
Abstract
Purpose
The rates of complications following radical/partial nephrectomy (RN/PN) are well known; however, the data regarding timing are opaque. Accordingly, we sought to assess the median time-to-event for 19 principal postoperative complications within 30 days following surgery.
Methods
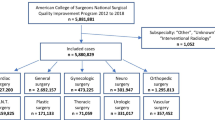
Patients undergoing RN/PN were identified within the American College of Surgeons National Surgical Quality Improvement Program database (2005–2011). Primary endpoint was time-to-complication. Secondary endpoints included length-of-stay (LOS), re-intervention, re-admission and 30-day mortality. Multivariable regression models assessed the predictors for pre-/post-discharge complications and the effect of time-to-complication on secondary outcomes.
Results
Overall, 3820 patients underwent nephrectomy (RN = 63.6 %). The overall complication rate was 16.8 %, and the median LOS was 4 days. The majority of major complications (88.1 %), including bleeding/transfusion, renal, septic, deep venous thrombosis or pulmonary embolism, pulmonary, cardiac and neurologic, occurred prior to discharge. Conversely, the relatively minor complications, including wound and urinary tract infections, occurred predominantly post-discharge (70.7 %). The median time to major complications was 3 versus 13 days for minor complications. In multivariable analyses, age [odds ratio (OR) 1.02, p < 0.001], American Society of Anesthesiologists score ≥ 2 (p < 0.01) and PN (p < 0.001) were predictors of pre-discharge complications, while female gender (OR 1.67, p < 0.001), hypertension (OR 1.28, p = 0.007) and diabetes (OR 1.48, p < 0.001) were predictors of post-discharge complications. Creatinine ≥ 1.2 mg/dl and hematocrit < 30 increased (p < 0.01), whereas a minimally invasive approach decreased the odds (p < 0.05) for both pre-/post-discharge complications. For a given complication, time-to-complication did not affect the odds for mortality (p = 0.343) or re-intervention (p = 0.872).
Conclusions
Approximately one in six patients suffers a complication following RN/PN; major complications tend to occur early with the majority occurring pre-discharge. Knowledge regarding the timing and risk factors for complications may facilitate improved patient–physician communication, both at admission and at discharge.

Similar content being viewed by others


References
Siegel R, Ma J, Zou Z, Jemal A (2014) Cancer statistics, 2014. CA Cancer J Clin 64:9–29
Pahernik S, Roos F, Hampel C, Gillitzer R, Melchior SW, Thuroff JW (2006) Nephron sparing surgery for renal cell carcinoma with normal contralateral kidney: 25 years of experience. J Urol 175:2027–2031
Motzer RJ, Jonasch E, Agarwal N, Beard C, Bhayani S, Bolger GB et al (2014) Kidney cancer, version 2.2014. J Nat Compr Cancer Netw 12:175–182
Zargar H, Allaf M, Bhayani S, Stifelman M, Rogers C, Ball M, Larson J, Marshall S, Kumar R, Kaouk J (2014) Trifecta and optimal peri-operative outcomes of robotic and laparoscopic partial nephrectomy in surgical treatment of small renal masses: a multi-institutional study. BJU int. doi:10.1111/bju.12933
Ghani KR, Sukumar S, Sammon JD, Rogers CG, Trinh QD, Menon M (2014) Practice patterns and outcomes of open and minimally invasive partial nephrectomy since the introduction of robotic partial nephrectomy: results from the nationwide inpatient sample. J Urol 191:907–912
Corman JM, Penson DF, Hur K, Khuri SF, Daley J, Henderson W et al (2000) Comparison of complications after radical and partial nephrectomy: results from the National Veterans Administration Surgical Quality Improvement Program. BJU Int 86:782–789
Abbou CC, Cicco A, Gasman D, Hoznek A, Antiphon P, Chopin DK et al (1999) Retroperitoneal laparoscopic versus open radical nephrectomy. J Urol 161:1776–1780
Kazaure HS, Roman SA, Sosa JA (2012) Association of postdischarge complications with reoperation and mortality in general surgery. Arch Surg 147:1000–1007
Morris MS, Deierhoi RJ, Richman JS, Altom LK, Hawn MT (2014) The relationship between timing of surgical complications and hospital readmission. JAMA Surg 149:348–354
Lawson EH, Hall BL, Louie R, Ettner SL, Zingmond DS, Han L et al (2013) Association between occurrence of a postoperative complication and readmission: implications for quality improvement and cost savings. Ann Surg 258:10–18
Bilimoria KY, Cohen ME, Ingraham AM, Bentrem DJ, Richards K, Hall BL et al (2010) Effect of postdischarge morbidity and mortality on comparisons of hospital surgical quality. Ann Surg 252:183–190
