
Abstract
Background
In myocardial infarction without cardiogenic shock (CS), the affected coronary vessel has significant influence on the final infarct size and patient prognosis. CS data on this relation are scarce. The objective of this study was to determine the prognostic relevance of the culprit lesion location in patients with CS complicating acute myocardial infarction.
Methods
In the Intraaortic Balloon Pump in Cardiogenic Shock II (IABP-SHOCK II) trial patients with CS were randomized to therapy with intraaortic balloon pump or control. Additional CS patients not eligible for the randomized trial were included in a registry. We compared the location of the culprit lesions in these patients with regard to the affected coronary vessel [left main (LM), left anterior descending (LAD), left circumflex (LCX) and right coronary artery (RCA)] and location within the vessel (proximal, mid or distal) regarding short- and long-term outcome.
Results
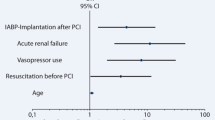
Of 758 patients, the majority had the culprit lesion in the LAD (44 %) compared to RCA (27 %), LCX (19 %) or LM (10 %). Proximal lesions were more frequent than mid or distal culprit lesions (60 vs. 27 vs. 13 %, p < 0.001). No differences were observed for mortality with respect to either culprit vessel (log-rank p value = 0.54). In contrast, a higher mortality was observed for patients with distal culprit lesions after 1 year (log-rank p value = 0.04). This difference persisted after multivariable adjustment (hazard ratio for distal lesions 1.40; 95 % confidential interval 1.03–1.90; p = 0.03).
Conclusion
For patients with CS complicating myocardial infarction, the culprit vessel seems to be unrelated with mortality whereas distal culprit lesions may have a worse outcome




Similar content being viewed by others


Abbreviations
- AMI:
-
Acute myocardial infarction
- CS:
-
Cardiogenic shock
- DES:
-
Drug-eluting stent
- LAD:
-
Left anterior descending coronary artery
- LCX:
-
Left circumflex coronary artery
- LM:
-
Left main coronary artery
- PCI:
-
Percutaneous coronary intervention
- RCA:
-
Right coronary artery
- STEMI:
-
ST-segment-elevation myocardial infarction
- TIMI:
-
Thrombolysis in myocardial infarction
References
Thiele H, Schuler G (2009) Cardiogenic shock: to pump or not to pump? Eur Heart J 30(4):389–390. doi:10.1093/eurheartj/ehp030
Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J (2009) Thirty-year trends (1975–2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation 119(9):1211–1219. doi:10.1161/CIRCULATIONAHA.108.814947
Karha J, Murphy SA, Kirtane AJ, de Lemos JA, Aroesty JM, Cannon CP, Antman EM, Braunwald E, Gibson CM, Group TS (2003) Evaluation of the association of proximal coronary culprit artery lesion location with clinical outcomes in acute myocardial infarction. Am J Cardiol 92(8):913–918
Harjai KJ, Mehta RH, Stone GW, Boura JA, Grines L, Brodie BR, Cox DA, O’Neill WW, Grines CL, Primary Angioplasty In Myocardial Infarction I (2006) Does proximal location of culprit lesion confer worse prognosis in patients undergoing primary percutaneous coronary intervention for ST elevation myocardial infarction? J Interv Cardiol 19(4):285–294. doi:10.1111/j.1540-8183.2006.00146.x
Hands ME, Lloyd BL, Robinson JS, de Klerk N, Thompson PL (1986) Prognostic significance of electrocardiographic site of infarction after correction for enzymatic size of infarction. Circulation 73(5):885–891
Stone PH, Raabe DS, Jaffe AS, Gustafson N, Muller JE, Turi ZG, Rutherford JD, Poole WK, Passamani E, Willerson JT et al (1988) Prognostic significance of location and type of myocardial infarction: independent adverse outcome associated with anterior location. J Am Coll Cardiol 11(3):453–463
Kandzari DE, Tcheng JE, Gersh BJ, Cox DA, Stuckey T, Turco M, Mehran R, Garcia E, Zimetbaum P, McGlaughlin MG, Lansky AJ, Costantini CO, Grines CL, Stone GW (2006) Relationship between infarct artery location, epicardial flow, and myocardial perfusion after primary percutaneous revascularization in acute myocardial infarction. Am Heart J 151(6):1288–1295. doi:10.1016/j.ahj.2005.08.017
