
Abstract
Purpose
The aim of this study was to evaluate whether daily consumption of coffee and tea was associated with components and prevalence of metabolic syndrome (MetS) in the Polish arm of the Health, Alcohol and Psychosocial factors In Eastern Europe cohort study.
Methods
A cross-sectional population-based survey including 8,821 adults (51.4 % female) was conducted in Krakow, Poland. Coffee and tea consumption was evaluated using food frequency questionnaires. MetS was defined according to the International Diabetes Federation definition. Linear and logistic regression models were performed to estimate odds ratios and confidence intervals.
Results
Among high coffee and tea consumers (3 or more cups/day), high prevalence of female gender, young age, medium–high educational and occupational level, high total energy intake, and smoking habit were found. High coffee drinkers had lower BMI, waist circumference, systolic and diastolic blood pressure, triglycerides, and higher HDL cholesterol than those drinking less than 1 cup/day. In contrast, high tea consumers had lower BMI, waist circumference, but not diastolic blood pressure, which was higher than low drinkers. After adjusting for potential confounding factors, both higher coffee and tea consumption were negatively associated with MetS (OR 0.75, 95 % CI 0.66, 0.86 and OR 0.79, 95 % CI 0.67, 0.92, respectively). Among specific components of MetS, high coffee consumption was negatively associated with waist circumference, hypertension, and triglycerides, whereas tea consumption with central obesity and fasting plasma glucose in women, but not in men.
Conclusions
Coffee and tea consumption was negatively associated with MetS and some of its components.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Metabolic syndrome (MetS) is defined by the presence of a group of cardiovascular risk factors, such as hyperglycemia, dyslipidemia, hypertension, and abdominal obesity, which clustered together are associated with greater cardiovascular disease risk [1, 2]. The prevalence of MetS has increased over recent decades, reaching alarming rates worldwide [3, 4]. However, there are important differences between regions, which could be attributed to diet and lifestyle that specifically differ by country [5, 6]. A protective effect is attributable, at least in part, to the contents of plant-derived foods and bioactive phytochemicals in the diet. Indeed, the components of MetS have been inversely associated with dietary pattern including polyphenol-rich foods, such as fruit and vegetables as well as olive oil and red wine [7].
Recently, increasing experimental and epidemiological studies pointed out the possible beneficial effects of coffee and tea on cardiovascular disease risk [8]. These two beverages are among the most consumed worldwide, with higher amount, especially in non-Mediterranean countries [9, 10]. Epidemiological studies showed that regular coffee intake improved some components of the MetS, including hypertension and diabetes mellitus [11, 12]. Tea consumption has been reported to protect against cardiovascular disease (CVD) by reducing blood pressure, blood glucose levels, and body weight [13]. The beneficial effects of tea and coffee consumption could be explained by their high content of vitamins and polyphenols, which are suggested to be negatively associated with chronic diseases [14, 15]. The potential health benefits depend on their antioxidant and antiinflammatory bioactivity, which may contribute to their protective role against CVD [16]. A growing number of studies have suggested that coffee and tea polyphenols may be useful for the prevention of obesity and MetS [17, 18]. Although results of experimental studies are not conclusive, the effects of tea and coffee consumption should be evaluated in the observational studies, since acute administration of caffeinated beverages in clinical trials leads to inconsistent or detrimental effects on health [19].
Studies regarding the association of coffee and tea consumption with MetS are scarce. Some studies conducted in Japan demonstrated a significant inverse correlation between coffee intake and MetS [20–22]. Other studies conducted in the European setting failed to demonstrate any relation [23–25], whereas another study conducted in a Mediterranean area reported a favorable effect [26]. However, investigations conducted on large and well-established nutritional cohorts are still lacking.
The aim of this study was to evaluate whether daily consumption of coffee and tea was independently associated with components and prevalence of MetS in a large cohort from the Krakow town in Poland. The association of coffee and tea consumption with multiple markers for MetS, including body mass index (BMI), waist circumference (WC), fasting plasma glucose (FPG), total cholesterol, HDL-cholesterol (HDL-c), LDL-cholesterol (LDL-c), serum triglycerides, and systolic and diastolic blood pressure (SBP and DBP, respectively), was explored.
