
Abstract
Nail psoriasis is a chronic, inflammatory condition which is difficult to treat, linked with greater psoriasis severity, and may be associated with anxiety and significant functional impairment of the quality of life. The 1064 nm Nd: YAG laser was reported to yield satisfactory results in the treatment of nail psoriasis.
The aim of the study was to assess the clinical and ultrasonographic efficacy of long-pulsed 1064 nm Nd: YAG laser in the treatment of fingernail psoriasis and compare its effect to control fingernails.
This intra-patient randomized controlled trial analyzed 86 fingernails collected from 13 patients suffering from cutaneous and nail psoriasis. The nails were randomized into two groups. Group A was treated with Nd: YAG laser once monthly for three sessions while group B served as control. Assessment took place at baseline, 1 and 3 months after the last treatment session. For scoring, the 32-points target NAPSI scoring systems was used. Additionally, two blinded dermatologists’ score of improvement, patients’ pain assessment by visual analogue score and ultrasonographic assessment were all performed.
At the end of follow up, the medians of tNAPSI score, plate definition, matrix thickness, bed thickness and bed vascularity decreased significantly in the Nd: YAG laser treated group in comparison to baseline (p = 0.001, 0.006, 0.039, < 0.001 and 0.010, respectively). While, there was a non-significant reduction in median tNAPSI score in the control group at last follow up, however, ultrasonography recorded a significant reduction in the medians of plate definition, bed thickness and vascularity (p = 0.002, 0.011 and 0.033, respectively) from the baseline. Comparison of the Nd: YAG laser and the control groups showed no significant difference from baseline regarding the medians of tNAPSI, tNAPSI percentile improvement, pits count, blinded evaluation of photographs and ultrasonographic assessments.
In conclusion, Nd: YAG laser showed clinical and ultrasonographic improvement in fingernail psoriasis. Ultrasonography is a useful noninvasive tool in diagnosing and monitoring the clinical and even the subclinical changes in nail psoriasis. Nail psoriasis although difficult to treat, may show spontaneous improvement.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Nail psoriasis (NP) is a chronic, difficult to treat clinical presentation of psoriasis, associated with greater severity of the disease, characterized by a higher risk and earlier onset of psoriatic arthritis. Accordingly, it can be painful, and may be associated with anxiety and depression with significant functional impairment and reduction of the quality of life [1].
The prevalence of NP varies widely and prevalence studies are rare. Augustin et al. (2010) reported 40.9% of 3531 German patients with psoriasis during the years 2005 and 2007 in a cross-sectional study complained of NP, Armesto et al. (2011) undertook a prospective case-control study on 661 Spanish patients with psoriasis between 2007 and 2009 and reported that 47.4% of them had NP and, El-Komy et al. (2020) conducted a retrospective single-center study on 2534 Egyptian patients with psoriasis during the period from 2015 to 2018 and found that nail involvement was present among 524 (20.7%) of the patients [2,3,4].
Treatment of NP is challenging as the clinical improvement takes time to be observed and treatment is often met with poor compliance [5]. Therapies include patient’s education, topical, intra-lesional and systemic treatments, including biological therapies. Therapies are selected according to the disease severity, presence of comorbidities, and the impact of psoriatic nail dystrophy on the patient’s quality of life due to impaired function, pain, and aesthetics [6].
Laser modalities gained much attention in the treatment of NP; due to their penetrability into nail bed and/or nail matrix [7]. The 595 nm pulsed dye laser results showed significant improvement in treatment of NP, but causes some pain and leaves transient petechiae, hyperpigmentation and purpura [8]. Also, the 1064 nm neodymium doped: Yttrium Aluminum Garnet (Nd: YAG) laser was used in the treatment of NP, based on selective photo-thermolysis of hemoglobin mainly, to target the dermal vasculature of the nail bed with satisfactory results [9,10,11].
High-frequency ultrasound (US) with power Doppler (PD) assessment provides details of nails’ soft tissue structures and microvasculature. Thickened nail bed and matrix, alteration of nail plate definition and nail bed vascularization are the major US manifestation of nail psoriasis [12].
