
Abstract
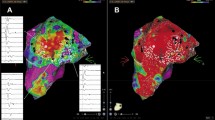
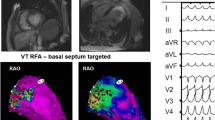
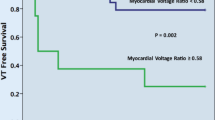
Patients with ischemic and non-ischemic cardiomyopathy often have substrate for ventricular tachycardia (VT) in the endocardium (ENDO), epicardium (EPI), and/or intramural. Although it has been reported that the ENDO unipolar (UNI) voltage map is useful in detecting EPI substrate, its feasibility to detect intramural scarring and its usefulness in radiofrequency catheter ablation (RFCA) remain unclear. To assess the relationship between the left ventricle (LV) ENDO UNI voltage map and the LV EPI bipolar (BIP) voltage map, and to determine the usefulness of the ENDO UNI voltage map to guide RFCA for VT in patients with cardiomyopathy undergoing combined ENDO- and EPI RFCA. Eleven patients with VT undergoing detailed ENDO and EPI electroanatomical mapping of the LV were included (mean age 59 ± 11 years, 9 men). We assessed the value of the LV ENDO UNI voltage map in identifying EPI and/or intramural substrate in these 11 patients with non-ischemic or ischemic cardiomyopathy. The underlying heart disease was dilated cardiomyopathy in 4 patients, cardiac sarcoidosis in 3, hypertrophic cardiomyopathy in 2, and ischemic heart disease in 2 patients. The mean LV ejection fraction was 24 ± 7 %. The low voltage zone (LVZ) was defined as <1.5 mV for LV ENDO BIP electrograms (EGMs), <8.3 mV for LV ENDO UNI EGMs, and <1.0 mV for LV EPI BIP EGMs. The surface area of each LVZ was measured. We also measured the LVZ of the spatial overlap between ENDO UNI and EPI BIP voltage maps using the transparency mode on CARTO software. We performed RFCA at the ENDO and EPI based on activation and/or substrate maps, targeting the LVZ and/or abnormal EGMs. The LVZ was present in the LV ENDO BIP voltage map in 10 of 11 patients (42 ± 33 cm2), and in the LV ENDO UNI voltage map in 10 of 11 patients (72 ± 45 cm2). The LVZ was present in the EPI BIP voltage map in 9 of 11 patients (70 ± 61 cm2), and the LVZ in the ENDO UNI voltage map was also seen in all 9 patients. The location of the LVZ in the EPI BIP map matched that in 45 ± 28 % of ENDO UNI voltage maps. The LVZ in the ENDO UNI voltage map was larger than that in the EPI BIP voltage map in 6 of 11 patients, and RFCA failed in 5 of these 6 patients. In the remaining 5 patients with a smaller LVZ in the ENDO UNI voltage map compared with the EPI BIP voltage map or no LVZ both at ENDO UNI and EPI BIP voltage map, VT was successfully eliminated in 4 of 5 patients. The LV ENDO UNI voltage map is useful in detecting EPI substrate in patients with cardiomyopathy. A larger LVZ in the ENDO UNI voltage map compared to that in the EPI BIP voltage map may indicate the presence of intramural substrate, which leads to difficulty in eliminating VT, even with combined ENDO- and EPI RFCA.




Similar content being viewed by others
References
Nazarian S, Bluemke DA, Lardo AC, Zviman MM, Watkins SP, Dickfeld TL, Meininger GR, Roguin A, Calkins H, Tomaselli GF, Weiss RG, Berger RD, Lima JA, Halperin HR (2005) Magnetic resonance assessment of the substrate for inducible ventricular tachycardia in nonischemic cardiomyopathy. Circulation 112:2821–2825
Cano O, Hutchinson M, Lin D, Garcia F, Zado E, Bala R, Riley M, Cooper J, Dixit S, Gerstenfeld E, Callans D, Marchlinski FE (2009) Electroanatomic substrate and ablation outcome for suspected EPI ventricular tachycardia in left ventricular nonischemic cardiomyopathy. J Am Coll Cardiol 54:799–808
Bogun FM, Desjardins B, Good E, Gupta S, Crawford T, Oral H, Ebinger M, Pelosi F, Chugh A, Jongnarangsin K, Morady F (2009) Delayed-enhanced magnetic resonance imaging in nonischemic cardiomyopathy: utility for identifying the ventricular arrhythmia substrate. J Am Coll Cardiol 53:1138–1145
Sosa E, Scanavacca M, D’avila A, Pilleggi F (1996) A new technique to perform EPI mapping in the electrophysiology laboratory. J Cardiovasc Electrophysiol 7:531–536
Jaïs P, Maury P, Khairy P, Sacher F, Nault I, Komatsu Y, Hocini M, Forclaz A, Jadidi AS, Weerasooryia R, Shah A, Derval N, Cochet H, Knecht S, Miyazaki S, Linton N, Rivard L, Wright M, Wilton SB, Scherr D, Pascale P, Roten L, Pederson M, Bordachar P, Laurent F, Kim SJ, Ritter P, Clementy J, Haïssaguerre M (2012) Elimination of local abnormal ventricular activities: a new end point for substrate modification in patients with scar-related ventricular tachycardia. Circulation 125:2184–2196