Subjects and methods
Study population
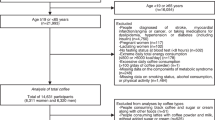
Subjects were participants of the Polish arm of the Health, Alcohol and Psychosocial factors In Eastern Europe (HAPIEE) study, which was a prospective cohort study aimed to investigate the determinants of CVD and other chronic conditions in Central and Eastern Europe. The study protocol with the rationale, design, and methods has been described in detail elsewhere [27]. Briefly, a random sample of 10,728 subjects (aged 45–69 year) was recruited at the baseline survey conducted in 2002–2005 (response ratio of 59 %) in the urban area of Krakow, Poland. The survey involved completion of structured questionnaires and an examination in clinic. The questionnaires covered health, medical history, health behavior, socioeconomic circumstances, psycho-social factors, and diet. The participants provided written informed consent, and the study protocol was approved by the ethics committee at University College London, UK and by the bioethics committee of the Jagiellonian University (no. KE/99/03/B/284 2).
Among participants who attended the clinical visit (n = 9,050), those with missing outcome measures, with incomplete (more than 50 % of answers missing) or incongruent (energy intake <500/>4,000 kcal/day for females and <800/>5,000 kcal/day for males) data regarding dietary information were excluded, resulting in a final sample of 8,821 adults (51.4 % female).
Demographic and lifestyle information
Socio-demographic and lifestyle characteristics included age, gender, educational and occupational level, smoking, and alcohol drinking habits. Educational level was categorized as (1) low (primary/secondary), (2) medium (high school), and (3) high (university). Occupational level was categorized as (1) low (unskilled/unemployed workers), (2) medium (partially skilled workers), and (3) high (skilled workers). Physical activity level was categorized as daily (1) low active [expended energy <16.7 kJ (<4 kcal)/min], (2) moderately active [expended energy 16.7–29.3 kJ (4–7 kcal)/min], and (3) highly active [expended energy >29.3 kJ (7 kcal)/min]. Smoking status was categorized as (1) non-smoker and (2) current smoker. Alcohol consumption was categorized as (1) none or moderate drinker (<12 g/day) and (2) alcohol drinker (>12 g/day).
Dietary assessment
Dietary data were collected by using a food frequency questionnaire (FFQ) based on the tool developed by Willett et al. [28] and subsequently adapted in the Whitehall II Study [29]. The FFQs consisted of 148 food and drink items. An instruction manual that included photographs to facilitate the estimation of portion sizes was used. Participants were asked how often, on average, they had consumed that amount of the item during the last 3 months, with nine responses ranging from “never or less than once per month” to “six or more times per day”. Moreover, participants were asked to include additional foods and frequency of consumption by manual entry.
The average beverage consumption was calculated (in mL) by following the standard portion sizes used in the study and then converted in 24-h intake. For the sake of simplicity, we categorized coffee and tea consumption according to standard cup of coffee (150 mL) and tea (250 mL) in (1) <1 cup/day, (2) 1–2 cups/day, and (3) 3 or more cups/day.
Clinical measurements
The physical examination included measurement of height, weight, waist circumference, and blood pressure using standard procedures [27]. MetS was defined according to the International Diabetes Federation definition, as having central obesity (WC ≥ 90 cm in men and ≥80 cm in women) and any two of the following: (1) triglycerides >150 mg/dL (1.7 mmol/L), or specific treatment for this lipid abnormality; (2) HDL-c <40 mg/dL (1.03 mmol/L) in males, <50 mg/dL (1.29 mmol/L) in females, or specific treatment for this lipid abnormality; (3) SBP >130 or DBP >85 mm Hg, or treatment of previously diagnosed hypertension; and (4) FPG >100 mg/dL (5.6 mmol/L), or previously diagnosed type two diabetes or treatment of previously diagnosed diabetes [30].
