
Abstract
Background
In Europe, more than 300,000 persons per year experience out-of-hospital cardiac arrest (OHCA). Despite medical progress, only few patients survive with good neurological outcome. For many issues, evidence from randomized trials is scarce. OHCA often occurs for cardiac causes. Therefore, we established the national, prospective, multicentre German Cardiac Arrest Registry (G-CAR). Herein, we describe the first results of the pilot phase.
Results
Over a period of 16 months, 15 centres included 559 consecutive OHCA patients aged ≥ 18 years. The median age of the patients was 66 years (interquartile range 57;75). Layperson resuscitation was performed in 60.5% of all OHCA cases which were not observed by emergency medical services. The initial rhythm was shockable in 46.4%, and 29.1% of patients had ongoing CPR on hospital admission. Main presumed causes of OHCA were acute coronary syndromes (ACS) and/or cardiogenic shock in 54.8%, with ST-elevation myocardial infarction being the most common aetiology (34.6%). In total, 62.9% of the patients underwent coronary angiography; percutaneous coronary intervention (PCI) was performed in 61.4%. Targeted temperature management was performed in 44.5%. Overall in-hospital mortality was 70.5%, with anoxic brain damage being the main presumed cause of death (38.8%). Extracorporeal cardiopulmonary resuscitation (eCPR) was performed in 11.0%. In these patients, the in-hospital mortality rate was 85.2%.
Conclusions
G-CAR is a multicentre German registry for adult OHCA patients with a focus on cardiac and interventional treatment aspects. The results of the 16-month pilot phase are shown herein. In parallel with further analyses, scaling up of G-CAR to a national level is envisaged.
Trial registration
ClinicalTrials.gov identifier: NCT05142124.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In Europe, more than 300,000 patients suffer from out-of-hospital cardiac arrest (OHCA) every year [1]. Despite medical progress leading to a trend towards decreased mortality rates of OHCA patients [2, 3], reported survival rates with good neurological outcome remain low, ranging from 2 to 10% [4,5,6]. Therefore, optimization of medical care of these patients is necessary. However, adequate evidence from randomized trials is scarce and clinical practice differs widely between centres. Against this background, a systematic and standardized registration of the treatment course and of the clinical outcomes of OHCA patients in a “real-world setting” is essential and has become a prerequisite for the certification of cardiac arrest centres in Germany [7]. Despite the fact that cardiac pathologies are the underlying cause in the majority of OHCA cases [8], a national registry including long-term and patient-reported outcomes, such as health-related quality of life, psychopathological symptoms (i.e. cognitive impairment, depression, anxiety, or post-traumatic stress disorder) and return to normal life under the guidance of cardiologists has not been published so far concerning the German population. As previously described in more detail [9], we established G-CAR (German Cardiac Arrest Registry) with the aim to achieve a better understanding of the acute and long-term consequences of OHCA and to optimize processes during treatment and follow-up of OHCA patients. Herein, we report the results of the pilot phase of this new registry with a special focus on interventional aspects, such as treatment of coronary artery disease and extracorporeal cardiopulmonary resuscitation (eCPR).
Methods
Design and overview
G-CAR (NCT05142124) is a prospective, multicentre registry of patients with OHCA in Germany. The design of the trial was published previously [9]. In total, 15 centres agreed to participate in the pilot phase and to provide data on their patients by filling out the electronic case report form. The registry collects information regarding the (i) pre-hospital phase; (ii) in-hospital phase including interventional therapy, treatment on the intensive care unit (ICU), and eCPR; and (iii) post-hospital (rehabilitation) phase. The collected information is stored at the Institut für Herzinfarktforschung in Ludwigshafen, Germany.