Nienhuis MB, Ottervanger JP, Dambrink JH, de Boer MJ, Hoorntje JC, Gosselink AT, Suryapranata H, van ‘t Hof AW (2009) Comparative predictive value of infarct location, peak CK, and ejection fraction after primary PCI for ST elevation myocardial infarction. Coron Artery Dis 20(1):9–14. doi:10.1097/MCA.0b013e32831bd875
Conde-Vela C, Moreno R, Hernandez R, Perez-Vizcayno MJ, Alfonso F, Escaned J, Sabate M, Banuelos C, Macaya C (2007) Cardiogenic shock at admission in patients with multivessel disease and acute myocardial infarction treated with percutaneous coronary intervention: related factors. Int J Cardiol 123(1):29–33. doi:10.1016/j.ijcard.2006.11.102
Trzeciak P, Gierlotka M, Gasior M, Lekston A, Wilczek K, Slonka G, Kalarus Z, Zembala M, Hudzik B, Polonski L (2013) Mortality of patients with ST-segment elevation myocardial infarction and cardiogenic shock treated by PCI is correlated to the infarct-related artery–results from the PL-ACS Registry. Int J Cardiol 166(1):193–197. doi:10.1016/j.ijcard.2011.10.100
Wong SC, Sanborn T, Sleeper LA, Webb JG, Pilchik R, Hart D, Mejnartowicz S, Antonelli TA, Lange R, French JK, Bergman G, LeJemtel T, Hochman JS (2000) Angiographic findings and clinical correlates in patients with cardiogenic shock complicating acute myocardial infarction: a report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK? J Am Coll Cardiol 36(3 Suppl A):1077–1083
Kunadian V, Qiu W, Ludman P, Redwood S, Curzen N, Stables R, Gunn J, Gershlick A (2014) Outcomes in patients with cardiogenic shock following percutaneous coronary intervention in the contemporary era: an analysis from the BCIS database (British Cardiovascular Intervention Society). JACC Cardiovasc Interv 7(12):1374–1385. doi:10.1016/j.jcin.2014.06.017
Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, Richardt G, Hennersdorf M, Empen K, Fuernau G, Desch S, Eitel I, Hambrecht R, Fuhrmann J, Bohm M, Ebelt H, Schneider S, Schuler G, Werdan K (2012) Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med 367(14):1287–1296. doi:10.1056/NEJMoa1208410
Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, da Waha A, Richardt G, Hennersdorf M, Empen K, Fuernau G, Desch S, Eitel I, Hambrecht R, Lauer B, Bohm M, Ebelt H, Schneider S, Werdan K, Schuler G (2013) Intra-aortic balloon counterpulsation in acute myocardial infarction complicated by cardiogenic shock (IABP-SHOCK II): final 12 month results of a randomised, open-label trial. Lancet 382(9905):1638–1645. doi:10.1016/S0140-6736(13)61783-3
Thiele H, Schuler G, Neumann FJ, Hausleiter J, Olbrich HG, Schwarz B, Hennersdorf M, Empen K, Fuernau G, Desch S, de Waha S, Eitel I, Hambrecht R, Bohm M, Kurowski V, Lauer B, Minden HH, Figulla HR, Braun-Dullaeus RC, Strasser RH, Rochor K, Maier SK, Mollmann H, Schneider S, Ebelt H, Werdan K, Zeymer U (2012) Intraaortic balloon counterpulsation in acute myocardial infarction complicated by cardiogenic shock: design and rationale of the Intraaortic Balloon Pump in Cardiogenic Shock II (IABP-SHOCK II) trial. Am Heart J 163(6):938–945. doi:10.1016/j.ahj.2012.03.012
Austen WG, Edwards JE, Frye RL, Gensini GG, Gott VL, Griffith LS, McGoon DC, Murphy ML, Roe BB (1975) A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for grading of coronary artery disease, council on cardiovascular surgery, American Heart Association. Circulation 51(4 Suppl):5–40
Kappetein AP, Feldman TE, Mack MJ, Morice MC, Holmes DR, Stahle E, Dawkins KD, Mohr FW, Serruys PW, Colombo A (2011) Comparison of coronary bypass surgery with drug-eluting stenting for the treatment of left main and/or three-vessel disease: 3-year follow-up of the SYNTAX trial. Eur Heart J 32(17):2125–2134. doi:10.1093/eurheartj/ehr213
