al (2022) MRI and adenomyosis: what can radiologists evaluate? Int J Environ Res Public Health 19:5840. https://doi.org/10.3390/ijerph19105840
Karamanidis D, Nicolaou P, Chrysafis I et al (2018) OC01: transvaginal ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis. Ultrasound Obstet Gynecol 52:555. https://doi.org/10.1002/uog.19201
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Conceptualization: BHH and MS; methodology: R-MS; software, LP; validation: E-FS; formal analysis: GO; investigation: BHH; resources: R-MS; data curation: MK; writing—original draft preparation: BHH; writing—review and editing: MS; visualization: LP; supervision: GO; project administration: BHH. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki, and approved by the University of Saarland Hospital Ethics Committee (59/2017).
Informed consent
Informed consent was obtained from all subjects involved in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Haj Hamoud, B., Kasoha, M., Sillem, M. et al. Sonographic features of adenomyosis correlated with clinical symptoms and intraoperative findings: a case–control study. Arch Gynecol Obstet 307, 1883–1889 (2023). https://doi.org/10.1007/s00404-022-06852-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-022-06852-2