
Abstract
Background
YouTube is an increasingly used platform for medical information. However, the validity of health-related information on psoriatic arthritis (PsA) on YouTube has not been determined.
Objective
The purpose of this study was to evaluate the accuracy and quality of YouTube videos concerning PsA.
Materials and methods
A YouTube search was performed on April 18, 2021, using the keyword “psoriatic arthritis.” Two independent raters accessed the content, source, and detailed characteristics of the included videos. The reliability and quality of the videos were analyzed using the modified DISCERN score, Journal of the American Medical Association benchmark criteria score, and global quality scale score.
Results
Of the 200 videos screened, 155 were included in the study after applying the exclusion criteria. A total of 132 (85.2%) videos revealed useful information about PsA, whereas the remaining 23 (14.8%) were misleading. Video interaction parameters including the median number of views, views per day, likes, dislikes, and comments demonstrated no significant difference between the two groups. The videos posted by universities and professional organizations displayed the highest reliability and quality scores.
Conclusion
The majority of YouTube videos on PsA contained useful information. However, physicians should alert patients to the possibility of misinformation and non-validated sources. Professional organizations in the field of rheumatology, such as the American College of Rheumatology and European League Against Rheumatism, should consider collaborating with YouTube to deliver high-quality content.
Zusammenfassung
Hintergrund
YouTube ist eine Plattform, die zunehmend für medizinische Informationen genutzt wird. Die Validität von gesundheitsbezogenen Informationen über Psoriasisarthritis auf YouTube wurde jedoch nicht nachgewiesen.
Ziel der Arbeit
Der Zweck dieser Studie war die Auswertung der Genauigkeit und Qualität von YouTube-Videos über Psoriasisarthritis.
Material und Methoden
Eine YouTube-Suche wurde am 18. April 2021 mit dem Stichwort „Psoriasisarthritis“ durchgeführt. Zwei unabhängige Prüfer griffen auf den Inhalt, die Quelle und die detaillierten Merkmale der einbezogenen Videos zu. Die Zuverlässigkeit und Qualität der Videos wurde anhand des modifizierten DISCERN-Score, des Journal of the American Medical Association Benchmark Criteria Score und des Global Quality Scale Score analysiert.
Ergebnisse
Von den 200 gescreenten Videos wurden nach Anwendung der Ausschlusskriterien 155 in die Studie aufgenommen. Insgesamt 132 (85,2 %) Videos enthielten nützliche Informationen über Psoriasisarthritis, während die restlichen 23 (14,8 %) irreführend waren. Die Parameter der Video-Interaktion, einschließlich der mittleren Anzahl der Aufrufe, der Aufrufe pro Tag, der Likes, der Dislikes und der Kommentare, zeigten keinen signifikanten Unterschied zwischen den beiden Gruppen. Die Videos, die von Universitäten und Berufsverbänden veröffentlicht wurden, wiesen die höchsten Werte für Zuverlässigkeit und Qualität auf.
Schlussfolgerung
Die meisten YouTube-Videos über Psoriasisarthritis enthielten nützliche Informationen. Dennoch müssen Ärzte ihre Patienten auf die Möglichkeit von Fehlinformationen und nichtvalidierten Quellen hinweisen. Professionelle Organisationen im Bereich der Rheumatologie wie das American College of Rheumatology und die European League Against Rheumatism sollten eine Zusammenarbeit mit YouTube in Betracht ziehen, um qualitativ hochwertige Inhalte zu liefern.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
PsA is a common systemic inflammatory disease included in the spondyloarthropathy spectrum, which involves both the peripheral joints and the axial skeleton [1, 2]. PsA usually develops in those with psoriasis, but in about 20% of patients, it precedes the onset of psoriasis [3]. Up to 30% of patients with psoriasis develop PsA at some time in their lives [4, 5]. Musculoskeletal manifestations vary from enthesitis to severe involvement of peripheral joints, called arthritis mutilans [3]. Going beyond joint and skin involvement and extra-articular manifestations, such as uveitis and inflammatory bowel disease, PsA is also associated with several comorbidities, including metabolic syndrome, obesity, and cardiovascular disease [2, 5]. Although PsA was initially considered as a relatively benign disorder, registry data suggest that the progressive and devastating character of the disease cause functional disability and impair quality of life [1, 4].
