
Abstract
Objective
Lumbar lordosis can be divided into two parts by a horizontal line, creating the L1 slope and the sacral slope. Despite being a major spinopelvic parameter, the L1slope (L1S) is rarely reported. However, there is some evidence that L1S is a relatively constant parameter. This study aimed to analyze the L1 slope and its relationships with other spinopelvic parameters.
Methods
Standing lateral lumbosacral x-ray radiographies of 76 patients with low back pain and CT scans of 116 asymptomatic subjects were evaluated for spinal and spinopelvic parameters including L1 slope (L1S). The x-ray and CT groups were divided into subgroups according to mean sacral slope (SS) or pelvic incidence (PI) values. The mean values of the spinopelvic parameters and the correlations between them were investigated and compared.
Results
L1S was 19.70 and 18.15 in low SS and high SS subgroups of x-ray respectively. L1S was 7.95 and 9.36 in low and high PI subgroups of CT, respectively, and the differences were insignificant statistically. L1S was the only spinal parameter that did not change as SS or PI increased in standing and supine positions. L1S was correlated with lumbar lordosis (LL) proximal lumbar lordosis (PLL) and distal lumbar lordosis (DLL) in both x-ray and CT groups. L1S was also the strongest correlated parameter with pelvic incidence lumbar lordosis mismatch (PI-LL) mismatch in supine position.
Conclusions
L1S is a relatively constant parameter and is around 16°–18° and 8°–9° in the standing and supine positions, respectively. It was significantly correlated with LL, PLL, DLL, and PI-LL. In the standing position it was nearly equal to PLL while this equality was present in low PI subgroups of CT. There is strong evidence that L1S is significantly correlated with health-related quality of life scores.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The pelvis and spine must be aligned to provide balance and minimize energy consumption during activities. This is referred to as spinopelvic alignment and is evaluated according to pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS), which also affect lumbar lordosis (LL) and thoracal kyphosis curvatures [1,2,3,4]. PT and SS are positional parameters, and PI is the sum of PT and SS. PI defines the position of the sacrum within the pelvis and is the most important parameter. PI is also a unique morphological parameter in that it does not change with position. There are strong correlations between PI, PT, SS, and LL; the higher the PI, the less vertical the sacrum. This causes an increase in the LL angle [1, 3].
Studies have shown the spinopelvic parameters to be correlated with certain spinal pathologies including scoliosis, spondylolisthesis, disc degeneration, and adjacent segment disease [4,5,6]. They are also related to the severity of pain, disability, and reductions in health-related quality of life [7, 8]. Some authors have developed predictive formulas (such as PI-LL < ± 9°) that determine the ideal LL for surgical planning [9]. LL can be divided into two parts by a horizontal line, creating the L1 slope and the sacral slope. Despite being a major spinopelvic parameter that is highly correlated with LL, the L1slope (L1S) is rarely reported. However, there is some evidence that L1S is a relatively constant parameter [10,11,12]. The present study aimed to analyze the L1S and its relationships with other spinopelvic parameters.
Materials and methods
Ethics statement
This study was conducted in accordance with the tenets of the 2013 revision of the Declaration of Helsinki. It was approved by Local Ethics Committee. Informed consent was not obtained from patients because of retrospective nature of the study.
Inclusion and exclusion criteria
This retrospective study was conducted at Harran University, Şanliurfa, Turkey. Standing lateral lumbosacral radiographies of patients with low back pain and abdominal pelvic computed tomography (CT) scans of patients with acute abdominal and urologic problems performed between June 2018 and June 2019 were reviewed. The demographic and clinical characteristics of the patients were also extracted from the medical records, including age, height, body mass index, and medical history.
In the first group (standing radiographs), patients with low back pain starting within the last three months, without motor deficit, and who were treated conservatively were included. For the second group (supine CT), we included patients who presented with acute abdominal or urological problems for which they underwent abdominal CT scans. In general, all included patients were aged between 18 and 60 years, had a body mass index of 18.5–40 kg/m2, and had no previous history or complaints of spinal, pelvic, hip, or lower extremity diseases, trauma, or surgery. In addition, the following radiological inclusion criteria were used for both groups:
-
1.
Absence of transitional lumbosacral vertebrae, spondylolisthesis, or vertebral fracture.
-
2.
Absence of radiological findings (on radiographs or CT) of degenerative spine disorder, such as the collapse of disc space, endplate sclerosis, degenerating facets, vacuum sign, or spinal stenosis.
