
Abstract
Guillain-Barré syndrome has been defined as a post-infectious immune-mediated polyneuropathy. COVID-19 usually presents with respiratory symptoms but can less commonly present with extra-respiratory manifestations such as neurological symptoms. Few cases were published in the literature regarding post-COVID-19 infection Guillain-Barré in the pediatric age group. In this paper, we present a 13-year-old male with possible Guillain-Barré syndrome occurring 2 weeks after a presumed COVID-19 infection. We conducted a systematic review and searched for published pediatric cases until March 2022. We included 35 patients in 25 publications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Coronavirus disease (COVID-19) is caused by the novel coronavirus strain severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Studies showed that children have a lower incidence rate and milder symptoms when compared to adults [1]. Children typically present with fever, cough, pharyngitis, and rhinorrhea [2]. Immunocompromised children present with severe disease [3]. COVID-19 can less commonly present with extra-respiratory manifestations. Multiple studies have linked COVID-19 in adults and children with multiple central and peripheral neurological manifestations; however, children might be more susceptible to post-COVID-19 neurological injury due to their developing nervous system with differential expression of cell receptor targets over time [4]. Furthermore, a recent entity was recognized in late April 2020, called multisystem inflammatory syndrome in children (MIS-C) [5]. MIS-C is a post-infectious syndrome or inflammatory reaction following asymptomatic or mildly symptomatic COVID-19 related to SARS-CoV-2 infection in children and adolescents [6]. Both COVID-19 infection and MIS-C can give rise to neurological manifestations. In both scenarios, they present as central involvement such as encephalopathy, ischemic and hemorrhagic stroke, seizure, and meningoencephalitis or peripheral involvement such as cranial nerve impairment, myopathic involvement, or Guillain-Barré syndrome [7, 8]. Few studies reported an association between COVID-19 and Guillain-Barré syndrome (GBS) in children (Table 1) [8–28]. We present the first Jordanian case report of a 13-year-old male with possible GBS occurring 2 weeks after presumed COVID-19 infection.
Case presentation
A previously healthy 13-year-old male had a history of fever, cough, and runny nose with a history of concurrent direct contact with COVID-19-positive family members who live in the same household and did not quarantine. There was no diarrhea nor preceding history of vaccination. A nasopharyngeal SARS-CoV-2 PCR test yielded a negative result. Two weeks later, he presented with history of pain in thighs and back followed by progressive ascending weakness and unsteady gait. He visited the emergency room but was reassured that his complaint is related to his grief after the death of his grandfather from COVID-19. One month later, he presented to our child neurology clinic due to the persistence of weakness manifested by the inability to walk without support. Physical examination revealed stable vital signs and a normal general exam. His neurological examination revealed normal cranial nerves, normal tone in the upper limbs, and decreased tone in the lower limbs. Power was decreased in both upper and lower limbs but more marked distally. Power of the upper limbs proximally was 5/5, distally was 4/5. Power of the lower limbs proximally was 4/5, distally feet plantar flexion 4/5, and dorsiflexion 3/5. Deep tendon reflexes were absent in the upper and lower limbs. His gait was unsteady, and he was unable to walk without assistance. The sensation was intact.
Based on the history and examination, suspicion of a diagnosis of Guillain-Barré was raised.
The following investigations were done for him: complete blood count, C-reactive protein, and CK were normal. Serology test of SARS-CoV-2 showed positive IgG antibodies. The nerve conduction study showed demyelinating polyneuropathy with secondary axonal loss involving the upper and lower limbs. Cerebrospinal fluid (CSF) analysis revealed the following: cells: nil, protein 92, glucose 71. CSF SARS-CoV-2 RNA and oligoclonal bands in addition to serum anti-ganglioside antibody and anti Gq1b antibody were not tested. Antibodies for other viruses (adenovirus, EBV, CMV, influenza virus) and bacteria (Campylobacter jejuni, Mycoplasma pneumoniae) were not tested due to late diagnosis. Screening for autoimmune diseases was not done because the history, physical examination, and family history were not suggestive. In addition, neuroimaging including brain and spine MRI with contrast were normal, which could be attributable to delay of neuroimaging from the onset of symptoms and/or the use of steroids few days prior to neuroimaging. Based on the aforementioned clinical picture and investigations, we diagnosed the patient to have Guillain-Barré syndrome. We treated him with IVIG (dose 2 g/kg over 5 days) and methylprednisolone succinate (dose 1 g/day for 5 days), followed by oral prednisolone which was tapered over 1 month. Although corticosteroids are not indicated in GBS, however, we decided to give him both IVIG and methylprednisolone due to delayed diagnosis in addition to lack of guideline on how to treat patients with post-COVID-19 GBS and paucity of data in the literature. The patient’s power improved; however, a second dose of IVIG was given 1 month later because of incomplete recovery and persistence of unsteady gait. Follow-up 1 month later revealed normalization of power and gait with absent deep tendon reflexes.