Patients and follow-up
Patients ≥ 18 years with OHCA were eligible for inclusion. The only exclusion criterion was rejection of participation by either the patient or the legal representative. Patients were treated according to the local standards of the participating centres. Clinical and neurological outcomes were and will be assessed after 30 days, 6 months, and 1 year. The evaluation after 30 days is performed either by a personal interview if the patient is still hospitalized or by a structured telephone interview by qualified staff. After 6 and 12 months, patient-reported outcomes such as health-related quality of life, psychopathological symptoms (cognitive impairment, affective disorders, post-traumatic stress disorder), and social reintegration are assessed by standardized questionnaires and by a telephone interview using standardized questionnaires.
Informed consent
Due to their clinical status, some patients were unable to give consent on admission to the hospital. Patients who were able to give consent during the hospital stay were asked to do so as soon as possible. If patients were unable to give informed consent during the hospital stay, her/his consent was sought from their legal representative. Data of patients who died before regaining their capacity to consent and before a legal representative was appointed were anonymized and included in the registry. This informed consent process has been validated and approved by the ethical committees in all federal counties of the recruiting study centres in Germany.
Results
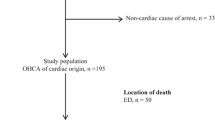
A total of 559 consecutive adult OHCA patients were included in 15 tertiary care hospitals between 07/2021 and 03/2023. Out of the 15 centres involved in the pilot phase, 13 (86.7%) are certified cardiac arrest centres. The baseline characteristics of the patients are depicted in Table 1. The median age of the patients was 66 years (interquartile range [IQR] 57;75), and 73.7% were male. The medical history of the patients encompasses the classical comorbidities, such as a history of myocardial infarction (17.0%), peripheral artery disease (9.6%), and chronic kidney disease (12.0%). Figure 1 depicts a flow diagram of the included patients.

Flow diagram of study patients. OHCA, out-of-hospital cardiac arrest; ROSC, return of spontaneous circulation; (e)CPR, (extracorporeal) cardiopulmonary resuscitation. Due to missing information about the different variables, the total number of patients differs within the figure
Pre-hospital phase
Mostly, OHCA occurred in private homes (52.2%), followed by public spaces in around one-third of cases (32.5%). Less frequently, patients suffered OHCA in medical facilities (6.3%), nursing homes (5.3%), or workspaces (3.7%). OHCA was unwitnessed in 22.1%, witnessed by laypersons in 59.3%, and by emergency medical services (EMS) in 18.6%. CPR was dispatcher-assisted in 11.5%; automatic external defibrillators (AED) were used in 7.2%, and a first-responder App in 0.7% of cases. Layperson resuscitation was performed in 60.5% of all OHCA cases which were not observed by EMS. The initial rhythm was shockable in 46.4%, non-shockable in 46.0%, and not documented in 7.6% (Table 2).
In-hospital phase
The majority of patients (64.1%) were admitted to a shock room or an emergency department, 24.3% were directly transferred to the catheterization laboratory, and 11.6% were admitted to an ICU. In total, 29.1% of the patients had ongoing CPR on hospital admission (Table 2).
Main presumed underlying causes of OHCA were acute coronary syndromes (ACS) and/or cardiogenic shock (CS) in more than half (54.8%) of the patients. ST-elevation myocardial infarction was observed in more than one-third (34.6%) of the cases. Primary arrhythmia without suspected ischemia was reported in 14.3%. Overall, the presumed cause for OHCA was cardiac in 69.1%. Non-cardiac causes included pulmonary embolism in 5.2%, and other non-cardiac causes (i.e. intoxication, hypoxia, hypovolemia, hypo-/hyperkalaemia, hypothermia, pneumothorax, and neurological causes) in 16.1% (Fig. 2).