-
3.
Coronal Cobb angle < 10°.
-
4.
In the X-ray group, LL and SS values should be within the range of values previously reported for healthy populations (20°–80° for LL and 13°–65° for SS).
-
5.
In the CT group, patients with PT values < 20° and PI–LL values < 11° were included. However, those with PI–LL values between 10°–20° were included if their PT values were < 20°.
Accordingly, 76 patients were included in the first group and 116 patients in the second group.
Measurements
The standing lateral lumbosacral plain x-ray radiography was performed on a XGEOGC80 X-ray instrument (Samsung, Korea). CT scans of all participants were performed on a Revolution GSI 256 MSCT (General Electric Healthcare, USA) with patients lying on their backs with their knees flexed. The measurements were performed on a Clear Canvas Workstation (Synaptive Medical, Canada) using Surgimap Software (Nemaris Inc. New York, USA). SS, LL, L1S, proximal (PLL), and distal lordosis (DLL) were measured on standing lumbosacral radiographies while PI, PT, SS, LL, L1S, proximal (PLL), and distal lordosis (DLL) were measured on CT. PI and PT could not be measured on x-ray because of poor visualization of femur heads in most of the cases. All measurements were performed twice by two experienced spinal surgeons. The time interval between measurements was > 2 weeks.
Parameters
-
PI: the angle between a line perpendicular to the superior sacral endplate at its midpoint and a line connecting this point to the midpoint of the axis of the femoral heads.
-
PT: the angle between a line from the midpoint of the sacral endplate to the midpoint of the femoral head axis and a vertical plumb line.
-
SS: the angle between a line parallel to the endplate of the sacrum and a horizontal line.
-
LL: the angle between a line through the superior endplate of the L1 vertebra and a line through the superior endplate of the S1 vertebra.
-
L1S: the angle between the upper endplate and a horizontal line.
-
PLL: the angle between the superior endplates of the L1 and L4 vertebra.
-
DLL: The angle between the superior endplates of the L4 and S1 vertebrae. (Figures 1 and 2).
-
PI − LL: the PI value minus the LL value.

Spinal parameters measured on lateral standing lumbosacral radiography. SS: Sacral Slope, L1S: L1 Slope, LL: Lumbar Lordosis, PLL: Proximal Lumbar Lordosis, DLL: Distal Lumbar Lordosis

Spinopelvic parameters on a midsagittal slice of lumbosacral computed tomography. PI: Pelvic Incidence, PT: Pelvic Tilt, SS: Sacral Slope, L1S: L1 Slope, LL: Lumbar Lordosis, PLL: Proximal Lumbar Lordosis, DLL: Distal Lumbar Lordosis
The measurement of PI on CT has been previously described [13]. First, the coordinates of the centers of both femur heads were found. The average of these coordinates was taken as the coordinate for the hip axis in a midsagittal slice. PI and PT were measured using this reference point.
Statistics
The interclass correlation coefficient (ICC) was used to assess intra- and interobserver reliability. Values of 0.60–0.74 and 0.75–1.00 were considered good and excellent, respectively. The mean and standard deviation of each parameter was calculated. T-tests were used to compare parameters between the low- and high PI groups. The Pearson correlation coefficient was performed to determine correlations between the parameters. The level of statistical significance was set at p < 0.05. Linear regression analysis was performed for parameter prediction.
Results
In the x-ray group there were 76 patients (36 males and40 females) with an average age of 36.74 + 13.11. The CT group included 116 subjects (54 males and 62 females), with a mean age of 41.79 ± 9.98. The intra- and interobserver ICC values for all parameters were excellent (0.88–0.94). The mean values for all of the spinopelvic and spinal parameters of the cohort are shown in Tables 1 and 2. The mean value of L1S was 18.93 + 8.15 and 8.21 + 4.33 on x-ray and CT respectively. In both groups, there was no statistically significant difference between the mean L1S values for male and female patients (X-ray: males = 18.43°, females = 19.23°; CT: males = 7.7°, females = 8.8°).