Seeking online health information has dramatically increased in recent years [6], with nearly 80% of internet users searching for medical information using online platforms [7]. Today, social media is widely used to share health-related information [8]. Especially patients with chronic diseases trust internet-based sources, and 75% are reported to base their disease-related decisions on information they have obtained from the internet [7]. YouTube is the most popular video-sharing website worldwide, receiving more than 1 billion hours of views every day, including 30 million medical videos [8, 9]. However, there have been concerns about the accuracy and quality of health-related information in YouTube videos due to the minimal regulation of the enormous volume of information [7, 10, 11].
Physicians should be aware of the quality of content presented on YouTube, given that patients are increasingly using this source and it affects their decision-making processes [12]. Previous studies have found varying accuracy and quality of YouTube content on rheumatic diseases such as rheumatoid arthritis [13], spondyloarthritis [14], systemic lupus erythematosus (SLE) [15], Sjögren’s syndrome [16], and fibromyalgia [17]. In addition, several studies have been performed to investigate the quality of information about psoriasis on YouTube [7, 18]. However, to our knowledge, there is no study that has analyzed the quality of YouTube videos pertaining to PsA. Therefore, the purpose of the current study was to analyze the quality of YouTube videos on PsA.
Materials and methods
Search procedure
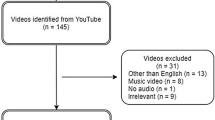
A YouTube search was performed on April 18, 2021, using the keyword “psoriatic arthritis.” The “incognito” mode of Google Chrome (Google Inc., CA, USA) was used for browsing YouTube. Browsing history was deleted prior to the search to prevent results from being influenced by previous online activity. YouTube’s default relevance mode was used to mimic most consumers’ search pattern. It is known that most viewers do not go beyond the first few pages of search results; therefore, the first 200 videos regarding PsA were listed, similar to previous studies [13, 17, 19]. The selected videos were saved in a playlist in YouTube Library for further analysis. Duplicates, videos that were not related to PsA, videos presented in a language other than English, those lasting more than 1 h, and music and advertisement videos were excluded from the study. After applying the exclusion criteria, the remaining 155 videos were included in the study (Fig. 1).

Flowchart demonstrating video selection
Data review
Viewer engagement parameters, including the number of views, likes, dislikes, and comments were documented by the authors. The remaining characteristics of the videos, namely upload date, video length, target audience, and video source were also noted. Since the upload date and online duration of the videos varied, the number of views per day was calculated for a strong analysis. The content of the videos (epidemiology, pathogenesis, clinical characteristics, diagnosis, and treatment) was also recorded. Two rheumatologists (MEO and OZ) blindly analyzed each video. Any discrepancy between the raters was resolved by reevaluation and consensus.
Video source and targeted audience
The video sources were grouped into five categories as universities and professional organizations, physicians, health information websites, TV programs, and independent users. The primary target audience of the videos was classified as healthcare professionals and patients.
Usefulness
The videos were deemed useful if the information they contained was completely scientifically accurate, and misleading if they contained any inaccurate information regarding any aspect of PsA, in accordance with the guidelines of professional organizations in the field of rheumatology such as the American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR). Previous studies have followed the same path [13, 20].
Video popularity
To evaluate video popularity, the video power index (VPI) was calculated using a formula including the like ratio [(likes × 100) / (likes + dislikes)] and view ratio (views per day): VPI = [(like ratio * view ratio) / 100] [21,22,23].