The aim of this study was to assess clinically and by ultrasonography the efficacy of Nd: YAG laser in the treatment of fingernail psoriasis and to compare its effect with control fingernails.
Patients and methods
Subjects
This randomized controlled study included 13 psoriasis vulgaris patients with evidence of nail psoriasis affecting at least six fingernails, recruited from Kasr Al-Aini Psoriasis Unit (KAPU), Cairo University and the dermatology clinic of the National Research Center (NRC), Egypt. All patients received an explanation of the steps of the study and signed an informed consent to participate in the study. The study was approved by the ethical committee of the National Institute of Laser Enhanced Sciences (NILES), Giza, Egypt with reference number “NILES-EC-CU 23/12/27”.
Patients were excluded if they received any systemic therapies for psoriasis in the last 6 months or any topical treatments for the last two weeks. Other exclusion criteria included patients with any other chronic illnesses and patients with proven onychomycosis.
For all included recruits, each fingernail was dealt with as a different case to a total of 86 fingernails. The card randomization procedure was used to distribute the affected fingernails to receive either long-pulsed Nd: YAG 1064 nm laser treatment or serve as control. Accordingly, 43 fingernails were included in group A to receive long-pulsed Nd: YAG 1064 nm laser treatment and 43 fingernails were included in group B to serve as control (Fig. 1).

Patients flow chart
Long-pulsed 1064 nm nd: YAG Laser
Long-pulsed Nd: YAG 1064 nm laser was applied using the (Cynosure®, INC, 5 Carlisle Road, Westford, MA 01886, USA). Patients received 3 sessions with 1-month intervals, with 2 passes of energy 20 Joules/cm2, pulse duration 10ms and spot size 5 mm, together with continuous cold air cooling.
Assessment methods
Clinical assessment
Assessments were done at the baseline, 1 month from last treatment session (EOS) and 2 months later at the last follow up (FU).
For clinical scoring of nail psoriasis, we used the 32-points target NAPSI (tNAPSI) scoring system where nails were examined for pitting, leukonychia, lunular red spots, crumbling, onycholysis, subungual hyperkeratosis, salmon patches and splinter hemorrhages [13]. Nail pits were counted and analyzed separately at every evaluation point.
Assessment included photography using a digital camera (Canon DS126291, CANON INC. Taiwan) and a dermoscope (Dermlite DL4, USA) to be evaluated by two blinded dermatologists experienced in psoriasis management at FU according to the physician’s global assessment of fingernail psoriasis score that ranged from 0 to 4 corresponding to clear, minimal, mild, moderate and severe [14].
Ultrasonographic assessment
A musculoskeletal ultrasound evaluation was carried out at the baseline and FU using a GE LOGIQ P6 device (Model 183995SUO, India) in conjunction with a high-frequency broadband linear array transducer (10-13 MHz). The settings for Doppler were a 500 Hz pulse repetition frequency, with color gain optimized for optimal sensitivity while minimizing excessive color noise. The patients were seated with their forearms, hands, and fingers in a neutral and relaxed posture on a table, and their fingernails were scanned longitudinally. To ensure an adequate acoustic interface and prevent compression of the structures, a thick gel layer was applied.
The severity of psoriatic nail changes was assessed using the Wortsman’s classification (0–4), which includes Grade 0 (normal nail plate consisting of two parallel hyperechoic bilaminar bands together with a virtual anechoic space between them), Grade I (focal hyperechoic involvement of the ventral nail plate without involvement of the dorsal nail plate), Grade II (continuous loss of the borders of the ventral nail plate), Grade III (wavy plates without blurring of both plates), and Grade IV (loss of definition of both nail plates) [15].
The thickness of the hypoechoic nail bed was measured as the maximum distance between the ventral plate of the nail and the edge of the phalangeal bone, while the thickness of the isoechoic area of the nail matrix was measured at the proximal end of the nail bed.