The x-ray and CT groups were divided into two subgroups according to their mean SS or PI values. Those with SS values higher than the mean SS were designated as the high SS subgroup and those with SS values lower than the mean were in the low SS subgroup for x-ray. In CT group, those with PI values higher than the mean PI were designated as the high PI subgroup and those with PI values lower than the mean were in the low PI subgroup. All of the mean spinopelvic parameters were significantly different between these groups, except L1S (Tables 3 and 4). The mean L1S was 19.70 and 18.15 in the low and high SS subgroups respectively for x-ray. For CT, It was 7.95 and 9.36 in the low PI and high PI groups, respectively, and there was no significant difference between them. In the x-ray group and the CT subgroup with low PI value, the mean PLL was nearly equal to the mean L1S, suggesting that the L4 upper endplates of the patients were nearly horizontal.
Correlations
The results of the Pearson correlation analysis of the spinal and spinopelvic parameters are shown in Tables 5 and 6. There was no statistically significant correlation between L1S and the patient’s age (X-ray: r = − 0.155, p = 0.181; CT: r = 0.111, p = 0.256).
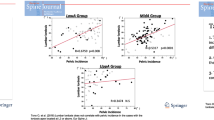
The correlations between PI, PT, SS, and LL in the total cohort were in the agreement with those found in previous studies. L1S was correlated with LL (r:0.630 for x-ray and r: 0.492 for CT), PLL (r: 0.454 for x-ray and r: 0.422 for CT), DLL (r:0.297 for x-ray and r: 0.293 for CT). L1S was the parameter with the strongest correlation with PI-LL mismatch (r: 0.749) Table 7. Linear regression analysis disclosed the following formulas:
-
For standing x-ray, LL:37.59 + 0.926 L1S.
-
For CT, PT: 0.2317PI—1.015
-
LL: 0.8276PI + 6.5835
-
PI-LL: PT-L1S, L1S: PT-(PI-LL)
-
L1S: 0.0593PI + 5.57 with an average PI value of 45°–50° L1S was nearly 8°–8.5°.
The predictive formula for PI-LL mismatch using L1S was established as:
-
PI-LL: 8.6529-0.9109L1S.
Discussion
According to Roussoly, LL is measured between the inflection point and the upper S1 endplate [14]. The inflection point is the location that determines the border of LL and thoracic kyphosis. This angle may contain more than five vertebral bodies and can be divided by a horizontal line through the apex of LL. The upper arc is constant at 15°–17°, while the lower arc is the SS [10, 14]. In most cases, the inflection point is around the L1 body. Otherwise, the angle of the upper arc differs by less than 1° from the L1S so resembles the L1S. Hey et al. found L1 to be the only vertebrae with a similar vertebral slope (14.4°–16.3°) across Roussoly curve types [11].
The two formulas that allow us to determine the mean L1S from clinical and radiological studies are:
L1S = LL-SS.
PI-LL = PT + SS-(L1S + SS) = PT-L1S.
L1S: PT-(PI-LL).
In a systematic review of spinopelvic parameters in asymptomatic patients, (2926 patients from 17 studies), the mean L1S was found to be 16.1° [15]. In a series by Bourret et al., the mean L1S were 17.3°, 18.3°, and 17.6° in 486 asymptomatic patients with low, normal, and high PI, respectively [16]. Pesenti et al. found mean L1S of 20.3°, 20.6°, and 18.8° in low, normal, and high PI groups, respectively [17]. Bourret et al. also reported the following equations [16]:
LL = 28.4291 + 0.5578PI.
PT = − 10.2499 + 0.4374PI.
PI-LL = − 28.4291 + 0.4422 PI From this, we can calculate the mean S1 slope as follows:
L1S = 18.18°−0.005PI.
Similar results were obtained from regression analyses by Legaye and Duval-Beaupere, Le Huec et al., and Hasegawa et al. [18,19,20] A PI of 0.005 is negligible because of its very low value. This finding suggests that L1S is relatively constant at around 18°.