Wakeam E, Hyder JA, Tsai TC, Lipsitz SR, Orgill DP, Finlayson SR (2015) Complication timing and association with mortality in the American College of Surgeons’ National Surgical Quality Improvement Program database. J Surg Res 193(1):77–87
American College of Surgeons (2012) American College of Surgeons National Surgical Quality Improvement Project: User Guide for the 2011 Participant Use Data File
Henderson WG, Daley J (2009) Design and statistical methodology of the National Surgical Quality Improvement Program: why is it what it is? Am J Surg 198(5 Suppl):S19–S27
Bhojani N, Gandaglia G, Sood A, Rai A, Pucheril D, Chang SL et al (2014) Morbidity and mortality after benign prostatic hyperplasia surgery: data from the American College of Surgeons National Surgical Quality Improvement Program. J Endourol
Massie AB, Kuricka LM, Segev DL (2014) Big data in organ transplantation: registries and administrative claims. Am J Transplant 14:1723–1730
Schroeck FR, Krupski TL, Sun L, Albala DM, Price MM, Polascik TJ et al (2008) Satisfaction and regret after open retropubic or robot-assisted laparoscopic radical prostatectomy. Eur Urol 54:785–793
Engel H, Huang JJ, Tsao CK, Lin CY, Chou PY, Brey EM et al (2011) Remote real-time monitoring of free flaps via smartphone photography and 3G wireless Internet: a prospective study evidencing diagnostic accuracy. Microsurgery 31:589–595
Murphy RX Jr, Bain MA, Wasser TE, Wilson E, Okunski WJ (2006) The reliability of digital imaging in the remote assessment of wounds: defining a standard. Ann Plast Surg 56:431–436
Varkey P, Tan NC, Girotto R, Tang WR, Liu YT, Chen HC (2008) A picture speaks a thousand words: the use of digital photography and the Internet as a cost-effective tool in monitoring free flaps. Ann Plast Surg 60:45–48
Graham J, Tomcavage J, Salek D, Sciandra J, Davis DE, Stewart WF (2012) Postdischarge monitoring using interactive voice response system reduces 30-day readmission rates in a case-managed Medicare population. Med Care 50:50–57
Tuggle CT, Park LS, Roman S, Udelsman R, Sosa JA (2010) Rehospitalization among elderly patients with thyroid cancer after thyroidectomy are prevalent and costly. Ann Surg Oncol 17:2816–2823
Robles L, Slogoff M, Ladwig-Scott E, Zank D, Larson MK, Aranha G et al (2011) The addition of a nurse practitioner to an inpatient surgical team results in improved use of resources. Surgery 150:711–717
Maniar HS, Bell JM, Moon MR, Meyers BF, Marsala J, Lawton JS et al (2014) Prospective evaluation of patients readmitted after cardiac surgery: analysis of outcomes and identification of risk factors. J Thorac Cardiovasc Surg 147:1013–1018
Chong TW, Chan G, Feng L, Goh S, Hew A, Ng TP et al (2013) Integrated care pathway for hip fractures in a subacute rehabilitation setting. Ann Acad Med Singap 42:579–584
Trinh QD, Schmitges J, Sun M, Sammon J, Shariat SF, Zorn K et al (2012) Morbidity and mortality of radical prostatectomy differs by insurance status. Cancer 118:1803–1810
Pierorazio PM, Hyams ES, Lin BM, Mullins JK, Allaf ME (2012) Laparoscopic radical nephrectomy for large renal masses: critical assessment of perioperative and oncologic outcomes of stage T2a and T2b tumors. Urology 79:570–575
Kutikov A, Uzzo RG (2009) The R.E.N.A.L. nephrometry score: a comprehensive standardized system for quantitating renal tumor size, location and depth. J Urol 182:844–853
Trinh QD, Sun M, Kim SP, Sammon J, Kowalczyk KJ, Friedman AA et al (2014) The impact of hospital volume, residency, and fellowship training on perioperative outcomes after radical prostatectomy. Urol Oncol 32(29):e13–e20
Trinh QD, Bjartell A, Freedland SJ, Hollenbeck BK, Hu JC, Shariat SF et al (2013) A systematic review of the volume-outcome relationship for radical prostatectomy. Eur Urol 64:786–798
Acknowledgments
Quoc-Dien Trinh is supported by the Professor Walter Morris-Hale Distinguished Chair in Urologic Oncology at Brigham and Women’s Hospital; the American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS-NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Conflict of interest
None.
Ethical standard
The manuscript does not contain clinical studies or patient data.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sood, A., Abdollah, F., Sammon, J.D. et al. An evaluation of the timing of surgical complications following nephrectomy: data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP). World J Urol 33, 2031–2038 (2015). https://doi.org/10.1007/s00345-015-1564-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-015-1564-x