Presumed aetiologies of OHCA
Coronary angiography (CAG)
Figure 3 A–C depicts the relevant findings regarding coronary angiography. In total, 62.9% of the patients underwent CAG. In three-quarters (75.0%) of these patients, CAG was performed immediately, and in 20.9% within 24 h. The remaining patients underwent elective CAG. Out of all patients undergoing CAG, 61.2% received percutaneous coronary intervention (PCI). Figure 4 depicts the rate and timing of CAG according to the presumed underlying cause of OHCA (STEMI (A), cardiogenic shock (B), and all other aetiologies [including NSTEMI, excluding STEMI and CS] (C)). More than two-thirds (67.2%) of the procedures were performed via femoral access. Culprit-only PCI was performed in 72.6% of cases, while immediate multivessel PCI was performed in 27.4%

Coronary angiography data: A timing of coronary angiography, B access, C strategy (PCI, percutaneous coronary intervention)

Rate and timing of coronary angiography according to the presumed underlying cause of OHCA: A STEMI, B cardiogenic shock, C all other aetiologies (including NSTEMI, excluding STEMI and cardiogenic shock) (NSTEMI, non-ST-elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction). Note: A Only 167/169 patients with available information on timing of coronary angiography and PCI. C Only 138/141 patients with available information on timing of coronary angiography and PCI
Targeted temperature management (TTM)
Targeted temperature management was performed in 44.5% (Table 3). Among those patients, therapeutic hypothermia was performed in 87.0% with a mean target temperature of 35.0 °C and a mean duration of 24 h. In 42.8%, TTM was applied invasively (i.e. intravascular catheter), in 49.0% non-invasively, and in 8.2% via an extracorporeal life support (ECLS) system. Active fever prevention was performed in 69.3% over a period of 72 h.
eCPR
Relevant data regarding eCPR are depicted in Fig. 5A–C. eCPR was performed in 11.0% of the patients. Implantation of an ECLS system was mostly performed in the catheterization laboratory (84.6%), followed by the ICU (9.6%) and the emergency department (5.8%) (Fig. 5A). Coronary angiography was performed in 82%, and PCI in 59.2%. Most ECLS systems were implanted before PCI (71.2%), 13.5% during PCI, and 15.4% after PCI (Fig. 5B). Cannulation was performed percutaneously in 98.1%. In most of the cases (83.0%), the care-taking ICU had a cardiology specialisation, followed by anaesthesiology (7.5%), interdisciplinary (1.9%), or surgical (1.9%) ICUs (Fig. 5C). Complications of eCPR are depicted in Table 4. Bleeding complications occurred in one-third (33.3%) of patients and were mainly located at the access site. Limb ischemia was observed in 9.8%, and ischemic stroke in 2.0% of cases.

eCPR: A location of implantation, B timing of implantation, C care-taking ICU (eCPR, (extracorporeal) cardiopulmonary resuscitation; ICU, intensive care unit)
Outcomes
Overall, the in-hospital mortality rate was 70.5% with anoxic brain damage representing the leading cause of death (38.8%), followed by circulatory (30.6%) and multiorgan failure (11.6%) (Table 5). In more than half of the patients (54.9%), in-hospital treatment was terminated prematurely. Main reasons for termination were the occurrence of anoxic brain damage (32.9%) and presumed patient will (28.2%) (Table 5). In-hospital mortality of eCPR patients was 85.2%.
Discussion
Herein, we present the results of the 16-month pilot phase of G-CAR including 559 patients and covering the pre-hospital and in-hospital phases with a focus on interventional aspects, including data on coronary angiography and eCPR.
Baseline data and pre-hospital phase
All 15 participating centres are tertiary care hospitals. The reported mean age of 66.0 years is comparable to the results of the European EuReCa TWO study (67.6 years) and slightly lower compared to the 2022 report of the German Resuscitation Registry (GRR; 70.2 years) [5]. The predominance of male sex has also been reported in the other two registries. As shown in these data, most OHCA cases occurred at home.
The rate of witnessed OHCA was higher in our cohort than in the GRR (77.9% vs. 56.3%, respectively). Correspondingly, the rate of a shockable initial rhythm was much higher (46.4% vs. 19.8%), and the rate of layperson CPR was higher (60.5% vs. 51.3%). Most likely, this is explained by the fact that the centres involved in G-CAR are mostly cardiac arrest centres with a focus on cardiological patients. Furthermore, most centres are located in urban areas with a high population density and a high number of potential bystanders. The higher rate of underlying cardiac causes in G-CAR compared to the GRR (69.1% vs. 57.9%, respectively) and the high rate (54.8%) of patients presenting with an ACS or with CS as presumed underlying aetiology in G-CAR might explain this difference. Unfortunately, the GRR does not further classify cardiac causes, making a direct comparison of the incidence of ACS as underlying cause impossible [10].