The vascularity of the nail bed was assessed using the power Doppler (PD) technique on a scale of 0 to 3, with 0 indicating no PD signal (normal), Grade I indicating a signal present in less than 25% of the examined area, Grade II indicating a signal present on 25% but less than 50% of the examined area, and Grade III indicating a signal present on 50% or more of the examined area [16].
Patients’ self-assessment
Patients were asked to report the degree of pain they felt during the first session for Nd: YAG laser through the pain visual assessment score (0–10) where “0” =no pain, “1–3” =mild pain, “4–6” =moderate to severe, “7–9” =very severe and “10” =worst pain possible [17].
Statistical analysis
Sample size: Using the Power Analysis and Sample Size (PASS) 11th release [18], a sample size of 21 nails in each group was calculated to have at least an 80% power to detect the differences at α = 0.050 between the Nd: YAG laser and control groups with total score mean ± SD at FU of 16.0 ± 5.8 and 22.85 ± 9.0, among Nd: YAG laser and placebo sides respectively [11]. We increased the sample for possible attrition up to 40 nails in each of the two studied groups.
Data were coded and entered using the Statistical Package for the Social Sciences (SPSS) version 28, 2021 (IBM Corp., Armonk, NY, USA). Data was summarized using mean, standard deviation, median, minimum and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. For comparison of serial measurements within each patient the non-parametric Wilcoxon signed rank test was used, comparisons between quantitative variables were done using the non-parametric Mann-Whitney test [19]. For comparing categorical data, Chi square (χ2) test was performed. Exact test was used instead when the expected frequency is less than 5 [20]. Testing for inter-rater and intra-rater reliability was done using the Intra Class Coefficient (ICC) and Cronbach’s alpha reliability coefficient with their 95% confidence interval (95%CI) [21]. P-values less than 0.05 were considered as statistically significant.
Results
Thirteen patients (86 fingernails), seven males and six females; completed the study and were analyzed. Patients ages ranged from 18 to 63 years with a median of 31 years, the duration of skin psoriasis ranged from 1 to 35 years with a median of 7 years and the duration of nail psoriasis ranged from 4 months-14 years with a median of 1.5 years. Six patients were cigarette smokers. Three patients had a family history of psoriasis. Urban residents were nine and four were rural residents. Twelve of the thirteen patients (92.3%) were manual workers.
Changes in target NAPSI and pitting
At baseline, we did not detect any significant differences between the studied groups regarding medians of tNAPSI scores and counted numbers of pits. Comparison between Nd: YAG laser and control groups at the end of FU did not show any statistically significant differences regarding the medians of tNAPSI score or pits count, and this was the case with both blinded dermatologists and ultrasonographic assessments as well.
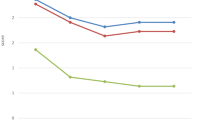
However, when groups were analyzed separately, there was a statistically significant difference in tNAPSI score between baseline and FU in group A (p = 0.001), while in group B this was non-significant (p = 0.054). The median percentage of improvement of tNAPSI score at FU in group A and B were 33.33% and 12.50%, respectively (Table 1; Figs. 2, 3 and 4).

Changes in median tNAPSI scores over time among studied groups

Changes in median pits count over time among studied groups

Clinical assessment of laser-treated and control nails of one patient at baseline and follow up
Also, blinded dermatologists’ photographic assessment of clinical as well as dermoscopic photos showed statistically significant improvement at FU in group A when analyzed separately, while this was not the case in the control group except for dermoscopic evaluation of the 2nd observer (Figs. 5 and 6).

Physicians’ global assessment by first blinded dermatologist at FU

Physicians’ global assessment by second blinded dermatologist at FU
Changes in ultrasonography
Ultrasonographic assessment of the Nd: YAG and control groups detected a statistically significant improvement in the median nail plate definition grade (p = 0.006 and 0.002, respectively) at end of FU period. Median nail matrix thickness showed significant reduction in the Nd: YAG treated group (p = 0.039) but not in the control group. Median nail bed thickness was reduced significantly in both Nd: YAG and control groups (p < 0.001, 0.011, respectively) and bed vascularity grade also showed significant improvement in both groups (p = 0.010, 0.033, respectively) (Table 2; Figs. 7, 8 and 9).