Quality and reliability evaluation
The Global Quality Scale (GQS), which was first developed by Bernard et al. [24], was used to evaluate the quality of the videos. This is a five-point scale in which higher scores indicate greater quality. The Journal of the American Medical Association (JAMA) benchmark criteria to determine authorship, attribution, disclosure, and currency were also used to assess quality. Each of these criteria was rated with 1 point, with the maximum score being 4 points. Lastly, a five-point modified DISCERN score was obtained to evaluate reliability. Each question in this instrument is scored 1 point, giving a maximum score of 5 points, and higher scores indicate better reliability. Several studies on YouTube videos have used GQS [13, 22], JAMA [17, 25], and modified DISCERN [14, 15] for similar purposes. Questions of the GQS [22], JAMA [25], and modified DISCERN [15] tools are shown in Table 1.
Statistical analyses
The normality of data was examined using the Shapiro–Wilk test. Continuous variables were stated as median and interquartile range, while categorical variables were presented as counts and percentages. The Mann–Whitney U-test was carried out for two groups and the Kruskal–Wallis test for more than two groups to compare non-normally distributed data. The Mann–Whitney U-test was also used for pairwise comparisons following the Kruskal–Wallis test to determine the groups that led to significant differences. Correction for the p-value was done automatically by SPSS (IBM SPSS Statistics for Windows; IBM Corp, Armonk, NY, USA). Fischer’s exact test was used for categorical variables to assess the differences between the two groups. Inter-rater agreement was evaluated using Cohen’s kappa coefficient. A p-value of < 0.05 was set as significant. SPSS version 22 was used for all statistical analyses.
Results
Of the total 200 videos screened, 155 met the inclusion criteria and were included in the study. For the 155 videos analyzed, the total number of days on YouTube was 163,517, the total video duration was 23.16 h, and the total view count was 794,999. The first video was uploaded on March 30, 2011, and the last on March 26, 2021. The number of uploaded videos generally increased over the years. More than half of the videos (52%) were uploaded within the last 3 years. While 2019 represented the year with the most video uploads, there was a partial decrease in 2020 (Fig. 2). Cohen’s kappa coefficient for inter-rater agreement was 0.783 for the DISCERN score, indicating a substantial agreement, and 0.862 and 0.824 for the JAMA and GQS scores, respectively, indicating near-perfect agreement for both.

Distribution of the analyzed videos over the years. Note: samples for 2021 only gathered until March 2021
Target audience and video content
Of the total 155 videos, 74.8% targeted patients and 25.2% targeted healthcare professionals. Since more than one topic was mentioned in 53 videos, each topic was recorded separately. Over 60% of the videos contained information about the treatment of PsA, followed by clinical features (n = 89, 56.8%), diagnosis (n = 37, 23.9%), pathogenesis (n = 24, 15.5%), and epidemiology (n = 24, 15.5%).
General characteristics of the videos
For the 155 videos analyzed, the median view count was 1047 (range 271–4213), the number of views per day was 1.80 (range 0.49–5.67), and the number of likes was 10 (range 2–49). The median duration of the videos was 5.00 (range 2.22–9.12) minutes. The median VPI was 1.66 (range 0.49–5.44). The median reliability score measured with the modified DISCERN was 3 (range 2–4). Concerning quality, the median score was 3 (range 2–3) for JAMA and 4 (range 2–4) for GQS. Baseline characteristics of the analyzed videos were demonstrated in Table 2.
Assessment of usefulness
Of the total 155 videos evaluated, 132 (85.2%) were categorized as useful, while 23 (14.8%) contained misleading information. There was no significant difference detected between the two groups in terms of the median number of days on YouTube. Video metrics, including the median number of views, views per day, likes, dislikes, and comments did not significantly differ between the two groups (p = 0.926, p = 0.594, p = 0.367, p = 0.373, and p = 0.189, respectively). The median length was significantly higher in the useful videos than in the misleading ones (p = 0.028). The VPI score, reflecting the popularity of the videos, showed no significant difference between the useful and misleading video groups (p = 0.587). The modified DISCERN, JAMA, and GQS scores were significantly higher in the useful videos, indicating better reliability and quality. Independent users constituted the source that posted the highest percentage of misleading videos (6/10, 60%). In contrast, all the videos uploaded by universities and professional organizations were determined to be useful. Independent users were the source that contributed only 3% of useful videos, whereas they uploaded 26% of misleading videos. The majority of videos were related to treatment in the useful group (65.2%) and clinical signs in the misleading group (56.5%). In terms of the target audience, all of the misleading videos were aimed at patients. Of the total 19 videos regarding patients’ personal experience, five (26.3%) contained misleading information (Table 3).