Discussion
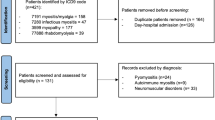
We presented a 13-year-old child who developed Guillain-Barré syndrome 2 weeks after COVID-19 infection. The clinical picture and diagnostic workup along with the presence of IgG to SARS-CoV-2 supported the diagnosis of missed post-COVID-19 GBS. We carried out a literature review and searched for published cases until March 2022. We used the keywords “COVID-19” or “SARS-CoV 2” together with “Guillain Barre Syndrome” or “GBS” or “Miller Fisher syndrome” or “Bickerstaff Encephalitis” and “Pediatrics” or “Children”. We included 35 patients in 25 publications. Their findings are summarized in Table 1 [8–32] and Table 2. Studies included 35 children in total, of which 22 were males and 13 were females. Ages varied between 2 and 18 years. The most common presentation was ascending progressive weakness. The clinical picture of COVID-19-associated GBS in children seems to resemble that of classic GBS [33]. The time elapsed from the onset of COVID-19 symptoms to the clinical GBS manifestations varied between 1 and 6 weeks. Of the 35 patients, the nasopharyngeal SARS-CoV-2 PCR test was performed in 22 patients; 17 patients yielded positive results. In contrast, similar to our patient, 5 patients yielded negative results. This can be attributed to the false-negative potential associated with the nasopharyngeal SARS-CoV-2 PCR test [34]. A serology test of SARS-CoV-2 was done for 12 patients, and all had positive serology. Our patient was diagnosed with acute inflammatory demyelinating polyradiculoneuropathy (AIDP) variant; likewise 9 patients had the same diagnosis. On the other hand, 6 patients were diagnosed with acute motor axonal neuropathy (AMAN), 3 patients with Miller Fisher syndrome (MFS), 1 with MFS with posterior reversible encephalopathy syndrome (PRES), 1 had unexcitable variant, and none had Bickerstaff encephalitis. Nerve conduction study was not done in 1 patient.
In congruence with our patient, the diagnosis was missed in 2 children. The first case was a 15-year-old male, who presented initially to the medical care with history of headache and fever followed by limb weakness but was not diagnosed until 2 weeks later [16]. The second case was a 2-year-old female, who presented initially to the medical care with left facial droop and abnormal gait but was diagnosed 3 weeks later with GBS [14]. Treatment was mentioned for 22 patients, 19 patients received 1 dose of IVIG, 2 patients received 2 doses of IVIG, 4 patients received steroids followed by IVIG, and 2 underwent plasma exchange. In all the reported pediatric cases of Guillain-Barré syndrome following COVID-19 infection, prognosis was good, as most showed complete recovery or significant improvement. Two treatment modalities have been proved to be equally effective for the treatment of GBS, either IVIG or plasma exchange with around 80% of patients being able to walk without assistance in 6 months [33].
Coronavirus is a family of enveloped positive-stranded RNA viruses [35]. WHO’s provisional case definition for the association of SARS-CoV-2 with neurological disease is probable when the onset of symptoms is within 6 weeks of suspected acute infection, RNA detected in any sample or antibody evidence of infection, and absence of other probable etiology on evaluation [36]. Studies of possible SARS-CoV-2 entry points showed that upon infection the virus attaches to the olfactory epithelium via the ACE-2 receptor; once the virus establishes entry inside the cell, it replicates [37]. Neurological manifestations of COVID-19 occur due to the presence of ACE-2 receptors in the nervous system and skeletal system. Hematogenous spread, disruption of the blood–brain barrier (BBB), and direct transmission through cranial nerves are all possible entry points to the central nervous system [37]. There are multiple possible means by which COVID-19 affects the nervous system: first, a secondary effect is associated with the vascular and prothrombotic effect of the viral infection on the CNS or PNS vasculature; second, the direct neurotropic or neuro-invasive effect of SARS-CoV-2; third, a secondary effect of the systemic inflammatory responses triggered by the viral infection; lastly, an immune-mediated para-infectious or post-infectious autoimmune effect in response to the viral infection (e.g., GBS) [37, 38].