The rate of dispatcher-assisted CPR was lower in our registry compared to the GRR (11.5% vs. 30.8%, respectively). The reasons for this are unclear and might be partly due to a reporting-bias. Clearly, the dispatcher-assisted CPR in Germany needs to be further developed [11]. The reported rate of AED use was higher in our cohort compared to the GRR (7.2% vs. 1.5%, respectively). Notably, a first-responder App was used in only 0.7% of the cases. Compared with other countries, e.g. Denmark [12, 13], this is extremely low and needs to be improved.
Coronary angiography
No detailed information on the timing of CAG and the strategy of PCI have been published recently for the German population. Early revascularisation by PCI is the guideline-based approach in patients with STEMI [14]. However, most OHCA patients show non-specific ECG changes after return of spontaneous circulation (ROSC). In these patients, the decision regarding the indication and timing of coronary angiography is more complex. The Angiography After Out-of-Hospital Cardiac Arrest Without ST-Segment Elevation (TOMAHAWK) [15] and the Coronary Angiography after Cardiac Arrest (COACT) trials [16] are the two available large-scale randomized multicentre trials comparing immediate versus delayed CAG in successfully resuscitated OHCA patients without ST-elevations on the ECG. Both, together with smaller randomized trials, showed no significant differences in clinical outcomes between the two strategies [15,16,17].
In our cohort, CAG was performed in 62.9% of patients. Immediate CAG was performed in three-quarters of patients. As only one-third of patients presented with ST-elevations after ROSC, this percentage seems rather high in the light of neutral trials in patients without ST-elevation. In total, 61.0% of patients undergoing CAG underwent PCI, corroborating the results of previous publications that coronary artery disease is the underlying problem in a relevant proportion of the patients. The high rate of culprit-only PCI (72.6%) might reflect the results of the CULPRIT-SHOCK trial, which showed a lower rate of death and severe renal failure in patients with infarct-related cardiogenic shock and multivessel disease who initially underwent culprit-only PCI compared with those who underwent immediate multivessel PCI [18]. Notably, despite the recommendation of current guidelines to use the radial access as the default strategy [19, 20], more than two-thirds of the procedures were performed via femoral access. According to the annual report of the GRR 2022, CAG was performed in 26.9%, which is much lower than in our cohort. Most likely, this is again explained by the selection of the centres. The GRR report does not provide detailed data on the timing of CAG, the rates, and the strategy of PCI [10].
Targeted temperature management (TTM)
The optimal implementation of TTM and its influence on the neurological outcome are still controversially discussed. In 2021, the guideline of the European Resuscitation Council (ERC) recommended therapeutic hypothermia (TH) for all comatose patients after ROSC [16]. However, recent published data shows no significant difference in mortality or functional outcomes between TH with a target temperature of 33.0 °C and normothermia with fever prevention (≤ 37.7 °C) in adult OHCA patients with persistent coma after ROSC [21]. In 2022, the ERC guideline downgraded its recommendation for TH but recommended active fever prevention for at least 72 h [17]. The ESC 2023 ACS guidelines recommend continuous monitoring of core temperature and active fever prevention in OHCA patients with persistent coma, but do not give a statement on TH [15]. However, the before-mentioned recent data cannot be generalized for Germany because of various differences in patient characteristics (e.g. longer no-flow times, lower percentage of shockable rhythms, and lower bystander resuscitation rates in Germany) [22]. Furthermore, according to the most recent Cochrane systematic review and meta-analysis including all randomized controlled trials on TTM following OHCA, TH in the range of 32–34 °C as compared to normothermia or no temperature control was associated with improved neurologic outcomes after cardiac arrest [23]. This resulted in respective statements of national and international societies [24, 25]. The inconsistency of the data and the guideline recommendations is reflected in our data: TTM was performed in 44.5%. TH was applied in almost 87.0% of these patients, most likely because of the recommendations of the German national societies. Notably, there was a substantial variance in the mode of TTM application, i.e. invasive (device-based) vs. non-invasive. The rate of fever prevention (69.3%) was lower than could be expected due to the recommendations and in view of the fact that 87.4% of the patients were ventilated at admission. Most likely, this is due to an underreporting, since upon request, almost all recruiting centres stated to have a protocol for fever prevention.