Chieffo A, Morici N, Maisano F, Bonizzoni E, Cosgrave J, Montorfano M, Airoldi F, Carlino M, Michev I, Melzi G, Sangiorgi G, Alfieri O, Colombo A (2006) Percutaneous treatment with drug-eluting stent implantation versus bypass surgery for unprotected left main stenosis: a single-center experience. Circulation 113(21):2542–2547. doi:10.1161/CIRCULATIONAHA.105.595694
Buszman PE, Kiesz SR, Bochenek A, Peszek-Przybyla E, Szkrobka I, Debinski M, Bialkowska B, Dudek D, Gruszka A, Zurakowski A, Milewski K, Wilczynski M, Rzeszutko L, Buszman P, Szymszal J, Martin JL, Tendera M (2008) Acute and late outcomes of unprotected left main stenting in comparison with surgical revascularization. J Am Coll Cardiol 51(5):538–545. doi:10.1016/j.jacc.2007.09.054
Seung KB, Park DW, Kim YH, Lee SW, Lee CW, Hong MK, Park SW, Yun SC, Gwon HC, Jeong MH, Jang Y, Kim HS, Kim PJ, Seong IW, Park HS, Ahn T, Chae IH, Tahk SJ, Chung WS, Park SJ (2008) Stents versus coronary-artery bypass grafting for left main coronary artery disease. N Engl J Med 358(17):1781–1792. doi:10.1056/NEJMoa0801441
Boudriot E, Thiele H, Walther T, Liebetrau C, Boeckstegers P, Pohl T, Reichart B, Mudra H, Beier F, Gansera B, Neumann FJ, Gick M, Zietak T, Desch S, Schuler G, Mohr FW (2011) Randomized comparison of percutaneous coronary intervention with sirolimus-eluting stents versus coronary artery bypass grafting in unprotected left main stem stenosis. J Am Coll Cardiol 57(5):538–545. doi:10.1016/j.jacc.2010.09.038
Chen SL, Ye F, Zhang JJ, Hu ZY, Tian NL, Zhang JX, Kwan TW (2010) Prediction of clinical outcomes in patients with unprotected left main trifurcation lesions treated by drug-eluting stents: importance of 2-stent technique and SYNTAX score. J Interv Cardiol 23(4):352–357. doi:10.1111/j.1540-8183.2010.00569.x
Chen SL, Xu B, Han YL, Sheiban I, Zhang JJ, Ye F, Kwan TW, Paiboon C, Zhou YJ, Lv SZ, Dangas GD, Xu YW, Wen SY, Hong L, Zhang RY, Wang HC, Jiang TM, Wang Y, Chen F, Yuan ZY, Li WM, Leon MB (2013) Comparison of double kissing crush versus Culotte stenting for unprotected distal left main bifurcation lesions: results from a multicenter, randomized, prospective DKCRUSH-III study. J Am Coll Cardiol 61(14):1482–1488. doi:10.1016/j.jacc.2013.01.023
Chen SL, Zhang Y, Xu B, Ye F, Zhang J, Tian N, Liu Z, Qian X, Ding S, Li F, Zhang A, Liu Y, Lin S (2012) Five-year clinical follow-up of unprotected left main bifurcation lesion stenting: one-stent versus two-stent techniques versus double-kissing crush technique. EuroIntervention 8(7):803–814. doi:10.4244/eijv8i7a123
Park SJ, Ahn JM, Kim YH, Park DW, Yun SC, Yoon SH, Park HW, Chang M, Lee JY, Kang SJ, Lee SW, Lee CW, Park SW (2015) Temporal trends in revascularization strategy and outcomes in left main coronary artery stenosis: data from the ASAN medical center-left main revascularization registry. Circ Cardiovasc Interv. doi:10.1161/circinterventions.114.001846
Vis MM, Beijk MA, Grundeken MJ, Baan J Jr, Koch KT, Wykrzykowska JJ, Arkenbout EK, Tijssen JG, de Winter RJ, Piek JJ, Henriques JP (2013) A systematic review and meta-analysis on primary percutaneous coronary intervention of an unprotected left main coronary artery culprit lesion in the setting of acute myocardial infarction. JACC Cardiovasc Interv 6(4):317–324. doi:10.1016/j.jcin.2012.10.020
Waziri H, Jorgensen E, Kelbaek H, Fosbol EL, Pedersen F, Mogensen UM, Gerds TA, Kober L, Wachtell K (2015) Acute myocardial infarction and lesion location in the left circumflex artery: importance of coronary artery dominance. EuroIntervention. doi:10.4244/eijy15m09_04
Kuno T, Kohsaka S, Numasawa Y, Ueda I, Suzuki M, Nakamura I, Negishi K, Ishikawa S, Maekawa Y, Kawamura A, Miyata H, Fukuda K (2015) Location of the culprit coronary lesion and its association with delay in door-to-balloon time (from a multicenter registry of primary percutaneous coronary intervention). Am J Cardiol 115(5):581–586. doi:10.1016/j.amjcard.2014.12.004