In our study for CT, L1S was 0.06 (PI) + 5.57°, with an average PI value of 45°–50° L1S was nearly 8°–8.5°. The difference was due to the supine position used for our CT studies. In the supine position, the LL decreases by 3°–5°, while the SS increases by 3°–5°. So, L1S decreases by 8°–10°. Therefore, based on our results, the mean L1S in a standing position would be ~ 18°.This finding is also supported by the study of Hariyama et al. concluded that positional change in lordosis occurred primarily through the upper lumbar segments [21]. In our study, the PI and LL values for all groups (cumulative, low, and high PI) were nearly equal so the values of PI-LL were − 1.05°–1.4°. This finding is in accord with those from other studies performed with patients in the supine position [22, 23]. According to LL prediction formulas such as those described by Le Huec et al. and Hasegawa et al. [19], LL = 0.50PI + 28. Thus, LL is 3°–4° greater than PI when PI is less than 60°. This means that, in most cases, LL will decrease and become closer to PI when the patient is in the supine position. [19]
These findings also support the hypothesis that L1S is not significantly correlated with PI. We found that L1S was correlated with LL, PLL, DLL, and PI-LL. These relationships with other spinopelvic parameters are in line with those previously reported [12]. L1S and PT were the parameters with the strongest correlations with PI-LL; although, the correlation between L1S and PI-LL was negative. PI-LL is an important spinal parameter and has been found to modify adult spinal deformity (ASD) classifications [24].
We also found L1S to be correlated with PLL and DLL. In the x-ray group and low PI subgroup of CT, the mean PLL value was equal to the mean L1S value so, SS = DLL. This finding is in agreement with those of Hey et al., who found an L4 vertebral slope of ~ 0° in Roussoly groups 1 and 2 (low PI) [11]. However, in the Pesenti et al. cohort, DLL was nearly equal to SS in their average PI group (PI: 45°–65°) [17], Therefore, L1S nearly equals PLL in patients with low PIs.
There were several limitations in our study. First, absence of PI and PT parameters in x-ray group. Although lateral lumbar radiography is a good alternative to whole spine radiography for the measurement of spinopelvic parameters [25], in our series poor identification of hip centers was present in most of the cases so we could not measure PI and PT values. However, SS is a highly correlated parameter with PI and high SS and low SS groups could represent high PI and low PI groups respectively. Another associated problem was not able to use spinal modifiers in the X-ray group for the detection of deformity patients. Adult spinal deformity is usually associated with spinal degenerative disorders and a loss of lordosis. Such marked spinal degenerative changes are commonly seen in the elderly population; therefore, these patients were excluded from our study.
Another limitation was the mismatch between the X-ray and CT groups. We evaluated L1S and its relationships with other parameters in two different positions (standing X-rays and supine CT). Because of the retrospective nature of the study, patients in the X-ray group were symptomatic while those in the CT groups were asymptomatic. To minimize this effect, we ensured that the patients in the group X-ray were only mildly symptomatic without motor deficits; also, they were relatively young. Therefore, the mean L1S, LL, and SS values reported for this group were very close to that of healthy subjects and can be accepted as an asymptomatic group. On the other hand, we thought that evaluation of spinopelvic parameters in supine position strengthened our study, because the importance of supine imaging tools has been increasing for several reasons [26,27,28]. First, the correlation between the spinopelvic parameters are strongest in the supine position and lumbosacral sagittal alingment in the supine position is appromixately equal to that in the prone position which is actually intraoperative position, so supine images can be helpful for the surgical planing [26]. Second, the difference between LL values measured in supine and standing position was found correlated with postoperative outcome in the patients with adult spinal deformity [27, 28]. We believe that supine imaging will be utilized more commonly in the future for the diagnosis and the treatment of spinal disease.
Conclusion
L1S is a relatively constant parameter and is around 18–19° and 8°–9° in the standing and supine positions, respectively. It is significantly correlated with LL, PLL, DLL, and PI-LL. In those with low PI values, L1S equals PLL. L1S is also the parameter with the strongest correlation with PI-LL and it is equal to the difference between two important modifiers of SRS-Schwab ASD classification (PT, PI-LL). However, more studies are needed to corroborate these results.