Statistical analysis
Continuous variables are presented as means and standard deviations (SDs), categorical variables as frequencies and percentages. Variables were examined for normality and skewness (Kolmogorov and Levene tests). One-way ANOVA using Bonferroni correction and Kruskal–Wallis test was used for comparisons of continuous variables, and Chi-square test was used for categorical variables. Linear trends across the coffee consumption categories were tested by assigning each participant the median of the category and modeling this value as a continuous variable. Multivariable logistic regression models were performed to assess the relationship between metabolic parameters (BMI, WC, HDL-c, LDL-c, total cholesterol, FPG, SBP, and DBP) as dependent variables and coffee and tea consumption categories as exposure variables by odds ratios (ORs) and 95 % confidence intervals (CIs). Gender-specific analyses were also conducted to take into account the natural differences in body composition and caloric needs between men and women. Endpoints were adjusted for gender, age, educational level, occupational level, physical activity, smoking status, alcohol drinking, and total energy intake. p values <0.05 (two-tailed) were considered significant. Analyses were performed using SPSS software v17.0 (Chicago, USA).
Results
Baseline characteristics of the 8,822 subjects included in the analysis by coffee and tea consumption category are presented in Table 1. Among high coffee consumers (3 or more cups/day), a higher prevalence of female gender, younger age (average 56.8 years), higher total energy intake, and medium–higher educational and occupational level were found. A significant different distribution was found also according smoking status and alcohol drinking (Table 1). Similar trends were found regarding tea consumption with respect to gender (female) and total energy intake (higher mean intake). High tea consumers were also mostly smokers, not alcohol drinkers, and high physically active.
When examining the association between coffee and tea consumption and various anthropometric measures, a significant inverse trend across categories of coffee consumption was found for BMI (P < 0.001), WC (P < 0.001), SBP (P < 0.001), DBP (P < 0.001), triglycerides (P = 0.014), and a direct association with HDL-c (P = 0.024) and LDL-c (P = 0.045) (Table 2). In contrast, significant inverse trend was found for categories of tea drinking and only BMI (P < 0.001) and WC (P = 0.036) (Table 2).
Both coffee and tea consumption were inversely associated with having MetS (Tables 3, 4). The multivariable regression analysis of overall sample, adjusted for gender, age, educational level, occupational level, physical activity, smoking status, alcohol drinking, total energy intake, and tea consumption, revealed that high coffee consumption (>2 vs. <1 cup/day) was significantly associated with several components of MetS, such as WC, blood pressure cut offs, and triglycerides (Table 3). When the analysis was repeated by gender, coffee consumption was inversely related to WC in men, but not in women, whereas among the latter a significant association with hypertension and low HDL-c was found (Table 3). Results about tea consumption were slightly different (Table 4). Despite the high consumption of tea was inversely related with having MetS, the analysis stratified by gender revealed a significant association for men, but not for women. The strongest relation was between tea consumption and central obesity, with a trend over categories of tea consumption in both men and women. Finally, tea consumption was also inversely related to FPG in women, but not in men.
Discussion
In the present study, we evaluated the relationship between coffee and tea consumption with cardiovascular risk factors and MetS in a large sample of men and women living in Krakow, Poland. Both coffee and tea consumption were negatively associated with MetS. The overall prevalence of MetS in the sample was 27.9 %, similar to previous reports from Poland [31–33]. The proportion of MetS in low and high consumers of coffee was 30.2 and 23.7 %, respectively. Similar differences were found for tea consumers, for instance, 30.8 % among low consumers and 26.4 % in high consumers.
The relationship between coffee consumption and MetS has not yet been well investigated, and results of previous epidemiological studies are contrasting. Several studies reported that coffee consumption was inversely associated with MetS in the Japanese population [20–22]. On the other hand, studies conducted in central [23, 24] and north [25] European countries reported no relation between coffee consumption and the development of MetS or its components. In contrast, a previous study conducted in a Southern European region (namely the Mediterranean area) showed a negative (beneficial) association [26]. Epidemiological studies exploring the favorable effect of tea consumption on MetS have reported more univocal results, such as an inverse association [34–36] and others even a therapeutic effect [37–39]. We reported an overall negative association between coffee and tea consumption and MetS, but contrarily to the previous studies, and this association was more remarked for coffee, rather than for tea. The components of MetS that have been found to be more susceptible to consumption of coffee and tea were primarily central obesity, with no differences between men and women, whereas association with cholesterol and glucose metabolisms greatly depended on the type of beverages and gender. Our results confirm in part the findings reported in previous studies assessing that habitual consumptions of tea were favorably associated with triglycerides [40], FPG [41, 42] and body fat [43], whereas coffee was more likely associated with improvements in glucose and insulin metabolism [44] as well as with BMI and WC [45].