The US Vaccine Adverse Event Reporting System (VAERS) in adults estimated a crude reporting rate of 1 case of GBS per 100,000 doses administered [39]. However, apart from two pediatric case reports [40, 41], the exact incidence of post-COVID-19 vaccine in the pediatric age group has not been studied. The first case is a 14-year-old child who developed GBS within 1 month of the administration of the second dose of the Pfizer-BioNTech COVID-19 vaccine [40]. The second case is a 16-year-old female who developed GBS 2 days following the Pfizer-BioNTech COVID-19 s dose vaccine [41].
Conclusion
Our case emphasizes the importance of having high index of suspicion of COVID-19-associated Guillain-Barré syndrome even in cases with negative PCR. Prompt treatment is associated with good outcome. Based on our literature review, it seems that post-COVID-19 GBS and the classical GBS are similar in clinical presentation and outcome.
References
https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/transmission_k_12_schools.html, C
Castagnoli R et al (2020) Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children and adolescents: a systematic review. JAMA Pediatr 174(9):882–889
Brodin P (2020) Why is COVID-19 so mild in children? Acta Paediatr 109(6):1082–1083
Lin JE et al (2021) Neurological issues in children with COVID-19. Neurosci Lett 743:135567
Esposito S, Principi N (2021) Multisystem inflammatory syndrome in children related to SARS-CoV-2. Paediatr Drugs 23(2):119–129
Nakra NA et al (2020) Multi-system inflammatory syndrome in children (MIS-C) following SARS-CoV-2 infection: review of clinical presentation, hypothetical pathogenesis, and proposed management. Children (Basel) 7(7)
Guerrero JI et al (2021) Central and peripheral nervous system involvement by COVID-19: a systematic review of the pathophysiology, clinical manifestations, neuropathology, neuroimaging, electrophysiology, and cerebrospinal fluid findings. BMC Infect Dis 21(1):515
LaRovere KL et al (2021) Neurologic involvement in children and adolescents hospitalized in the United States for COVID-19 or multisystem inflammatory syndrome. JAMA Neurol 78(5):536–547
Akçay N et al (2021) Axonal Guillain-Barre syndrome associated with SARS-CoV-2 infection in a child. J Med Virol 93(9):5599–5602
Araújo NM et al (2021) First report of SARS-CoV-2 detection in cerebrospinal fluid in a child with Guillain-Barré syndrome. Pediatr Infect Dis J 40(7):e274–e276
Blanco R, Pichardo J, Abdullah H, Khawaja UA (2021) A rare case of Guillain-Barré syndrome presenting with COVID-19 infection in a six-year-old child. Europ J Neurol
Curtis M et al (2021) Guillain-Barré syndrome in a child with COVID-19 infection. Pediatrics 147(4):e2020015115
Das KY et al (2021) Guillain-Barré syndrome associated with SARS-CoV-2 infection. Indian J Pediatr 88(5):479–479
Declusin A et al (2021) Guillain-Barré syndrome triggered by COVID-19: a pediatric case report and literature review. J Pediat Neurol Neurosci 5(2)
El Mezzeoui S et al (2012) Guillan Barre syndrome in post COVID-19 infection in children. Annals of Medicine and Surgery 2021(67):102524–102524
Frank CH, Almeida TV, Marques EA, de Sousa Monteiro Q, Feitoza PV, Borba MG, Vasconcelos HL, de Souza Bastos M, Lacerda MV (2021) Guillain-Barré syndrome associated with SARS-CoV-2 infection in a pediatric patient. J Trop Pediatr 67(3)
Goel N, Mehndiratta S, Singh A (2021) Post COVID-19 Guillain Barre syndrome in immunocompromised children - a report of two cases and review of literature
Kanou S et al (2022) Guillain-Barre syndrome (GBS) associated with COVID-19 infection that resolved without treatment in a child. BMJ Case Rep 15(3):e245455
Khalifa M et al (2020) Guillain-Barré syndrome associated with severe acute respiratory syndrome coronavirus 2 detection and coronavirus disease 2019 in a child. Journal of the Pediatric Infectious Diseases Society 9(4):510–513
Krishnakumar A et al (2021) Guillain-Barré syndrome with preserved reflexes in a child after COVID-19 infection. Indian J Pediatr 88(8):831–832