References
- J, Legaye G, Duval-Beaupère J, Hecquet C, Marty (1998) Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J 7(2):99–103. https://doi.org/10.1007/s005860050038
- Mac-Thiong JM, Hubert Labelle M, Charlebois M-P, Huot, Jacques A, de Guise (2003) Sagittal plane analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type. Spine (Phila Pa 1976) 28(13):1404–1409. https://doi.org/10.1097/01.BRS.0000067118.60199.D1
- Mac-Thiong JM, Hubert Labelle M, Charlebois M-P, Huot, Jacques A, de Guise, Le Huec JC, Aunoble S, Philippe L (2011) Le Huec JC, S Aunoble, Leijssen Philippe Pellet Nicolas. Pelvic parameters: origin and significance. Eur Spine J. 20 Suppl 5(Suppl 5):564 – 71. https://doi.org/10.1007/s00586-011-1940-1. Epub 2011 Aug 10
- Labelle H, Roussouly P, Berthonnaud E, Transfeldt E, O’Brien M, Chopin D, Hresko T, Dimnet J (2004) Spondylolisthesis, pelvic incidence, and spinopelvic balance: a correlation study. Spine (Phila Pa 1976) 29(18):2049–2054. https://doi.org/10.1097/01.brs.0000138279.53439.cc
- Roussouly P, Gollogly S, Berthonnaud E (2005) Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position Johanes Dimnet. Spine (Phila Pa 1976) 30(3):346–353. https://doi.org/10.1097/01.brs.0000152379.54463.65
- G, Vaz P, Roussouly E, Berthonnaud (2002) J DimnetSagittal morphology and equilibrium of pelvis and spine. Eur Spine J 11(1):80–87. https://doi.org/10.1007/s005860000224
Kyrölä K, Repo J, Mecklin J-P, Ylinen J, Kautiainen H, Häkkinen A (2018) Spinopelvic changes based on the simplified SRS-Schwab adult spinal deformity classification: relationships with disability and health-related quality of life in adult patients with prolonged degenerative spinal disorders. Spine (Phila Pa 1976) 43(7):497–502. https://doi.org/10.1097/BRS.0000000000002370
Takemoto M, Boissière L, Vital J-M, Pellisé F, Perez-Grueso FJS, Kleinstück F, Acaroglu ER, Alanay A, Obeid I (2017) Are sagittal spinopelvic radiographic parameters significantly associated with quality of life of adult spinal deformity patients? Multivariate linear regression analyses for pre-operative and short-term post-operative health-related quality of life. Eur Spine J 26(8):2176–2186. https://doi.org/10.1007/s00586-016-4872-y. Epub 2016 Nov 18
Schwab F, Patel A, Ungar B et al (2010) Adult spinal deformity-postoperative standing imbalance:how much can you tolerate? Anoverview of key parameters in assessing alingment and planning corrective surgery.Spine. (Phila Pa 1976) 35:2224–2231
Berthonnaud E, Dimnet J, Roussouly P, Labelle H (2005) Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. J Spinal Disord Tech 18(1):40–47. https://doi.org/10.1097/01.bsd.0000117542.88865.77
Hey HWD, Tan KA, Thadani VN, Liu GK, Wong HK (2020) Characterization of Sagittal Spine Alignment with reference to the gravity line and vertebral slopes: an analysis of different Roussouly Curves. Spine (Phila Pa 1976) 45(9):E481–E488. https://doi.org/10.1097/BRS.0000000000003379
Choi SH, Son SM, Lee D-H, Lee CS, Shin WC, Hong CG, Lee JS, Hwang CJ (2018) L1 incidence reflects pelvic incidence and lumbar lordosis mismatch in sagittal balance evaluation. Med (Baltim) 97(30):e11668. https://doi.org/10.1097/MD.0000000000011668
İplikçioğlu AC, Karabağ H (2022) Validity and reliability of spinopelvic parameters measured on computed tomography. Int J Spine Surg 16(5):875–880. https://doi.org/10.14444/8344. Epub 2022 Aug 25
Roussouly P, Berthonnaud E, Dimnet J (2003) [Geometrical and mechanical analysis of lumbar lordosis in an asymptomatic population: proposed classification]. Rev Chir Orthop Reparatrice Appar Mot 89(7):632–639
Noshchenko A, Hoffecker L, Cain CMJ, Patel VV, Burger EL (2017) Spinopelvic parameters in asymptomatic subjects without spine disease and deformity: a systematic review with Meta-analysis. Clin Spine Surg 30(9):392–403. https://doi.org/10.1097/BSD.0000000000000533
Bourret S, Cerpa M, Kelly MP, Hasegawa K, Hwee Hey WD, Wong H-K, Liu G, Sardar ZM, Riahi H, Lenke LG, Huec JCL (2022) Correlation analysis of the PI-LL mismatch according to the pelvic incidence from a database of 468 asymptomatic volunteers. Eur Spine J 31(6):1413–1420. https://doi.org/10.1007/s00586-021-07087-6. Epub 2022 Mar 24