Although the exact mechanism through which coffee and tea may prevent MetS is still unclear, previous studies suggested that their healthy effects on chronic diseases may depend on the antioxidant compounds contained in both coffee and tea [46]. These beverages contain significant amounts of vitamins and minerals, such as ascorbic acid (vitamin C), several B vitamins, riboflavin, niacin, folic acid, pantothenic acid, magnesium, potassium, manganese, and fluoride [47, 48]. Among other bioactive compounds, polyphenols are among the best candidates to be responsible for the beneficial actions of coffee and tea consumption on various metabolic disorders [49]. The polyphenols found in coffee are hydroxycinnamic acids (such as caffeic and ferulic acids), among which the most effective against CVD have been reported to be isomers of chlorogenic acid [17]. The main polyphenols contained in tea belong to the family of the catechins, flavanols, flavanol glycosides, flavandiols, and depsides [18]. The beneficial effects of polyphenols contained in coffee and tea in preventing chronic diseases (especially CVD) could be due to their ability to ameliorate endothelial function [50], suppress vascular endothelial cell expression of pro-inflammatory cytokines [51], and consequent upregulation of adhesion molecules and monocyte adhesion [52]. Among the other effects, tea has been demonstrated to ameliorate insulin resistance [53], whereas coffee has been associated with adiponectin levels [54]. However, differences in type and content of polyphenols depending on quality of both coffee and tea may result in a stronger beneficial effect of one rather than the other and this issue needs to be investigated further.
Some mechanisms to explain the healthful effects related to caffeine on preventing the MetS have been hypothesized, including sympathetic over activation, antagonism of adenosine receptors, increased norepinephrine release, a sympathomimetic agent that is capable of increasing energy expenditure, and promoting the loss of body fat [55, 56]. On the other hand, other studies failed in to demonstrate such beneficial effects and reported that caffeine may explicate itself favorable effects on the various components of the MetS [57].
Our study has some limitations that should be addressed. First, because of its cross-sectional nature, the associations retrieved in the study do not indicate causality. Reverse causation should be taken into account when exploring behavioral choices that may be influenced by health status. Also, coffee and tea consumption could be influenced by other lifestyle characteristics and not be equally distributed by social status. Adjustment for smoking status and education, which was done in our analysis, could not be sufficient to control the confounding effect of background characteristics. Second, the question regarding tea consumption was not specific for different types of tea. Despite the participants were allowed to add supplementary foods, such as green and herbal teas, the most of them did not differentiate between types of tea, thus not allowing us to assess possible differences on effects. Moreover, dietary information was self-reported, which may have led to recall bias. Finally, health information of individuals not included in the analysis due to lack of blood samples should be taken into account when considering our results. However, despite these limitations, our findings remain of significant value, since this was the first study describing the relationship between consumption of coffee and tea and components of MetS in a large sample from East Europe.
In conclusion, a significant negative association between coffee consumption and prevalence of MetS both in men and in women was found, whereas tea consumption was associated with MetS only in men. High coffee and tea consumption were also associated with a decreased prevalence of central obesity and better cholesterol and glucose metabolism. These findings reinforce the hypothesis on the possible health benefits of polyphenols. Due to methodological limitations, we cannot exclude that the observed associations on coffee/tea and MS are due to other healthy lifestyle behaviors, and further prospective studies are needed to better adjust for potential confounding factors.
