
Abstract
Background/aim
According to recent studies up to 80 % of patients would like to receive more information about how cancer treatments can affect their sexual functioning. Moreover, 75 % of them would not feel comfortable being the first to bring up the subject. Our Gynaecological Advice Clinic was established in 2006 at the Christie Hospital and offers support to cancer patients who face sexuality issues. A previous evaluation established that the service sees approximately, 200 patients per year. The aims of this study are to evaluate the service by collecting data relating to levels of attendance, type and amount of clinical activity and to explore further patients’ experiences and management.
Methods
This is a retrospective study which was carried out in 2012–2013. Different models are used to evaluate our patients including history taking integrated therapy model, consultations to understand the normal anatomy and physiology with the use of diagrams and photographs, psycho-education and the international classification “Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition” (DSMV). The treatment options advised include medications such as hormone replacement treatment, testosterone, antidepressant, local oestrogen, tibolone, aqueous cream, lubrication to introitus, diprobase, dermal cream and advice for massage to areas of discomfort. Moreover, the use of vaginal dilators, the role of pelvic floor exercises, vulval care and self examination are explained. The team works closely with the psycho-oncology department. The most frequently discussed topics that were covered during the consultation are analysed.
Results
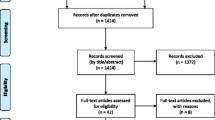
41 outpatient clinics were held between 2012 and 2013. 194 patients attended those clinics during the study period. Single and not group therapy was offered to all the participants. 216 patients were offered appointments while 194 patients actually attended (90 %). Patients’ age ranged from 24 to 91 years with a mean age of 59 years. 45 % had endometrial and 32 % cervical cancer, 18 % vulval cancer, 4 % ovarian cancer. 74 % attended on their own while 18 % with their partners and 8 % with another family member or friend. 98 % of the patients had confidence/trust in the healthcare professional. 95 % felt involved with treatment decisions. 82 % reported completely understanding information about side-effects. 16 % were unaware of who to contact once they had completed treatment. 8 % were attending for on-going help with psycho-sexual concerns following completion of treatment.
Conclusion
The clinic was positively evaluated by patients, they had a high level of trust in the nurses running the service and they found it beneficial. Consultations were generally lasting 20–30 min and most patients reported this was an appropriate length. It once again highlights that although the service was set-up to address psycho-sexual concerns, in reality it dealt with a variety of other patient concerns. Due to the success of the clinic, the service has expanded and we are now supporting patients from other tumour groups such as colorectal, urology and plastic surgery.
Similar content being viewed by others


References
Smith PH, Ballantyne B (1968) The neuroanatomical basis of denervation of the urinary bladder following major pelvic surgery. Br J Surg 55:929–933
Parys BT, Haylen B, Hutton JL, Parsons KF (1989) The effect of simple hysterectomy on vesicourethral function. Br J Urol 64:594–599
Ayhan A, Tuncer ZS, Yarali H (1991) Complications of radical hysterectomy in women with early stage cervical cancer: clinical analysis of 270 cases. Eur J Surg Oncol 17:492–494
Ralph G, Tamussino K, Lichtenegger W (1990) Urological complications after radical hysterectomy with or without radiotherapy for cervical cancer. Arch Gynecol Obstet 248:61–65
Greimel E, Thiel I, Peintinger F, Cegnar I, Pongratz E (2002) Prospective assessment of quality of life of female cancer patients. Gynecol Oncol 85:140–147
Lutgendorf SK, Anderson B, Ullrich P et al (2002) Quality of life and mood in women with gynecologic cancer: a one year prospective study. Cancer 94:131–140
Schover LR, Fife M, Gershenson DM (1989) Sexual dysfunction and treatment for early stage cervical cancer. Cancer 63:204–212
Wiggins D, Wood R, Granai C, Dizon D (2007) Sex, intimacy, and the gynecologic oncologist: survey results of the New England Association of Gynecologic Oncologists (NEAGO). J Psychosoc Oncol 25(4):61–70
Pountney D (2005) The loss of femininity, sexual desire and body image that women can suffer after radiotherapy or gynaecological surgery is very real. Cancer Nurs Pract (4):9
Jefferies H, Hoy S, McCahill R, Crichton A (2007) Guidelines on vaginal dilator use after pelvic radiotherapy. Nurs Times 103(30):28–29
Jeffries SA, Robinson JW, Craighead PS, Keats MR (2006) An effective group psychoeducational intervention for improving compliance with vaginal dilation; a randomised trial. Int J Radiat Biol Phys 6(4):404–411
Brotto L, Erskine Y, Carey M, Ehlen T, Finlayson S, Heywood M, Kwon J, McAlpine J, Stuart G, Thomson S, Miller D (2012) A brief mindfulness-based cognitive behavioral intervention improves sexual functioning versus wait-list control in women treated for gynecologic cancer. Gynecol Oncol 125(2):320–325
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Iavazzo, C., Johnson, K., Savage, H. et al. Sexuality issues in gynaecological oncology patients: post treatment symptoms and therapeutic options. Arch Gynecol Obstet 291, 653–656 (2015). https://doi.org/10.1007/s00404-014-3491-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-014-3491-2