eCPR
The poor results of conventional CPR and the increased availability of percutaneously implantable mechanical circulatory support systems (ECLS, extracorporeal life support) has led to an increase in the rates of eCPR. In the small, single-centre ARREST trial conducted in a high-volume centre, a clear advantage of eCPR over conventional CPR was observed [26]. The Prague-OHCA trial was also a single-centre trial and compared an invasive approach including intra-arrest transport, eCPR, and immediate invasive assessment and treatment with a standard approach. The results regarding the primary endpoint (survival with good neurological outcome at 180 days) were neutral. The secondary endpoint, neurological recovery at 30 days, was observed significantly more often in the hyperinvasive group [27]. The most recently published randomized and only multicentre trial in this field is the INCEPTION trial conducted in 10 centres in the Netherlands. Herein, no improvement of survival with a favourable neurological outcome at 30 days was observed for eCPR [28]. The use of eCPR in G-CAR (11.0%) is higher compared to data from other registries. In a prospective registry conducted in Paris including more than 13,000 patients between 2011 and 2018, eCPR was performed in 4.0%. The GRR reported the use of ECLS in 8.3% of OHCA patients in 2021, without specifying the proportion of eCPR [29]. The higher use of eCPR in our registry most likely reflects the selection of centres. A major future task will be to understand whether there are subgroups of patients who might benefit from such a highly invasive, expensive, and resource-binding treatment. Besides the conduction of further randomized clinical trials, registries reflecting the real-world will help to provide answers.
Outcomes
The observed in-hospital mortality was 70.5%; i.e., 29.5% of patients were discharged alive. According to the GRR 2022 report, 10.7% of the patients survived 30 days or were discharged alive [10]. However, the outcome data of the two registries are not comparable since the GRR reports total mortality rates, meaning that in contrast to G-CAR, the GRR also includes patients who are declared dead before arrival at the hospital. Notably, the survival rate of OHCA patients reaching the hospital in the large EuReCa TWO study was 26.4%, i.e. similar to our results [5]. Furthermore, there are more patients with respiratory/hypoxic and non-cardiac causes, such as trauma or drowning, in the GRR compared to G-CAR, which might lead to worse survival rates. Anoxic brain damage was the main cause of death and in more than half of the patients in hospital treatment was terminated, mainly because of brain damage or the patient's will. This underlines the need for an early and standardized neurological assessment and for a trained team taking care of the patients and relatives and discussing the patient’s (presumed) will in order to provide a medically and ethically correct treatment.
Post-hospital phase
Psychosocial aspects such as health-related quality of life and psychopathological symptoms are important sequelae after OHCA [30]. As described previously (9), we are investigating several patient-reported outcomes such as quality of life, affective disorders, social reintegration, post-traumatic stress syndrome, as well as cognitive impairment by postal dispatch of standardized questionnaires and telephone interviews at 6 and 12 months. Publication of these results is planned separately.
Limitations
G-CAR is a registry study with all well-known limitations of registries. However, registry studies are important to provide “real-world” data adding information to the results of randomized clinical trials and showing the extent to which they are implemented in clinical practice. Furthermore, registries are an important tool for quality control and are requested for certification as cardiac arrest centre. Another limitation is the above-mentioned centre bias with a focus on tertiary centres including many patients with underlying cardiac causes, especially ACS, impairing the generalizability of the data. Furthermore, the lack of information about the number of patients refusing participation might induce a bias towards the deceased patients. Last, missing values for specific parameters might induce a bias in the estimated results.