References
Eckel RH, Grundy SM, Zimmet PZ (2005) The metabolic syndrome. Lancet 365:1415–1428
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC Jr, Spertus JA, Costa F (2005) Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 112:2735–2752
Ford ES, Giles WH, Dietz WH (2002) Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA 287:356–359
Hu G, Qiao Q, Tuomilehto J, Balkau B, Borch-Johnsen K, Pyorala K (2004) Prevalence of the metabolic syndrome and its relation to all-cause and cardiovascular mortality in nondiabetic European men and women. Arch Intern Med 164:1066–1076
Grosso G, Mistretta A, Frigiola A, Gruttadauria S, Biondi A, Basile F, Vitaglione P, D’Orazio N, Galvano F (2014) Mediterranean diet and cardiovascular risk factors: a systematic review. Crit Rev Food Sci Nutr 54:593–610
Buscemi S, Sprini D, Grosso G, Galvano F, Nicolucci A, Lucisano G, Massenti FM, Amodio E, Rini GB (2014) Impact of lifestyle on metabolic syndrome in apparently healthy people. Eat Weight Disord 19:225–232
Grosso G, Pajak A, Mistretta A, Marventano S, Raciti T, Buscemi S, Drago F, Scalfi L, Galvano F (2014) Protective role of the Mediterranean diet on several cardiovascular risk factors: evidence from Sicily, southern Italy. Nutr Met Cardiovasc Discov 24:370–377
Bohn SK, Ward NC, Hodgson JM, Croft KD (2012) Effects of tea and coffee on cardiovascular disease risk. Food Funct 3:575–591
Thompson WG (1994) Coffee: brew or bane? Am J Med Sci 308:49–57
Weisburger JH (1997) Tea and health: a historical perspective. Cancer Lett 114:315–317
Jiang X, Zhang D, Jiang W (2014) Coffee and caffeine intake and incidence of type 2 diabetes mellitus: a meta-analysis of prospective studies. Eur J Nutr 53:25–38
Steffen M, Kuhle C, Hensrud D, Erwin PJ, Murad MH (2012) The effect of coffee consumption on blood pressure and the development of hypertension: a systematic review and meta-analysis. J Hypertens 30:2245–2254
Psaltopoulou T, Ilias I, Alevizaki M (2010) The role of diet and lifestyle in primary, secondary, and tertiary diabetes prevention: a review of meta-analyses. Rev Diabet Stud 7:26–35
Grosso G, Bei R, Mistretta A, Marventano S, Calabrese G, Masuelli L, Giganti MG, Modesti A, Galvano F, Gazzolo D (2013) Effects of vitamin C on health: a review of evidence. Front Biosci (Landmark Ed) 18:1017–1029
Godos J, Pluchinotta FR, Marventano S, Buscemi S, Li Volti G, Galvano F, Grosso G (2014) Coffee components and cardiovascular risk: beneficial and detrimental effects. Int J Food Sci Nutr 21:1–12
Barnes S, Prasain J, D’Alessandro T, Arabshahi A, Botting N, Lila MA, Jackson G, Janle EM, Weaver CM (2011) The metabolism and analysis of isoflavones and other dietary polyphenols in foods and biological systems. Food Funct 2:235–244
Meng S, Cao J, Feng Q, Peng J, Hu Y (2013) Roles of chlorogenic acid on regulating glucose and lipids metabolism: a review. Evid Based Complement Alternat Med 2013:801457
Islam MA (2012) Cardiovascular effects of green tea catechins: progress and promise. Recent Pat Cardiovasc Drug Discov 7:88–99
Geleijnse JM (2008) Habitual coffee consumption and blood pressure: an epidemiological perspective. Vasc Health Risk Manag 4:963–970
Matsuura H, Mure K, Nishio N, Kitano N, Nagai N, Takeshita T (2012) Relationship between coffee consumption and prevalence of metabolic syndrome among Japanese civil servants. J Epidemiol 22:160–166
Hino A, Adachi H, Enomoto M, Furuki K, Shigetoh Y, Ohtsuka M, Kumagae S, Hirai Y, Jalaldin A, Satoh A, Imaizumi T (2007) Habitual coffee but not green tea consumption is inversely associated with metabolic syndrome: an epidemiological study in a general Japanese population. Diabetes Res Clin Pract 76:383–389
Takami H, Nakamoto M, Uemura H, Katsuura S, Yamaguchi M, Hiyoshi M, Sawachika F, Juta T, Arisawa K (2013) Inverse correlation between coffee consumption and prevalence of metabolic syndrome: baseline survey of the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study in Tokushima, Japan. J Epidemiol 23:12–20