We also conducted an extra analysis to assess how the top 10 high-performer videos (in regard to the number of views) were separated into useful and misleading, and detected one misleading video (10%). In addition, we compared the top 10 high-performer videos with the remaining 145 videos and detected no significant difference concerning the number of useful and misleading videos between the two groups (p = 0.546), suggesting that the videos with a high view count may not serve as a guide for viewers to distinguish between useful and misleading videos.
Evaluation of reliability, quality, and popularity according to video source
In view of reliability and quality, the median DISCERN, JAMA, and GQS scores revealed a statistically significant difference between the video sources (p < 0.001 for all). The videos posted by universities and professional organizations had the highest median scores concerning the modified DISCERN (5, range 4–5), JAMA (4, range 3–4), and GQS (5, range 4.25–5), followed by physicians (4, range 3–4; 3, range 2–3; and 4, range 3–5, respectively). As expected, the videos uploaded by universities and professional organizations had significantly higher reliability and quality scores compared to all the remaining sources. The median DISCERN score of the videos uploaded by universities and professional organizations was significantly higher than those of the videos posted by physicians, health information websites, TV programs, and independent users (p = 0.024, p < 0.001, p < 0.001, and p < 0.001, respectively). The median JAMA and GQS score of the videos posted by universities and professional organizations were also higher compared to those uploaded by physicians (p = 0.010 and 0.034, respectively) and the remaining sources (p < 0.001 for all). The videos provided by independent users displayed the lowest reliability and quality scores. The VPI scores, assessing popularity, did not significantly differ between the upload sources (Table 4).
Discussion
In recent years, social media has become a trendy source of medical information [26]. Especially patients with chronic conditions increasingly trust online healthcare information sources [10], and most patients diagnosed with a rheumatic disease seek online medical information to manage their diseases [27].
The database obtained in the current study included 155 videos with approximately 1 million total views and a total duration of 23.16 h, suggesting that YouTube is commonly utilized when seeking medical information regarding PsA. In view of video metrics, a cumulative number of 9901 likes, 448 dislikes, and 1185 comments was recorded. Compared to the number of views, the rate of video interaction parameters (likes + dislikes + comments) was quite low (1.15%) in the current study. This ratio was 1.24% in a study performed by Elangovan et al. [14] on SLE, and 0.98% in another study performed by Kumar et al. [28] on hypertension, similar to our study. These results suggest that viewers mostly prefer just to watch passively and hardly interact with the platform. The videos covered a wide variety of issues related to PsA, mainly focusing on the clinical signs and treatment of the disease.
While information on online platforms is sometimes useful, it is not always appropriate [28]. In our study, 132 (85.2%) contained scientifically accurate information and were categorized as useful, whereas 23 (14.8%) contained misleading information. Previous studies investigating YouTube as a source of health-related information on several diseases have reported various results regarding misleading information. Mueller et al. [7] reported misinformation 63% on psoriasis, Kumar et al. [29] 33% on hypertension, and Pathak et al. [30] 26% on Ebola virus disease. Considering rheumatic diseases, Singh et al. [13] determined that 30% of videos contained misleading information on rheumatoid arthritis, while Ng et al. [15] reported it to be 16% for SLE and Elongovan et al. [14] 14% for spondyloarthritis, similar to our study. Spread of misinformation may result in patients following inappropriate medical advice or experiencing excessive anxiety [28]. On January 26, 2021, a letter from YouTube CEO, Susan Wojcicki, stated that more than 500,000 videos containing misinformation associated with COVID-19 were removed from the platform according to their new health policies [31]. YouTube should also consider expanding this misinformation policy to other health topics, including rheumatology.