Pesenti S, Lafage R, Stein D, Elysee JC, Lenke LG, Schwab FJ, Kim HJ, Lafage V (2018) The amount of proximal lumbar lordosis is related to pelvic incidence. Clin Orthop Relat Res 476(8):1603–1611. https://doi.org/10.1097/CORR.0000000000000380
Legaye J, Duval-Beaupère G (2005) Sagittal plane alignment of the spine and gravity: a adiological and clinical evaluation. Acta Orthop Belg 71(2):213–220
Le Huec JC, Hasegawa K (2016) Normative values for the spine shape parameters using 3D standing analysis from a database of 268 asymptomatic caucasian and Japanese subjects. Eur Spine J 25(11):3630–3637 Epub 2016 Mar 7
Hasegawa K, Okamoto M, Hatsushikano S, Shimoda H, Ono M, Watanabe K (2016) Normative values of spino-pelvic sagittal alignment, balance, age, and health-related quality of life in a cohort of healthy adult subjects. Eur Spine J 25(11):3675–3686 Epub 2016 Jul 18
Harimaya K, Lenke LG, Mishiro T, Bridwell KH, Koester LA, Sides BA (2009) Increasing lumbar lordosis of adult spinal deformity patients via intraoperative prone positioning. Spine (Phila Pa 1976) 34(22):2406–2412. https://doi.org/10.1097/BRS.0b013e3181bab13b
Baker JF, Robertson PA (2020) Segmental contributions to lumbar lordosis: a computed Tomography Study. Int J Spine Surg 14(6):949–955. https://doi.org/10.14444/7144. Epub 2020 Dec 29
Chevillotte T, Coudert P, Cawley D, Bouloussa H, Mazas S, Boissière L, Gille O (2018) Influence of posture on relationships between pelvic parameters and lumbar lordosis: comparison of the standing, seated, and supine positions. A preliminary study. Orthop Traumatol Surg Res 104(5):565–568. https://doi.org/10.1016/j.otsr.2018.06.005. Epub 2018 Jul 31
Schwab FJ, Blondel B, Bess S, Hostin R, Shaffrey CI, Smith JS, Boachie-Adjei O, Burton DC, Akbarnia BA, Mundis GM, Ames CP, Kebaish K, Hart RA, Farcy J-P, Lafage V, International Spine Study Group (ISSG) (2013) Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine (Phila Pa 1976) 38(13):E803–E812. https://doi.org/10.1097/BRS.0b013e318292b7b9
Tarpada SP, Cho W, Chen F, Amorosa LF (2018) Utility of Supine lateral radiographs for Assessment of lumbar segmental instability in degenerative lumbar spondylolisthesis. Spine (Phila Pa 1976) 43(18):1275–1280. 0.1097/BRS.0000000000002604
Yasuda T, Hasegawa T, Yamato Y, Togawa D, Kobayashi S, Yoshida G, Banno T, Arima H, Oe S, Matsuyama Y (2018) Effect of position on lumbar lordosis in patients with adult spinal deformity. J Neurosurg Spine 29(5):530–534. https://doi.org/10.3171/2018.3.SPINE1879
Elysee JC, Lovecchio F, Lafage R, Ang B, Huang A, Bannwarth M, Kim HJ, Schwab F, Lafage V (2022) Supine imaging is a Superior Predictor of Long-Term Alignment following adult spinal deformity surgery. Global Spine J 12(4):631–637 Epub 2020 Sep 25
Ohyama S, Aoki Y, Inoue M, Kubota G, Watanabe A, Nakajima T, Sato Y, Takahashi H, Nakajima A, Saito J, Eguchi Y, Orita S, Inage K, Shiga Y, Nakagawa K, Ohtori S (2021) Influence of preoperative difference in lumbar lordosis between the Standing and Supine positions on clinical outcomes after single-level transforaminal lumbar Interbody Fusion: Minimum 2-year follow-up. Spine (Phila Pa 1976) 46(16):1070–1080. https://doi.org/10.1097/BRS.0000000000003955
Funding
No funding was received for this research.
Open access funding provided by the Scientific and Technological Research Council of Türkiye (TÜBİTAK).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
This study was conducted in accordance with the 2013 revision of Declaration of Helsinki. It was approved by the Local Ethics Committee.
Informed consent
The requirement of informed consent was waived due to the retrospective nature of this study.
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Iplikcioglu, A.C., Karabag, H. L1 slope: an overlooked spinal parameter. Arch Orthop Trauma Surg 144, 2077–2083 (2024). https://doi.org/10.1007/s00402-024-05311-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-024-05311-8