Summary
G-CAR is a national multicentre registry of adult OHCA patients, providing detailed information with a focus on interventional treatment aspects. The results of the 16-month pilot phase are presented herein. The fact that the available evidence for OHCA patients is often scarce or contradictory underlines the usefulness of this first cardiologic resuscitation registry. Besides the national extension of G-CAR, assessment and publication of the patient-reported outcomes is planned.
References
Nichols M, Townsend N, Scarborough P, Rayner M (2013) Trends in age-specific coronary heart disease mortality in the European Union over three decades: 1980–2009. Eur Heart J 34(39):3017–3027
Chan PS, McNally B, Tang F, Kellermann A, Group CS (2014) Recent trends in survival from out-of-hospital cardiac arrest in the United States. Circulation. 130(21):1876–82
Wissenberg M, Lippert FK, Folke F, Weeke P, Hansen CM, Christensen EF et al (2013) Association of national initiatives to improve cardiac arrest management with rates of bystander intervention and patient survival after out-of-hospital cardiac arrest. JAMA 310(13):1377–1384
Gräsner JT, Lefering R, Koster RW, Masterson S, Böttiger BW, Herlitz J et al (2016) EuReCa ONE-27 Nations, ONE Europe, ONE Registry: a prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation 105:188–195
Gräsner JT, Wnent J, Herlitz J, Perkins GD, Lefering R, Tjelmeland I et al (2020) Survival after out-of-hospital cardiac arrest in Europe - results of the EuReCa TWO study. Resuscitation 148:218–226
Hayashi M, Shimizu W, Albert CM (2015) The spectrum of epidemiology underlying sudden cardiac death. Circ Res 116(12):1887–1906
Scholz KH, Andresen D, Böttiger BW, Busch HJ, Fischer M, Frey N et al (2017) Quality indicators and structural requirements for cardiac arrest centers-German Resuscitation Council (GRC). Med Klin Intensivmed Notfmed 112(5):459–461
Hassager C, Nagao K, Hildick-Smith D (2018) Out-of-hospital cardiac arrest: in-hospital intervention strategies. Lancet 391(10124):989–998
Pöss J, Sinning C, Schreiner I, Apfelbacher C, Drewitz KP, Hösler N et al (2023) German Cardiac Arrest Registry: rationale and design of G-CAR. Clin Res Cardiol 112(4):455–463
Fischer MWJ, Gräsner J-T, Seewald S (2023) Jahresbericht des Deutschen Reanimationsregisters: Außerklinische Reanimation im Notarzt- und Rettungsdienst 2022. Anästh Intensivmed 64:V161–V169
Wingen S, Rott N, Schittko N, Hackstein A, Kreimeier U, Bartholme B et al (2022) State of implementation of telephone cardiopulmonary resuscitation by rescue coordination centers in Germany. Dtsch Arztebl Int 119(4):55–56
Andelius L, Malta Hansen C, Lippert FK, Karlsson L, Torp-Pedersen C, KjaerErsboll A et al (2020) Smartphone activation of citizen responders to facilitate defibrillation in out-of-hospital cardiac arrest. J Am Coll Cardiol 76(1):43–53
Gregers MCT, Andelius L, Kjoelbye JS, JuulGrabmayr A, Jakobsen LK, Bo Christensen N et al (2023) Association between number of volunteer responders and interventions before ambulance arrival for cardiac arrest. J Am Coll Cardiol 81(7):668–680
Noc M, Fajadet J, Lassen JF, Kala P, MacCarthy P, Olivecrona GK et al (2014) Invasive coronary treatment strategies for out-of-hospital cardiac arrest: a consensus statement from the European Association for Percutaneous Cardiovascular Interventions (EAPCI)/Stent for Life (SFL) groups. EuroIntervention 10(1):31–37
Desch S, Freund A, Akin I, Behnes M, Preusch MR, Zelniker TA et al (2021) Angiography after out-of-hospital cardiac arrest without ST-segment elevation. N Engl J Med 385(27):2544–2553
Lemkes JS, Janssens GN, van der Hoeven NW, Jewbali LSD, Dubois EA, Meuwissen M et al (2019) Coronary angiography after cardiac arrest without ST-segment elevation. N Engl J Med 380(15):1397–1407