Driessen MT, Koppes LL, Veldhuis L, Samoocha D, Twisk JW (2009) Coffee consumption is not related to the metabolic syndrome at the age of 36 years: the Amsterdam Growth and Health Longitudinal Study. Eur J Clin Nutr 63:536–542
Balk L, Hoekstra T, Twisk J (2009) Relationship between long-term coffee consumption and components of the metabolic syndrome: the Amsterdam Growth and Health Longitudinal Study. Eur J Epidemiol 24:203–209
Hostmark AT (2010) The Oslo health study: soft drink intake is associated with the metabolic syndrome. Appl Physiol Nutr Metab 35:635–642
Grosso G, Marventano S, Galvano F, Pajak A, Mistretta A (2014) Factors associated with metabolic syndrome in a Mediterranean population: role of caffeinated beverages. J Epidemiol 24:327–333
Peasey A, Bobak M, Kubinova R, Malyutina S, Pajak A, Tamosiunas A, Pikhart H, Nicholson A, Marmot M (2006) Determinants of cardiovascular disease and other non-communicable diseases in Central and Eastern Europe: rationale and design of the HAPIEE study. BMC Public Health 6:255
Brunner E, Stallone D, Juneja M, Bingham S, Marmot M (2001) Dietary assessment in Whitehall II: comparison of 7 d diet diary and food-frequency questionnaire and validity against biomarkers. Br J Nutr 86:405–414
Willett WC, Sampson L, Stampfer MJ, Rosner B, Bain C, Witschi J, Hennekens CH, Speizer FE (1985) Reproducibility and validity of a semiquantitative food frequency questionnaire. Am J Epidemiol 122:51–65
Alberti KG, Zimmet P, Shaw J (2006) Metabolic syndrome–a new world-wide definition. A consensus statement from the international diabetes federation. Diabet Med 23:469–480
Janszky I, Vatten L, Romundstad P, Laugsand LE, Bjorngard JH, Manczuk M, Zatonski WA (2011) Metabolic syndrome in Poland—the PONS Study. Ann Agric Environ Med 18:270–272
Ilow R, Regulska-Ilow B, Rozanska D, Kowalisko A, Biernat J (2012) Prevalence of metabolic syndrome among 40- and 50-year-old inhabitants of Wroclaw, Poland. Ann Agric Environ Med 19:551–556
Szurkowska M, Szafraniec K, Gilis-Januszewska A, Pach D, Krzentowska A, Szybinski Z, Huszno B (2006) Prevalence of the metabolic syndrome and its components in adult inhabitants of Krakow. Przegl Lek 63:733–737
Zuo H, Shi Z, Hu X, Wu M, Guo Z, Hussain A (2009) Prevalence of metabolic syndrome and factors associated with its components in Chinese adults. Metabolism 58:1102–1108
Vernarelli JA, Lambert JD (2013) Tea consumption is inversely associated with weight status and other markers for metabolic syndrome in US adults. Eur J Nutr 52:1039–1048
Chang CS, Chang YF, Liu PY, Chen CY, Tsai YS, Wu CH (2012) Smoking, habitual tea drinking and metabolic syndrome in elderly men living in rural community: the Tianliao old people (TOP) study 02. PLoS One 7:e38874
Hashizume C, Kishimoto Y, Kanahori S, Yamamoto T, Okuma K, Yamamoto K (2012) Improvement effect of resistant maltodextrin in humans with metabolic syndrome by continuous administration. J Nutr Sci Vitaminol (Tokyo) 58:423–430
Vieira Senger AE, Schwanke CH, Gomes I, Valle Gottlieb MG (2012) Effect of green tea (Camellia sinensis) consumption on the components of metabolic syndrome in elderly. J Nutr Health Aging 16:738–742
Kubota K, Sumi S, Tojo H, Sumi-Inoue Y, I-Chin H, Oi Y, Fujita H, Urata H (2011) Improvements of mean body mass index and body weight in preobese and overweight Japanese adults with black Chinese tea (Pu-Erh) water extract. Nutr Res 31:421–428
Tokunaga S, White IR, Frost C, Tanaka K, Kono S, Tokudome S, Akamatsu T, Moriyama T, Zakouji H (2002) Green tea consumption and serum lipids and lipoproteins in a population of healthy workers in Japan. Ann Epidemiol 12:157–165