In this study, as expected, the reliability and quality of the useful videos were much better than those of the misleading videos, which is in agreement with previous studies [15, 32]. The duration of the useful videos was significantly longer, as also determined by Moon et al. for COVID-19 videos on YouTube [33]. This may be because useful videos are presented from a more comprehensive and detailed perspective, resulting in a longer duration. Video interaction parameters, including likes, dislikes, and comments showed no significant difference between the useful and misleading videos. In addition, the useful and misleading videos did not significantly differ in popularity, similar to the results of previous research [13, 33]. The literature contains conflicting results concerning whether interaction parameters are similar between useful and misleading videos [13, 16]. While some authors reported higher interaction scores for useful videos [33], others indicated higher values for misleading videos [19]. As video interaction parameters are poor determinants of accuracy and usefulness, they should not be used as a guide to assess usefulness. During consultations, physicians should consider directing patients to reliable sources of online medical information rather than relying on video metrics.
In the current study, it was observed that the majority of the videos had been uploaded by health information websites (45.8%), followed by physicians (27.1%) and universities and professional organizations (12.9%). In view of reliability and quality, universities and professional organizations had higher modified DISCERN and JAMA scores, which significantly differed as compared to the other upload sources, except physicians. However, the relatively lower number of videos posted by universities and professional organizations was noteworthy. This analysis suggests that universities and professional organizations should increase the number of videos they produce. In addition, the videos with the lowest reliability and quality scores had been mostly posted by independent users, which is in agreement with the studies of Li et al. [32] and Khatri et al. [20]. We suggest that YouTube content creators use validating scoring systems to make better-quality and unbiased videos.
It is essential for viewers to access credible, evidence-based accurate information provided by trusted sources. Recently, YouTube has announced that they have established a team under the leadership of Garth Graham (who has worked as a cardiologist and as a researcher educating people about public health over the past 20 years, and as Deputy Assistant Secretary at the U.S. Department of Health and Human Services prior to joining YouTube) to make high-quality health content available for viewers in collaboration with some of the most respected organizations and clinicians. They have also initiated novel collaborations with organizations such as the American Public Health Association, the Mayo Clinic, and the Cleveland Clinic, and expressed their willingness to establish new health partnerships to help offer trustworthy medical information on YouTube [34]. Professional organizations, especially ACR and EULAR, should consider participating in this collaboration in order to deliver better-quality videos in the field of rheumatology to the target audience.
Conclusion
The results of our study demonstrated that the majority of the YouTube videos contained useful information regarding PsA. Given patients’ limited consultation time with their physicians, YouTube can be recommended as a complementary source to receive additional information on PsA. However, rheumatologists should warn their patients about the possibility of misinformation and refer them to trusted sources available on YouTube. We recommend universities and professional organizations to share more videos on rheumatic diseases on this platform. Considering that YouTube has begun to make partnerships with reputable healthcare organizations to create high-quality health content, professional rheumatology organizations, such as ACR and EULAR, should also consider collaborating with YouTube for this purpose.