Ultrasonographic assessment at baseline and FU of nail plate definition grades (0–4) and nail bed vascularity grades (0–3)

Ultrasonographic assessment at baseline and FU of nail matrix and bed thickness (um)

Ultrasonographic assessment of laser-treated and control nails of another patient at baseline and follow up
The median degree of pain assessed through the pain visual assessment score (from 0 to 10) after the first session with the long-pulsed Nd: YAG laser was 2 (0–4).
Discussion
Treatment of nail psoriasis include topical, intra-lesional and systemic therapies selected according to the disease severity, its impact on the patient’s quality of life and comorbidities [5]. The penetrability of topical agents into the nail bed and/or matrix is essential to achieve therapeutic effect [6]. Nd: YAG laser, based on selective photo-thermolysis of hemoglobin, targets the dermal vasculature of the nail bed; the site of new changes occurring in psoriatic nail lesions [9,10,11]. In the current work treatment of NP with Nd: YAG laser was associated with significant improvements in tNAPSI, PGA and US measurements of matrix thickness in comparison to untreated nails with no adverse events reported in any of our patients.
The improvement of NP with Nd: YAG treatments we observed as well as previous investigators [9,10,11, 22] can be attributed to its ability to penetrate down to 5–6 mm in the tissue thus reaching the nail bed vascularity deep enough to target the abnormally increased vasculature in nail psoriasis by selective photo-thermolysis of hemoglobin [23, 24]. In addition, Nd: YAG laser reduces T cytotoxic cells in the epidermis, and T helper cells and CD3 + lymphocytes in the dermis, which in turn normalizes the epidermal proliferation and improve the clinical signs of psoriasis [10].
It is worth mentioning that Elwan et al. (2021) did not find significant improvements with Nd: YAG laser Vs controls in a left to right sided comparison of NP treatment after 6 month. Unlike the current study, the latter authors included toenail psoriasis, used NAPSI score and applied one pass with spot size 2.5 mm with laser energy of 110 J/cm2 to 130 J/cm2. They assumed that this non-significance was because they treated both finger-and toenails and that toenails may be more resistant than fingernails.[25, 26]
In the current study, we observed a non-significant spontaneous improvement in our “untreated” control group as regards tNAPSI score and this was also observed in the blinded physicians’ PGA score. Surprisingly, this non-significant clinical improvement was associated with significant ultrasonographic changes suggestive of a tendency towards normalization of nail plate definition, nail bed thickness and vascularity. Such observations are not unusual, as the course of NP is unpredictable and it may improve spontaneously or show unexpected remissions and exacerbations.[25,26,27,28,29] These improvements we report for the control group may also be attributed to the small sample size, or the systemic effect of locally targeted laser and thermal energies. Anders et al. (2015) and Khalkhal et al. (2020) described that laser irradiation can alter cellular metabolism and cellular functions in the body. They reported that local photo-biomodulation can produce systemic effects and that local irradiation produces distant effects. In a study performed on rats, the application of laser on a standardized skin wound had systemic effects on the wounds located distally from the point of laser application.[30,31,32]
Limitations
The limitations in the present study were the relatively small sample. Also, the fact that 92.3% were manual workers and housewives using unprotected bare hands may have hindered the therapeutic effects desired from treatment.
Conclusion
In conclusion, Nd: YAG laser can be considered safe, efficacious, local method of treating nail psoriasis. Ultrasonography is a useful noninvasive diagnostic and follow up tool that helps in detection of even subclinical changes. Our results also confirm that, nail psoriasis although a treatment challenge; may sometimes improves spontaneously.
Recommendation
Further larger scale studies for extended time periods are needed to verify our results and investigate the usefulness of US monitoring of nail changes in the treatment of NP.
Data availability
No datasets were generated or analysed during the current study.