Scholz KH, Maier SK, Jung J, Fleischmann C, Werner GS, Olbrich HG, Ahlersmann D, Keating FK, Jacobshagen C, Moehlis H, Hilgers R, Maier LS (2012) Reduction in treatment times through formalized data feedback: results from a prospective multicenter study of ST-segment elevation myocardial infarction. JACC Cardiovasc Interv 5(8):848–857. doi:10.1016/j.jcin.2012.04.012
Towae F, Juenger C, Mudra H, Glunz HG, Hauptmann E, Grube E, Voigtlander T, Bauer T, Zeymer U, Senges J, Gitt AK, Zahn R (2011) The development of door-to-angiography time in the last 14 years for patients with acute ST-elevation myocardial infarction treated with primary coronary intervention: determinants and outcome. Results from the MITRAplus and OPTAMI registry. Acute Card Care 13(1):35–39. doi:10.3109/17482941.2010.551133
Muller UM, Eitel I, Eckrich K, Erbs S, Linke A, Mobius-Winkler S, Mende M, Schuler GC, Thiele H (2011) Impact of minimising door-to-balloon times in ST-elevation myocardial infarction to less than 30 min on outcome: an analysis over an 8-year period in a tertiary care centre. Clin Res Cardiol 100(4):297–309. doi:10.1007/s00392-010-0242-7
Kellner P, Prondzinsky R, Pallmann L, Siegmann S, Unverzagt S, Lemm H, Dietz S, Soukup J, Werdan K, Buerke M (2013) Predictive value of outcome scores in patients suffering from cardiogenic shock complicating AMI: APACHE II, APACHE III, Elebute-Stoner, SOFA, and SAPS II. Med Klin Intensivmed Notfmed 108(8):666–674. doi:10.1007/s00063-013-0234-2
Reynolds HR, Hochman JS (2008) Cardiogenic shock: current concepts and improving outcomes. Circulation 117(5):686–697. doi:10.1161/CIRCULATIONAHA.106.613596
Stegman BM, Newby LK, Hochman JS, Ohman EM (2012) Post-myocardial infarction cardiogenic shock is a systemic illness in need of systemic treatment: is therapeutic hypothermia one possibility? J Am Coll Cardiol 59(7):644–647. doi:10.1016/j.jacc.2011.11.010
Fengler K, Fuernau G, Desch S, Eitel I, Neumann FJ, Olbrich HG, de Waha A, de Waha S, Richardt G, Hennersdorf M, Empen K, Hambrecht R, Fuhrmann J, Bohm M, Poess J, Strasser R, Schneider S, Schuler G, Werdan K, Zeymer U, Thiele H (2015) Gender differences in patients with cardiogenic shock complicating myocardial infarction: a substudy of the IABP-SHOCK II-trial. Clin Res Cardiol 104(1):71–78. doi:10.1007/s00392-014-0767-2
Fuernau G, Poenisch C, Eitel I, de Waha S, Desch S, Schuler G, Adams V, Werdan K, Zeymer U, Thiele H (2014) Growth-differentiation factor 15 and osteoprotegerin in acute myocardial infarction complicated by cardiogenic shock: a biomarker substudy of the IABP-SHOCK II-trial. Eur J Heart Fail 16(8):880–887. doi:10.1002/ejhf.117
Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, LeJemtel TH (1999) Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK investigators. Should we emergently revascularize occluded coronaries for cardiogenic shock. N Engl J Med 341(9):625–634. doi:10.1056/NEJM199908263410901
Geske JB, Edwards WD, MacDonald RJ, Holmes DR Jr (2010) Location of coronary culprit lesions at autopsy in 41 nondiabetic patients with acute myocardial infarction. Am J Forensic Med Pathol 31(3):213–217. doi:10.1097/PAF.0b013e3181dd7949
Arinell K, Josefsson J, Magnuson A, Frobert O (2011) Angiographic morphology impacts outcomes in STEMI patients with LAD occlusion. Catheter Cardiovasc Interv 77(1):29–34. doi:10.1002/ccd.22604
Acknowledgments
The IABP-SHOCK II-trial has been approved by the local ethics committee at each participating center and has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All patients in the randomized study or their legally authorized representatives provided written informed consent.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Supported by grants from the German Research Foundation (Bonn, Germany), the German Heart Research Foundation (Frankfurt, Germany), the German Cardiac Society (Düsseldorf, Germany), Arbeitsgemeinschaft Leitende Kardiologische Krankenhausärzte (Berlin, Germany), the University of Leipzig-Heart Center (Leipzig, Germany) and by unrestricted grants from Maquet Cardiopulmonary (Rastatt, Germany) and Teleflex Medical (Wayne, PA, USA).
