
Abstract
Purpose
Because there are few comparative studies of open, laparoscopy-assisted (LA), and robot-assisted (RA) total mesorectal excision (TME) for rectal cancer, we aimed to compare these three procedures in terms of sphincter-saving operation (SSO) achievement, surgical complications, and early oncological outcomes.
Methods
The short-term outcomes of 2114 patients with rectal cancer consecutively enrolled between July 2010 and February 2015 at Asan Medical Center (Seoul, Korea) were retrospectively evaluated. Patients underwent either open, LA, or RA TME (n = 1095, 486, and 533, respectively) performed by experienced surgeons.
Results
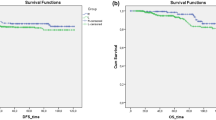
RA TME was a significant determinant of SSO in multivariate analysis that included potential variables such as tumor location and T4 category (odds ratio, 2.458; 95 % confidence interval, 1.497–4.036; p < 0.001). The cumulative rates of 3-year local recurrence, overall survival, and disease-free survival did not differ among the three groups: 2.5–3.4, 91.9–94.6, and 82.2–83.1 % (p = 0.85, 0.352, and 0.944, respectively). Early general surgical complications occurred more frequently in the open group than in the LA and RA groups (19.3 versus 13.0 versus 12.2 %, p < 0.001), specifically ileus and wound infection.
Conclusions
There were no significant differences in 3-year survival outcomes and local recurrence among open, LA, and RA TME. RA TME is useful for SSO achievement, regardless of advanced stage and location of rectal cancer. The open procedure had a slightly but significantly higher incidence of postoperative complications than LA and RA.