References
Coates LC, Helliwell PS (2017) Psoriatic arthritis: state of the art review. Clin Med (Lond) 17(1):65–70. https://doi.org/10.7861/clinmedicine.17-1-65
Veale DJ, Fearon U (2018) The pathogenesis of psoriatic arthritis. Lancet 391(10136):2273–2284. https://doi.org/10.1016/S0140-6736(18)30830-4
Rida MA, Chandran V (2020) Challenges in the clinical diagnosis of psoriatic arthritis. Clin Immunol 214:108390. https://doi.org/10.1016/j.clim.2020.108390
Ritchlin CT, Colbert RA, Gladman DD (2017) Psoriatic arthritis. N Engl J Med 376(10):957–970. https://doi.org/10.1056/NEJMra1505557
Ogdie A, Coates LC, Gladman DD (2020) Treatment guidelines in psoriatic arthritis. Rheumatology (Oxford) 59(Suppl 1):i37–i46. https://doi.org/10.1093/rheumatology/kez383
Diviani N, van den Putte B, Giani S, van Weert JC (2015) Low health literacy and evaluation of online health information: a systematic review of the literature. J Med Internet Res 17(5):e112. https://doi.org/10.2196/jmir.4018
Mueller SM, Jungo P, Cajacob L, Schwegler S, Itin P, Brandt O (2019) The absence of evidence is evidence of non-sense: cross-sectional study on the quality of psoriasis-related videos on YouTube and their reception by health seekers. J Med Internet Res 21(1):e11935. https://doi.org/10.2196/11935
Haslam K, Doucette H, Hachey S, MacCallum T, Zwicker D, Smith-Brilliant M, Gilbert R (2019) YouTube videos as health decision aids for the public: an integrative review. Can J Dent Hyg 53(1):53–66
YouTube Official Blog (2021) YouTube for press. https://blog.youtube/press. Accessed 7 May 2021
Madathil KC, Rivera-Rodriguez AJ, Greenstein JS, Gramopadhye AK (2015) Healthcare information on YouTube: a systematic review. Health Informatics J 21(3):173–194. https://doi.org/10.1177/1460458213512220
Meldrum S, Savarimuthu BT, Licorish S, Tahir A, Bosu M, Jayakaran P (2017) Is knee pain information on YouTube videos perceived to be helpful? An analysis of user comments and implications for dissemination on social media. Digit Health 3:2055207617698908. https://doi.org/10.1177/2055207617698908
Wong M, Desai B, Bautista M, Kwon O, Kolodychuk N, Chimento G (2018) YouTube is a poor source of patient information for knee arthroplasty and knee osteoarthritis. Arthroplast Today 5(1):78–82. https://doi.org/10.1016/j.artd.2018.09.010
Singh AG, Singh S, Singh PP (2012) YouTube for information on rheumatoid arthritis—a wakeup call? J Rheumatol 39(5):899–903. https://doi.org/10.3899/jrheum.111114
Elangovan S, Kwan YH, Fong W (2021) The usefulness and validity of English-language videos on YouTube as an educational resource for spondyloarthritis. Clin Rheumatol 40(4):1567–1573. https://doi.org/10.1007/s10067-020-05377-w
Ng CH, Lim GRS, Fong W (2020) Quality of English-language videos on YouTube as a source of information on systemic lupus erythematosus. Int J Rheum Dis 23(12):1636–1644. https://doi.org/10.1111/1756-185X.13852
Delli K, Livas C, Vissink A, Spijkervet FK (2016) Is YouTube useful as a source of information for Sjögren’s syndrome? Oral Dis 22(3):196–201. https://doi.org/10.1111/odi.12404
Ozsoy-Unubol T, Alanbay-Yagci E (2020) YouTube as a source of information on fibromyalgia. Int J Rheum Dis 24(2):197–202. https://doi.org/10.1111/1756-185X.14043
Qi J, Trang T, Doong J, Kang S, Chien AL (2016) Misinformation is prevalent in psoriasis-related YouTube videos. Dermatol Online J 22(11):5. https://doi.org/10.5070/D32211033142
Garg N, Venkatraman A, Pandey A, Kumar N (2015) YouTube as a source of information on dialysis: a content analysis. Nephrology (Carlton) 20(5):315–320. https://doi.org/10.1111/nep.12397
Khatri P, Singh SR, Belani NK, Yeong YL, Lohan R, Lim YW, Teo WZ (2020) YouTube as source of information on 2019 novel coronavirus outbreak: a cross sectional study of English and Mandarin content. Travel Med Infect Dis 35:101636. https://doi.org/10.1016/j.tmaid.2020.101636