Conflict of interest
Dr. Thiele reports receiving consulting fees from Eli Lilly (Indianapolis, IN, USA) grant support on behalf of his institution from Eli Lilly and Terumo (Tokyo, Japan), and lecture fees from AstraZeneca (London, UK), Boehringer Ingelheim (Ingelheim, Germany), Daiichi Sankyo (Chuo, Japan), Eli Lilly, the Medicines Company (Leipzig, Germany), and Terumo; Dr. Zeymer reports serving on the board of Daiichi Sankyo and Eli Lilly and receiving consulting and lecture fees from Daiichi Sankyo, Eli Lilly and the Medicines Company; Dr. Richardt reports receiving lecture fees from Maquet Cardiovascular; Dr. Böhm received consulting fees from AstraZeneca, Bayer (Leverkusen, Germany), Boehringer Ingelheim, Daiichi Sankyo, Medtronic (Minneapolis, MN, USA), Merck (White House Station, NJ, USA), Novartis (Basel, Switzerland), Pfizer (New York City, NY, USA), Sanofi Aventis (Paris, France), and Servier (Neuilly-sur-Seine, France) and lecture fees from AstraZeneca, AWD.pharma Dresden (Radebeul, Germany), Bayer, Berlin-Chemie (Berlin, Germany), Boehringer Ingelheim, Daiichi Sankyo, Merck, Novartis, Pfizer, Sanofi Aventis, and Servier; Dr. Schneider reports serving on the ethics committee of Landesärztekammer Baden-Württemberg (Stuttgart, Germany), receiving payment for manuscript preparation from Biosense Webster (Diamond Bar, CA, USA), Grupo Ferrer (Barcelona, Spain), and Nycomed (Opfikon, Switzerland), and receiving money on behalf of the clinical research organization at his institution from Abbott Vascular (Chicago, IL, USA), AstraZeneca, Bayer, Biotronik (Berlin, Germany), Bristol-Myers Squibb (New York City, NY, USA), Boehringer Ingelheim, Cordis (Bridgewater Township, NJ, USA), Daiichi Sankyo, Diagenics (Luxembourg, Luxembourg), Enverdis (Jena, Germany), Eli Lilly, GlaxoSmithKline (Brentford, UK), Guidant (Natick, MA, USA), IKKF (Munich, Germany), Impulse Dynamics (Stuttgart, Germany), Medtronic, Merck, Novartis, Roche Diagnostics (Rotkreuz, Switzerland), Sanofi Aventis, Schering-Plough (Kenilworth, NJ, USA), Siemens (Munich, Germany), St. Jude Medical (Saint Paul, MN, USA), Takeda Pharma (Osaka, Japan), Tromssdorff (Alsdorf, Germany), and Vifor Pharma (Munich, Germany); and Dr. Werdan reports serving on the board of Biotest (Dreieich, Germany) and Servier, receiving grant support on behalf of his institution from Biotest and Servier, and receiving lecture fees from Biotest, Brahms (Henningsdorf, Germany), Maquet Cardiovascular, and Servier. Dr. Jung reports receiving grant support on behalf of his institution from Bayer Healthcare (Leverkusen, Germany), Actelion Pharmaceuticals (Freiburg, Germany) and Novartis (Basel, Switzerland), and lecture fees Bayer Healthcare (Leverkusen, Germany), Actelion Pharmaceuticals (Freiburg, Germany), Novartis (Basel, Switzerland), Boehringer Ingelheim (Ingelheim, Germany), Vifor Pharma (Glattbrugg, Switzerland), and Pfizer (Berlin, Germany). Dr. Pöss reports receiving lecture fees from AstraZeneca (London, UK). No other potential conflict of interest relevant to this article was reported.
Additional information
G. Fuernau and K. Fengler contributed equally to the manuscript.
Rights and permissions
About this article

Cite this article
Fuernau, G., Fengler, K., Desch, S. et al. Culprit lesion location and outcome in patients with cardiogenic shock complicating myocardial infarction: a substudy of the IABP-SHOCK II-trial. Clin Res Cardiol 105, 1030–1041 (2016). https://doi.org/10.1007/s00392-016-1017-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-016-1017-6