Similar content being viewed by others


References
Vennix S, Pelzers L, Bouvy N et al (2014) Laparoscopic versus open total mesorectal excision for rectal cancer. Cochrane Database Syst Rev 4, CD005200
Martling AL, Holm T, Rutqvist LE, Moran BJ, Heald RJ, Cedemark B (2000) Effect of a surgical training programme on outcome of rectal cancer in the County of Stockholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project. Lancet 356:93–96
Peeters KC, Marijnen CA, Nagtegaal ID et al (2007) The TME trial after a median follow-up of 6 years: increased local control but no survival benefit in irradiated patients with resectable rectal carcinoma. Ann Surg 246:693–701
Lange MM, Rutten HJ, van de Velde CJ (2009) One hundred years of curative surgery for rectal cancer: 1908–2008. Eur J Surg Oncol 35:456–463
Jayne DG, Thorpe HC, Copeland J, Quirke P, Brown JM, Guillou PJ (2010) Five-year follow-up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. Br J Surg 97:1638–1645
Bonjer HJ, Deijen CL, Abis GA et al (2015) A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med 372:1324–1332
Jeong SY, Park JW, Nam BH et al (2014) Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol 15:767–774
Smith JJ, Garcia-Aguilar J (2015) Advances and challenges in treatment of locally advanced rectal cancer. J Clin Oncol 33:1797–1808
Miskovic D, Foster J, Agha A et al (2015) Standardization of laparoscopic total mesorectal excision for rectal cancer: a structured international expert consensus. Ann Surg 261:716–722
Kim CW, Kim CH, Baik SH (2014) Outcomes of robotic-assisted colorectal surgery compared with laparoscopic and open surgery: a systematic review. J Gastrointest Surg 18:816–830
Araujo SE, Seid VD, Klajner S (2014) Robotic surgery for rectal cancer: current immediate clinical and oncological outcomes. World J Gastroenterol 20:14359–14370
Kim JC, Yang SS, Jang TY, Kwak JY, Yun MJ, Lim SB (2012) Open versus robot-assisted sphincter-saving operations in rectal cancer patients: techniques and comparison of outcomes between groups of 100 matched patients. Int J Med Robot 8:468–475
Kim JC, Lim SB, Yoon YS, Park IJ, Kim CW, Kim CN (2014) Completely abdominal intersphincteric resection for lower rectal cancer: feasibility and comparison of robot-assisted and open surgery. Surg Endosc 28:2734–2744
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Denost Q, Adam JP, Rullier A, Buscail E, Laurent C, Rullier E (2014) Perineal transanal approach: a new standard for laparoscopic sphincter-saving resection in low rectal cancer, a randomized trial. Ann Surg 260:993–999
Speicher PJ, Englum BR, Ganapathi AM, Nussbaum DP, Mantyh CR, Migaly J (2015) Robotic low anterior resection for rectal cancer: a national perspective on short-term oncologic outcomes. Ann Surg 262:1040–1045
Kim JC, Yu CS, Lim SB, Kim CW, Park IJ, Yoon YS (2015) Outcomes of ultra-low anterior resection combined with or without intersphincteric resection in lower rectal cancer patients. Int J Colorectal Dis 30:1311–1321
Qu H, Liu Y, Bi DS (2015) Clinical risk factors for anastomotic leakage after laparoscopic anterior resection for rectal cancer: a systematic review and meta-analysis. Surg Endosc 29:3608–3617
Park EJ, Cho MS, Baek SJ et al (2015) Long-term oncologic outcomes of robotic low anterior resection for rectal cancer: a comparative study with laparoscopic surgery. Ann Surg 261:129–137
Dinnewitzer A, Jäger T, Nawara C, Buchner S, Wolfgang H, Öfner D (2013) Cumulative incidence of permanent stoma after sphincter preserving low anterior resection of mid and low rectal cancer. Dis Colon Rectum 56:1134–1142
Kim JY, Kim NK, Lee KY, Hur H, Min BS, Kim JH (2012) A comparative study of voiding and sexual function after total mesorectal excision with autonomic nerve preservation for rectal cancer: laparoscopic versus robotic surgery. Ann Surg Oncol 19:2485–2493
Lim RS, Yang TX, Chua TC (2014) Postoperative bladder and sexual function in patients undergoing surgery for rectal cancer: a systematic review and meta-analysis of laparoscopic versus open resection of rectal cancer. Technol Coloproctol 18:993–1002
Pahlman L, Bujko K, Rutkowski A, Michalski W (2013) Altering the therapeutic paradigm towards a distal bowel margin of <1 cm in patients with low-lying rectal cancer: a systematic review and commentary. Colorectal Dis 15:e166–e174
Lykke J, Roikjaer O, Jess P, Danish Colorectal Cancer Group (2014) Tumour stage and preoperative chemoradiotherapy influence the lymph node yield in stages I-III rectal cancer: results from a prospective nationwide cohort study. Colorectal Dis 16:O144–O149
Law WL, Chu KW (2004) Anterior resection for rectal cancer with mesorectal excision: a prospective evaluation of 622 patients. Ann Surg 240:260–268
Amato A, Pescatori M (2006) Perioperative blood transfusions for the recurrence of colorectal cancer. Cochrane Database Syst Rev 1, CD005033
Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P (2011) Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg 253:890–899
Acknowledgments
This study was supported by grants (to J.C. Kim) from the Korea Research Foundation (2013R1A2A1A03070986), Ministry of Science, ICT, and Future Planning, and the Korea Health 21 R&D Project (HI06C0868 and HI13C1750), Ministry of Health, Welfare, and Family Affairs, Republic of Korea. We gratefully acknowledge the expert assistance of Dr. J. Y. Lee, Mr. Y. J. Yoon, Ms. J. R. Kim, and H. J. Jung.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All patients provided written informed consent, and the study protocol was approved by the Institutional Review Board of Asan Medical Center (registration number: 2015-0973) in accordance with the Declaration of Helsinki.
Conflict of interest
The authors declare that they have no conflict of interest.
Role of the funding source
None
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Fig. 1
Mean fold ratios of basic manometric parameters of evaluable patients (open/LA/RA groups: n = 182/52/251 patients). The data represent the ratios of the values obtained at 6–12 postoperative months to the preoperative values and were compared using an analysis or variance (ANOVA) test. MRP, maximal resting pressure; MSP, maximal squeezing pressure; UDV, urge to defecate volume; MTV, maximal tolerance volume. (GIF 37 kb)
Supplementary Fig. 2
Overall survival (a–c) and disease-free survival (d–f) of the open, LA, and RA groups according to the respective stage. Survival outcomes were compared using the Kaplan–Meier method with the log-rank test. LA, laparoscopy-assisted; RA, robot-assisted; OS, overall survival; DFS, disease-free survival. (GIF 57 kb)
Table S1
Parameters associated with SSO achievementa (DOCX 27 kb)
Table S2
Parameters associated postoperative ileus and anastomotic complicationsa (DOCX 25 kb)
Table S3
Parameters associated 3-year local recurrence (DOCX 24 kb)
Rights and permissions
About this article

Cite this article
Kim, J.C., Yu, C.S., Lim, SB. et al. Comparative analysis focusing on surgical and early oncological outcomes of open, laparoscopy-assisted, and robot-assisted approaches in rectal cancer patients. Int J Colorectal Dis 31, 1179–1187 (2016). https://doi.org/10.1007/s00384-016-2586-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-016-2586-6