Erdem MN, Karaca S (2018) Evaluating the accuracy and quality of the information in kyphosis videos shared on YouTube. Spine 43(22):E1334–E1339. https://doi.org/10.1097/BRS.0000000000002691
Starks C, Akkera M, Shalaby M, Munshi R, Toraih E, Lee GS, Kandil E, Shama MA (2021) Evaluation of YouTube videos as a patient education source for novel surgical techniques in thyroid surgery. Gland Surg 10(2):697–705. https://doi.org/10.21037/gs-20-734
Wu V, Lee DJ, Vescan A, Lee JM (2020) Evaluating YouTube as a source of patient information for functional endoscopic sinus surgery. Ear Nose Throat J. https://doi.org/10.1177/0145561320962867
Bernard A, Langille M, Hughes S, Rose C, Leddin D, Veldhuyzen van Zanten S (2007) A systematic review of patient inflammatory bowel disease information resources on the World Wide Web. Am J Gastroenterol 102(9):2070–2077. https://doi.org/10.1111/j.1572-0241.2007.01325.x
Zhang S, Fukunaga T, Oka S, Orita H, Kaji S, Yube Y, Yamauchi S, Kohira Y, Egawa H (2020) Concerns of quality, utility, and reliability of laparoscopic gastrectomy for gastric cancer in public video sharing platform. Ann Transl Med 8(5):196. https://doi.org/10.21037/atm.2020.01.78
Hongler VNS, Navarini A, Brandt O, Goldust M, Mueller SM (2020) Global trends in YouTube and Google search activity for psoriasis and atopic eczema: detecting geographic hot spots, blind spots and treatment strategies. Dermatol Ther 33(4):e13510. https://doi.org/10.1111/dth.13510
Hay MC, Cadigan RJ, Khanna D, Strathmann C, Lieber E, Altman R, McMahon M, Kokhab M, Furst DE (2008) Prepared patients: internet information seeking by new rheumatology patients. Arthritis Rheum 59(4):575–582. https://doi.org/10.1002/art.23533
Kumar N, Pandey A, Venkatraman A, Garg N (2014) Are video sharing web sites a useful source of information on hypertension? J Am Soc Hypertens 8(7):481–490. https://doi.org/10.1016/j.jash.2014.05.001
Pathak R, Poudel DR, Karmacharya P, Pathak A, Aryal MR, Mahmood M, Donato AA (2015) YouTube as a source of information on ebola virus disease. N Am J Med Sci 7(7):306–309. https://doi.org/10.4103/1947-2714.161244
Jo W, Lee J, Park J, Kim Y (2020) Online information exchange and anxiety spread in the early stage of the novel coronavirus (COVID-19) outbreak in South Korea: structural topic model and network analysis. J Med Internet Res 22(6):e19455. https://doi.org/10.2196/19455
Wojcicki S (2021) Letter from Susan: our 2021 priorities. https://blog.youtube/inside-youtube/letter-from-susan-our-2021-priorities/. Accessed 22 May 2021
Li HO, Bailey A, Huynh D, Chan J (2020) YouTube as a source of information on COVID-19: a pandemic of misinformation? BMJ Glob Health 5(5):e2604. https://doi.org/10.1136/bmjgh-2020-002604
Moon H, Lee GH (2020) Evaluation of Korean-language COVID-19-related medical information on YouTube: cross-sectional infodemiology study. J Med Internet Res 22(8):e20775. https://doi.org/10.2196/20775
Graham G (2021) New health content is coming to YouTube. https://blog.youtube/news-and-events/new-health-content-coming-youtube/. Accessed 22 May 2021
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M. E. Onder and O. Zengin declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies performed were in accordance with the ethical standards indicated in each case.
Additional information
Redaktion
Ulf Müller-Ladner, Bad Nauheim
Uwe Lange, Bad Nauheim
Availability of data and material
The authors confirm that the data supporting the findings of this study are available within the article.

Scan QR code & read article online
Rights and permissions
About this article

Cite this article
Onder, M.E., Zengin, O. Quality of healthcare information on YouTube: psoriatic arthritis. Z Rheumatol 82 (Suppl 1), 30–37 (2023). https://doi.org/10.1007/s00393-021-01069-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00393-021-01069-1