References
Canal-García E, Bosch-Amate X, Belinchón I, Puig L (2022) [Translated article] nail psoriasis. Actas dermo-sifiliograficas 113(5):T481–T490
Augustin M, Reich K, Blome C, Schäfer I, Laass A, Radtke MA (2010) Nail psoriasis in Germany: epidemiology and burden of disease. Br J Dermatol 163(3):580–585
Armesto S, Esteve A, Coto-Segura P, Drake M, Galache C, Martínez-Borra J, Santos-Juanesc J (2011) Nail psoriasis in individuals with psoriasis vulgaris: a study of 661 patients. Actas Dermo-Sifiliográficas (English Edition) 102(5):365–372
El-Komy MH, Mashaly H, Sayed KS, Hafez V, El-Mesidy MS, Said ER, Amer MA, AlOrbani AM, Saadi DG, El-Kalioby M, Eid RO (2020) Clinical and epidemiologic features of psoriasis patients in an Egyptian medical center. JAAD Int 1(2):81–90
Kassir M, Kircik L, Weinberg J, Fatima F, Yamauchi P, Lotti T, Wollina U, Grabbe S, Goldust M (2022) Treatment of Nail Psoriasis. J Drugs Dermatology: JDD 21(2):146–150
Rich P, Manhart R (2017) Nail psoriasis. Psoriasis 2:S7–13
Jiaravuthisan MM, Sasseville D, Vender RB, Murphy F, Muhn CY (2007) Psoriasis of the nail: anatomy, pathology, clinical presentation, and a review of the literature on therapy. J Am Acad Dermatol 57(1):1–27
Treewittayapoom C, Singvahanont P, Chanprapaph K, Haneke E (2012) The effect of different pulse durations in the treatment of nail psoriasis with 595-nm pulsed dye laser: a randomized, double-blind, intrapatient left-to-right study. J Am Acad Dermatol 66(5):807–812
Arango-Duque LC, Roncero-Riesco M, Bárcena TU, Álvarez IP, López EF (2017) Treatment of nail psoriasis with pulse dye laser plus calcipotriol betametasona gel vs. nd:YAG plus calcipotriol betamethasone gel: an intrapatient left-to-right controlled study. Actas Dermosifiliogr 108(2):140–144
Kartal SP, Canpolat F, Gonul M, Ergin C, Gencturk Z (2018) Long-pulsed nd:YAG laser treatment for nail psoriasis. Dermatol Surg 44(2):227–233
Khashaba SA, Gamil H, Salah R, Salah E (2021) Efficacy of long-pulsed Nd-YAG laser in the treatment of nail psoriasis: a clinical and dermoscopic evaluation. J Dermatological Treat 32(4):446–452
Krajewska-Włodarczyk M, Owczarczyk-Saczonek A, Placek W, Wojtkiewicz M, Wiktorowicz A, Wojtkiewicz J (2018) Ultrasound assessment of changes in nails in psoriasis and psoriatic arthritis. BioMed research international. ;2018
Rich P, Scher RK (2003) Nail Psoriasis Severity Index: a useful tool for evaluation of nail psoriasis. J Am Acad Dermatol 49(2):206–212
Hudgens S, Rich P, Geng Z, Williams D, Fleischer A, Ganguli A (2021) Development and validation of the Physician’s Global Assessment of Fingernail Psoriasis. J Eur Acad Dermatol Venereol 35(11):2324–2330
Wortsman X, Gutierrez M, Saavedra T, Honeyman J (2011) The role of ultrasound in rheumatic skin and nail lesions: a multi-specialist approach. Clin Rheumatol 30:739–748
Gutierrez M, Di Geso L, Salaffi F, Bertolazzi C, Tardella M, Filosa G, Filippucci E, Grassi W (2012) Development of a preliminary US power Doppler composite score for monitoring treatment in PsA. Rheumatology 51(7):1261–1268
Scott J, Huskisson EC (1976) Graphic representation of pain. Pain 2(2):175–184
Hintze J, LLC (2011 Sep) PASS 11. Kaysville, vol 29. NCSS, Utah, USA
Chan YH (2003) Biostatistics 102: quantitative data–parametric & non-parametric tests. Blood Press 140(2408):79