Hamidi F, Anwari E, Spaulding C, Hauw-Berlemont C, Vilfaillot A, Viana-Tejedor A, Kern KB, Hsu CH, Bergmark BA, Qamar A, Bhatt DL, Furtado RHM, Myhre PL, Hengstenberg C, Lang IM, Frey N, Freund A, Desch S, Thiele H, Preusch MR, Zelniker TA (2024) Early versus delayed coronary angiography in patients with out-of-hospital cardiac arrest and no ST-segment elevation: a systematic review and meta-analysis of randomized controlled trials. Clin Res Cardiol 113(4):561–569. https://doi.org/10.1007/s00392-023-02264-7
Thiele H, Akin I, Sandri M, Fuernau G, de Waha S, Meyer-Saraei R, Nordbeck P, Geisler T, Landmesser U, Skurk C, Fach A (2017) PCI strategies in patients with acute myocardial infarction and cardiogenic shock. N Engl J Med 377(25):2419–2432
Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U et al (2019) 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J 40(2):87–165
Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A et al (2023) 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J 44(38):3720–3826
Dankiewicz J, Cronberg T, Lilja G, Jakobsen JC, Levin H, Ullen S et al (2021) Hypothermia versus normothermia after out-of-hospital cardiac arrest. N Engl J Med 384(24):2283–2294
Michels GB, J., Böttiger B.W. Leitlinien des European Resuscitation Council (ERC) zurkardiopulmonalen Reanimation, (2021) Update und Kommentar. Kardiologe 2022(16):22–33
Arrich J, Schutz N, Oppenauer J, Vendt J, Holzer M, Havel C et al (2023) Hypothermia for neuroprotection in adults after cardiac arrest. Cochrane Database Syst Rev 5(5):CD004128
Busch HJ, Behringer W, Biever P, Bottiger BW, Eisenburger P, Fink K et al (2023) Hypothermic temperature control after successful resuscitation of out-of-hospital cardiac arrest in adults: statement from the resuscitation and postresuscitation treatment working groups of the German Society of Medical Intensive Care and Emergency Medicine (DGIIN) and the German Interdisciplinary Association for Intensive Care and Emergency Medicine (DIVI), the German Society for Interdisciplinary Emergency and Acute Medicine (DGINA) and the Austrian Association of Emergency Medicine (AAEM). Med Klin Intensivmed Notfmed 118(Suppl 1):59–63
Behringer W, Böttiger BW, Biasucci DG, Chalkias A, Connolly J, Dodt C, Khoury A, Laribi S, Leach R, Ristagno G (2024) Temperature control after successful resuscitation from cardiac arrest in adults: a joint statement from the European Society for Emergency Medicine and the European Society of Anaesthesiology and Intensive Care. Eur J Anaesthesiol 1;41(4):278–281. https://doi.org/10.1097/EJA.0000000000001948
Yannopoulos D, Bartos J, Raveendran G, Walser E, Connett J, Murray TA et al (2020) Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet 396(10265):1807–1816
Belohlavek J, Smalcova J, Rob D, Franek O, Smid O, Pokorna M et al (2022) Effect of intra-arrest transport, extracorporeal cardiopulmonary resuscitation, and immediate invasive assessment and treatment on functional neurologic outcome in refractory out-of-hospital cardiac arrest: a randomized clinical trial. JAMA 327(8):737–747
Suverein MM, Maessen JG, van de Poll MCG (2023) Extracorporeal cardiopulmonary resuscitation in out-of-hospital cardiac arrest - current status. Curr Opin Crit Care 29(6):633–639
Bougouin W, Dumas F, Lamhaut L, Marijon E, Carli P, Combes A et al (2020) Extracorporeal cardiopulmonary resuscitation in out-of-hospital cardiac arrest: a registry study. Eur Heart J 41(21):1961–1971
Haywood K, Whitehead L, Nadkarni VM, Achana F, Beesems S, Bottiger BW et al (2018) COSCA (Core Outcome Set for Cardiac Arrest) in adults: an advisory statement from the International Liaison Committee on Resuscitation. Circulation 137(22):e783–e801
Funding
Open Access funding enabled and organized by Projekt DEAL. German Heart Research Foundation: Grant number: F/07/20.