Polychronopoulos E, Zeimbekis A, Kastorini CM, Papairakleous N, Vlachou I, Bountziouka V, Panagiotakos DB (2008) Effects of black and green tea consumption on blood glucose levels in non-obese elderly men and women from Mediterranean Islands (MEDIS epidemiological study). Eur J Nutr 47:10–16
Panagiotakos DB, Lionis C, Zeimbekis A, Gelastopoulou K, Papairakleous N, Das UN, Polychronopoulos E (2009) Long-term tea intake is associated with reduced prevalence of (type 2) diabetes mellitus among elderly people from Mediterranean islands: MEDIS epidemiological study. Yonsei Med J 50:31–38
Wu CH, Lu FH, Chang CS, Chang TC, Wang RH, Chang CJ (2003) Relationship among habitual tea consumption, percent body fat, and body fat distribution. Obes Res 11:1088–1095
Natella F, Scaccini C (2012) Role of coffee in modulation of diabetes risk. Nutr Rev 70:207–217
Bouchard DR, Ross R, Janssen I (2010) Coffee, tea and their additives: association with BMI and waist circumference. Obes Facts 3:345–352
Sae-tan S, Grove KA, Lambert JD (2011) Weight control and prevention of metabolic syndrome by green tea. Pharmacol Res 64:146–154
Suzuki Y, Miyoshi N, Isemura M (2012) Health-promoting effects of green tea. Proc Jpn Acad Ser B Phys Biol Sci 88:88–101
Higdon JV, Frei B (2006) Coffee and health: a review of recent human research. Crit Rev Food Sci Nutr 46:101–123
Grosso G, Stepaniak U, Topor-Mądry R, Szafraniec K, Pająk A (2014) Estimated dietary intake and major food sources of polyphenols in the Polish arm of the HAPIEE study. Nutrition 30:1398–1403
Buscemi S, Verga S, Batsis JA, Tranchina MR, Belmonte S, Mattina A, Re A, Rizzo R, Cerasola G (2009) Dose-dependent effects of decaffeinated coffee on endothelial function in healthy subjects. Eur J Clin Nutr 63:1200–1205
Buscemi S, Batsis JA, Arcoleo G, Verga S (2010) Coffee and endothelial function: a battle between caffeine and antioxidants? Eur J Clin Nutr 64:1242–1243
Andriantsitohaina R, Auger C, Chataigneau T, Etienne-Selloum N, Li H, Martinez MC, Schini-Kerth VB, Laher I (2012) Molecular mechanisms of the cardiovascular protective effects of polyphenols. Br J Nutr 108:1532–1549
Wu LY, Juan CC, Hwang LS, Hsu YP, Ho PH, Ho LT (2004) Green tea supplementation ameliorates insulin resistance and increases glucose transporter IV content in a fructose-fed rat model. Eur J Nutr 43:116–124
Imatoh T, Tanihara S, Miyazaki M, Momose Y, Uryu Y, Une H (2011) Coffee consumption but not green tea consumption is associated with adiponectin levels in Japanese males. Eur J Nutr 50:279–284
Westerterp-Plantenga M, Diepvens K, Joosen AM, Berube-Parent S, Tremblay A (2006) Metabolic effects of spices, teas, and caffeine. Physiol Behav 89:85–91
Acheson KJ, Gremaud G, Meirim I, Montigon F, Krebs Y, Fay LB, Gay LJ, Schneiter P, Schindler C, Tappy L (2004) Metabolic effects of caffeine in humans: lipid oxidation or futile cycling? Am J Clin Nutr 79:40–46
Buscemi S, Verga S, Batsis JA, Donatelli M, Tranchina MR, Belmonte S, Mattina A, Re A, Cerasola G (2010) Acute effects of coffee on endothelial function in healthy subjects. Eur J Clin Nutr 64:483–489
Acknowledgments
The study has been funded by the Wellcome Trust (Grants 064947/Z/01/Z and 081081/Z/06/Z), US National Institute on Ageing (Grant 1R01 AG23522-01) and the MacArthur Foundation Initiative on Social Upheaval and Health (award 71208). Giuseppe Grosso was supported by the International Ph.D. Program in Neuropharmacology, University Medical School of Catania, Catania, Italy.
Conflict of interest
The authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article

Cite this article
Grosso, G., Stepaniak, U., Micek, A. et al. Association of daily coffee and tea consumption and metabolic syndrome: results from the Polish arm of the HAPIEE study. Eur J Nutr 54, 1129–1137 (2015). https://doi.org/10.1007/s00394-014-0789-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-014-0789-6