Chan YH (2003) Biostatistics 103: qualitative data-tests of independence. Singap Med J 44(10):498–503
Ranganathan P, Pramesh CS, Aggarwal R (2017) Common pitfalls in statistical analysis: measures of agreement. Perspect Clin Res 8(4):187
Roter G, Szczerkowska-Dobosz A, Nowicki RJ (2022) Treatment of nail psoriasis with pulsed dye laser versus combined pulsed dye and nd:YAG lasers—An intrapatient left‐to‐right study. Lasers Surg Med 54(5):688–692
Heidenreich R, Röcken M, Ghoreschi K (2009) Angiogenesis drives psoriasis pathogenesis. Int J Exp Pathol 90(3):232–248
Ozyurt K, Colgecen E, Baykan H, Ozturk P, Ozkose M (2012) Treatment of superficial cutaneous vascular lesions: experience with the long-pulsed 1064 nm Nd:YAG laser. The Scientific World Journal. ;2012
Tosti A, Piraccini BM (2011) Nail disorders. Harper’s Textbook Pediatr Dermatology 1:150
Elwan YH, Azim AA, Starace M, Abd Elhafiz HS (2021) Nd:YAG Laser in the treatment of nail psoriasis: Clinical and Dermoscopic Assessment. Dermatology Practical Concept. ;11(2)
Ayala F (2007) Clinical presentation of psoriasis. Reumatismo 59(s1):40–45
Haneke E Nail psoriasis: clinical features, pathogenesis, differential diagnoses, and management. Psoriasis: Targets Therapy 2017 Oct 16:51–63
Mittal J, Mahajan BB (2018) Intramatricial injections for nail psoriasis: an open-label comparative study of triamcinolone, methotrexate, and cyclosporine. Indian J Dermatol Venereol Leprol 84:419
Anders JJ, Lanzafame RJ, Arany PR (2015) Low-level light/laser therapy versus photobiomodulation therapy. Photomed Laser Surg 33(4):183
Khalkhal E, Razzaghi M, Rostami-Nejad M, Rezaei-Tavirani M, Beigvand HH, Tavirani MR (2020) Evaluation of laser effects on the human body after laser therapy. J Lasers Med Sci 11(1):91
Rodrigo SM, Cunha A, Pozza DH, Blaya DS, Moraes JF, Weber JB, de Oliveira MG (2009) Analysis of the systemic effect of red and infrared laser therapy on wound repair. Photomed Laser Surg 27(6):929–935
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
Conceptualization: [Mohamed Hussein Medhat El-Komy]; Methodology: [Mohamed Hussein Medhat El-Komy, Hagar El Sayed, Mohamed Ahmed Salem El-Basiony, Hala El Gendy]; Formal analysis and investigation: [Mohamed Ahmed Salem El-Basiony, ]; Writing - original draft preparation: [Mohamed Ahmed Salem El-Basiony, ]; Writing - review and editing: [Mohamed Hussein Medhat El-Komy, Hagar El Sayed]; Resources: [Mohamed Ahmed Salem El-Basiony]; Supervision: [Mohamed Hussein Medhat El-Komy, Nevien Ahmed Samy, Dalia Gamal Aly, Hala El-Gendy, Mohamed Fouad Abdel Salam Hassan, Hagar El Sayed, Mohamed Mohsen Soliman].
Corresponding author
Ethics declarations
Financial support and sponsorship
Nil.
Conflict of interest
The authors declare no conflict of interest.
Patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published, and due efforts will be made to conceal their identity.
Ethical committee approval
Approved.
Clinical trials registration
The trial was registered on ClinicalTrials.gov with the reference number “NCT05695833”.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El-Basiony, M.A.S., El-Komy, M.H.M., Samy, N.A. et al. Long-pulsed nd: YAG laser treatment of nail psoriasis: clinical and ultrasonographic assessment. Arch Dermatol Res 316, 365 (2024). https://doi.org/10.1007/s00403-024-03036-7
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00403-024-03036-7