Dr. Rolf M. Schwiete Foundation: Grant number: 2020–029.
German Cardiac Society (DGK) – Centre for Cardiological Care Research (DGK-ZfKVF).
Maquet Cardiopulmonary GmbH.
The G-CAR project is an investigator-initiated registry supported by the German Cardiac Society – Zentrum für kardiologische Versorgungsforschung (DGK-ZfKVF), the German Heart Research Foundation, the Dr. Rolf M. Schwiete Foundation, and Maquet Cardiopulmonary GmbH. The Leipzig Heart Science GmbH and the individual centres provide additional funding. The authors are solely responsible for the design and conduct of this study, all study analyses, the drafting and editing of the paper, and its final contents. The above-mentioned foundations and organisations have no influence on the study design, data collection, data analysis, and final drafting of this manuscript.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
BWB is treasurer of the European Resuscitation Council (ERC), Chairman of the German Resuscitation Council (GRC), Member of the Advanced Life Support (ALS) Task Force of the International Liaison Committee on Resuscitation (ILCOR), Member of the Executive Committee of the German Interdisciplinary Association for Intensive Care and Emergency Medicine (DIVI), Founder of the “Deutsche Stiftung Wiederbelebung”, Federal Medical Advisor of the German Red Cross (DRK), Co-Editor of “Resuscitation”, Editor of the Journal “Notfall + Rettungsmedizin”, Co-Editor of the Brazilian Journal of Anesthesiology. He received fees for lectures from the following companies: Forum für medizinische Fortbildung (FomF), Baxalta Deutschland GmbH, ZOLL Medical Deutschland GmbH, C.R. Bard GmbH, GS Elektromedizinische Geräte G. Stemple GmbH, Novartis Pharma GmbH, Philips GmbH Market DACH, Bioscience Valuation BSV GmbH.
SE received speakers or consultant honorarium and/or travel support from Medtronic, Recor, Bayer, Berlin Chemie, Böhringer Ingelheim, Daiichi Sankyo, Novartis, AstraZeneca, Akcea Therapeutics, and Bristol-Myers Squibb-Pfizer.
GM received lecture fees from Orion Pharma and Getinge. The conflicts of interest are not related to the present work.
HW has received speakers or consultant honoraria from Boehringer Ingelheim, AstraZeneca, Novartis, and Bristol-Myers Squibb, outside the submitted work.
JD has received speakers and/or consultant honoraria from Novo Nordisk, Pfizer, Bayer, Bristol-Myers Squibb, and Daiichi Sankyo. He is chairing the section “Ethics” of the DIVI and the project group “Ethics in cardiology” of the German Cardiac Society.
UZ: Speakers honoraria and research support from AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Ferrer, Novartis, Pfizer, and Sanofi.
JP received institutional research grants from German Cardiac Society, German Heart Research Foundation, Dr. Rolf M. Schwiete Foundation and Maquet Cardiopulmonary GmbH.
Additional information
Janine Pöss and Christoph Sinning are first authors.
Holger Thiele and Uwe Zeymer are senior authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pöss, J., Sinning, C., Roßberg, M. et al. German Cardiac Arrest Registry (G-CAR)—results of the pilot phase. Clin Res Cardiol (2024). https://doi.org/10.1007/s00392-024-02468-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00392-024-02468-5