Manji HK et al (2020) Guillain-Barré syndrome associated with COVID-19 infection. Pan Afr Med J 35(Suppl 2):118
Meshref M et al (2021) Guillain-Barre syndrome associated with COVID-19 infection: a case report with review of literature. Cureus 13(2):e13096
Mozhdehipanah H, Paybast S, Gorji R (2020) Guillain-Barré syndrome as a neurological complication of COVID-19 infection: a case series and review of the literature. International Clinical Neuroscience Journal 7:156–161
Ray STJ et al (2021) Neurological manifestations of SARS-CoV-2 infection in hospitalised children and adolescents in the UK: a prospective national cohort study. The Lancet Child & Adolescent Health 5(9):631–641
Sánchez-Morales AE et al (2021) Neurological manifestations temporally associated with SARS-CoV-2 infection in pediatric patients in Mexico. Childs Nerv Syst 37(7):2305–2312
Sandoval F et al (2021) Neurologic features associated with SARS-CoV-2 infection in children: a case series report. J Child Neurol 36(10):853–866
Rafiei Tabatabaei S, Shariatpanahi G, Azadkiya R, Karimzadeh P, Karimi A (2021) Guillain-Barre syndrome in a child infected with COVID-19. Arch Pediatr Infect Dis In Press(In Press):e113564
Terencio BBP, Rachelle F, Jamora RDG (2021) Guillain-Barré syndrome in a pediatric patient with COVID-19: a case report and review of literature. Acta Med Philipp
Al Haboob AA (2021) Miller Fischer and posterior reversible encephalopathy syndromes post COVID-19 infection. Neurosciences (Riyadh) 26(3):295–299
Aljomah L et al (2021) Pediatrics COVID-19 and neurological manifestations: single tertiary centre experience. eNeurologicalSci 24:100355
Castro CJ, Enciso HR, Hortiales SS, Durán PX (2021) Miller-Fisher syndrome associated with post-infection by SARS-CoV-2 in a pediatric patient. Rev Latin Infect Pediatr
Raghunathan V et al (2021) Miller Fisher syndrome associated with COVID-19 infection. Pediatr Neurol 123:40
Nguyen TP, Taylor RS, Boyle AG (2022) Guillain Barre syndrome, in StatPearls StatPearls Publishing Copyright ©, StatPearls Publishing LLC.: Treasure Island (FL)
Sidiq Z et al (2020) Benefits and limitations of serological assays in COVID-19 infection. Indian J Tuberc 67(4s):S163-s166
Li YC, Bai WZ, Hashikawa T (2020) The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol 92(6):552–555
Ellul MA et al (2020) Neurological associations of COVID-19. Lancet Neurol 19(9):767–783
Stafstrom CE, Jantzie LL (2020) COVID-19: neurological considerations in neonates and children. Children 7(9):133
Coperchini F et al (2020) The cytokine storm in COVID-19: an overview of the involvement of the chemokine/chemokine-receptor system. Cytokine Growth Factor Rev 53:25–32
Woo EJ et al (2021) Association of receipt of the Ad26.COV2.S COVID-19 vaccine with presumptive Guillain-Barré syndrome, February-July 2021. JAMA 326(16):1606–1613
Malamud E et al (2022) Guillain-Barré syndrome after COVID-19 vaccination in an adolescent. Pediatr Neurol 126:9–10
Kim Y et al (2022) A pediatric case of sensory predominant Guillain-Barré syndrome following COVID-19 vaccination. Child Neurol Open 9:2329048–221074549
Author information
Authors and Affiliations
Contributions
Mira Al Jaberi contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; gave final approval; and accountable for all aspects of the work. Raghad Shihadat contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; gave final approval; and accountable for all aspects of the work. Amira Masri substantially contributed to conception and design; contributed to acquisition, analysis, and interpretation of data; critical review of the manuscript; gave final approval; and accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interest
No funding was received for conducting this study. All authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Al Jaberi, M., Shihadat, R. & Masri, A. Post SARS-CoV-2 Guillain-Barré syndrome in a child: case report and review of the literature. Childs Nerv Syst 38, 2011–2016 (2022). https://doi.org/10.1007/s00381-022-05536-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-022-05536-1