Soejima K, Stevenson WG, Sapp JL, Selwyn AP, Couper G, Epstein LM (2004) Endocardial and EPI radiofrequency ablation of ventricular tachycardia associated with dilated cardiomyopathy: the importance of low-voltage scars. J Am Coll Cardiol 43:1834–1842
Hutchinson MD, Gerstenfeld EP, Desjardins B, Bala R, Riley MP, Garcia FC, Dixit S, Lin D, Tzou WS, Cooper JM, Verdino RJ, Callans DJ, Marchlinski FE (2011) Endocardial unipolar voltage mapping to detect EPI ventricular tachycardia substrate in patients with nonischemic left ventricular cardiomyopathy. Circ Arrhythm Electrophysiol 4:49–55
Desjardins B, Yokokawa M, Good E, Crawford T, Latchamsetty R, Jongnarangsin K, Ghanbari H, Oral H, Pelosi F Jr, Chugh A, Morady F, Bogun F (2013) Characteristics of intramural scar in patients with nonischemic cardiomyopathy and relation to intramural ventricular arrhythmias. Circ Arrhythm Electrophysiol 6:891–897
Tokuda M, Tedrow UB, Inada K, Reichlin T, Michaud GF, John RM, Epstein LM, Stevenson WG (2013) Direct comparison of adjacent endocardial and EPI electrograms: implications for substrate mapping. J Am Heart Assoc 2:e000215
Miyamoto K, Noda T, Aiba T, Kusano K (2015) Parasternal intercostal approach, as an alternative to subxiphoid approach for EPI catheter ablation: a case report. Heart Rhythm Case Rep. doi:10.1016/j.hrcr.2014.12.014
Stevenson WG, Khan H, Sager P, Saxon LA, Middlekauff HR, Natterson PD, Wiener I (1993) Identification of reentry circuit sites during catheter mapping and radiofrequency ablation of ventricular tachycardia late after myocardial infarction. Circulation 88:1647–1670
Nakajima K, Miyamoto K, Noda T, Matsuyama T, Kimura Y, Maruyama M, Mishima T, Kanayama J, Kamakura T, Hirose S, Kamijima S, Wada M, Nakajima I, Ishibashi K, Okamura H, Aiba T, Kamakura S, Ueda H, Kusano K (2015) Pathology after combined epi- and endocardial ablation for ventricular tachycardia in a postmortem heart with hypertrophic cardiomyopathy. Heart Rhythm Case Rep. doi:10.1016/j.hrcr.2015.04.003
Nakagawa H, Yamanashi WS, Pitha JV, Arruda M, Wang X, Ohtomo K, Beckman KJ, McClelland JH, Lazzara R, Jackman WM (1995) Comparison of in vivo tissue temperature profile and lesion geometry for radiofrequency ablation with a saline-irrigated electrode versus temperature control in a canine thigh muscle preparation. Circulation 91:2264–2273
Fenelon G, Pereira KP, de Paola AA (2006) EPI radiofrequency ablation of ventricular myocardium: factors affecting lesion formation and damage to adjacent structures. J Interv Card Electrophysiol 15:57–63
Codreanu A, Odille F, Aliot E, Marie PY, Magnin-Poull I, Andronache M, Mandry D, Djaballah W, R_egent D, Felblinger J, de Chillou C (2008) Electroanatomic characterization of post-infarct scars comparison with 3-dimensional myocardial scar reconstruction based on magnetic resonance imaging. J Am Coll Cardiol 52:839–842
Wijnmaalen AP, van der Geest RJ, van Hulsvan Taxis CF, Siebelink HM, Kroft LJ, Bax JJ, Reiber JH, Schalij MJ, Zeppenfeld K (2011) Head-to-head comparison of contrast-enhanced magnetic resonance imaging and electroanatomical voltage mapping to assess post-infarct scar characteristics in patients with ventricular tachycardias: real-time image integration and reversed registration. Eur Heart J 32:104–114
Funada A, Kanzaki H, Noguchi T, Morita Y, Sugano Y, Ohara T, Hasegawa T, Hashimura H, Ishibashi-Ueda H, Kitakaze M, Yasuda S, Ogawa H, Anzai T (2015) Prognostic significance of late gadolinium enhancement quantification in cardiac magnetic resonance imaging of hypertrophic cardiomyopathy with systolic dysfunction. Heart Vessels. doi:10.1007/s00380-015-0697-6
Hen Y, Iguchi N, Machida H, Takada K, Utanohara Y, Sumiyoshi T (2013) High signal intensity on T2-weighted cardiac magnetic resonance imaging correlates with the ventricular tachyarrhythmia in hypertrophic cardiomyopathy. Heart Vessels 28:742–749
Nabeta T, Inomata T, Iida Y, Ikeda Y, Iwamoto M, Ishii S, Sato T, Watanabe I, Naruke T, Shinagawa H, Koitabashi T, Takeuchi I, Nishii M, Inoue Y, Izumi T (2014) Baseline cardiac magnetic resonance imaging versus baseline endomyocardial biopsy for the prediction of left ventricular reverse remodeling and prognosis in response to therapy in patients with idiopathic dilated cardiomyopathy. Heart Vessels 29:784–792
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Miyamoto, K., Noda, T., Satomi, K. et al. Larger low voltage zone in endocardial unipolar map compared with that in epicardial bipolar map indicates difficulty in eliminating ventricular tachycardia by catheter ablation. Heart Vessels 31, 1337–1346 (2016). https://doi.org/10.1007/s00380-015-0732-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-015-0732-7