
Abstract
Objectives
To evaluate the diagnostic performance of 1.5-T non-contrast MR coronary angiography (MRCA) for detection of coronary artery disease (CAD) using whole-heart imaging combined with volume-targeted imaging.
Methods
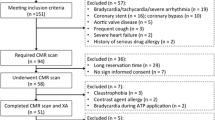
Forty-five patients scheduled for conventional coronary angiography (CAG) underwent 1.5-T free-breathing non-contrast steady-state free-precession MRCA, including whole-heart and subsequent three-vessel volume-targeted imaging. Coronary stenosis was evaluated as follows: (1) by whole-heart MRCA alone; (2) by combined MRCA (whole-heart plus volume-targeted images). The diagnostic performance for significant stenosis (≥ 50% diameter reduction) was evaluated and compared using CAG as a reference standard.
Results
Combined MRCA was completed in all 45 patients with a total acquisition time of 16.6 ± 3.3 min. The sensitivity, specificity, and accuracy of combined MRCA per patient were 97% (95% confidence interval 84–100%), 83% (52–98%), and 93% (82–98%), respectively. The areas under the receiver operating characteristic curve of combined MRCA were significantly higher than those of whole-heart MRCA on a per patient (0.97 versus 0.85, p = 0.0078) and per vessel (0.96 versus 0.86, p < 0.0001) basis. Compared with whole-heart MRCA, combined MRCA showed equally high sensitivity but significantly improved specificity on a per patient (83% versus 25%, p = 0.016) and per vessel (85% versus 50%, p < 0.0001) basis.
Conclusions
1.5-T non-contrast MRCA combining whole-heart and volume-targeted imaging can detect significant CAD with high sensitivity and moderate specificity. Combined MRCA significantly improves specificity compared with whole-heart imaging alone.
Key Points
• 1.5-T non-contrast MRCA with combined whole-heart and volume-targeted imaging can detect CAD with high sensitivity and moderate specificity comparable with coronary CTA.
• Compared with whole-heart imaging alone, combined imaging provides improved diagnostic accuracy, especially specificity.




Similar content being viewed by others


Abbreviations
- AUC:
-
Area under the ROC curve
- CABG:
-
Coronary artery bypass graft
- CAD:
-
Coronary artery disease
- CAG:
-
Conventional coronary angiography
- CI:
-
Confidence intervals
- CTA:
-
CT angiography
- CTO:
-
Chronic total occlusion
- FH:
-
Feet-to-head
- LAD:
-
Left anterior descending
- LCX:
-
Left circumflex
- MIP:
-
Maximum intensity projection
- MRCA:
-
MR coronary angiography
- NPV:
-
Negative predictive value
- PPV:
-
Positive predictive value
- RCA:
-
Right coronary artery
- RL:
-
Right-left
- ROC:
-
Receiver operating characteristic
- SPIR:
-
Spectral presaturation with inversion recovery
- SSFP:
-
Steady-state free-precession
- VR:
-
Volume rendering
References
Virani SS, Alonso A, Benjamin EJ et al (2020) Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. https://doi.org/10.1161/CIR.0000000000000757:CIR0000000000000757
Knuuti J, Wijns W, Saraste A et al (2020) 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 41:407–477
American College of Cardiology Foundation Task Force on Expert Consensus Documents, Hundley WG, Bluemke DA et al (2010) ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol 55:2614–2662
Di Leo G, Fisci E, Secchi F et al (2016) Diagnostic accuracy of magnetic resonance angiography for detection of coronary artery disease: a systematic review and meta-analysis. Eur Radiol 26:3706–3718
Pouleur AC, le Polain de Waroux JB, Kefer J, Pasquet A, Vanoverschelde JL, Gerber BL (2008) Direct comparison of whole-heart navigator-gated magnetic resonance coronary angiography and 40- and 64-slice multidetector row computed tomography to detect the coronary artery stenosis in patients scheduled for conventional coronary angiography. Circ Cardiovasc Imaging 1:114–121
Sakuma H, Ichikawa Y, Chino S, Hirano T, Makino K, Takeda K (2006) Detection of coronary artery stenosis with whole-heart coronary magnetic resonance angiography. J Am Coll Cardiol 48:1946–1950
Nagata M, Kato S, Kitagawa K et al (2011) Diagnostic accuracy of 1.5-T unenhanced whole-heart coronary MR angiography performed with 32-channel cardiac coils: initial single-center experience. Radiology 259:384–392
Kato S, Kitagawa K, Ishida N et al (2010) Assessment of coronary artery disease using magnetic resonance coronary angiography: a national multicenter trial. J Am Coll Cardiol 56:983–991
Jin H, Zeng MS, Ge MY, Yun H, Yang S (2013) 3D coronary MR angiography at 1.5 T: volume-targeted versus whole-heart acquisition. J Magn Reson Imaging 38:594–602
Bi X, Deshpande V, Carr J, Li D (2006) Coronary artery magnetic resonance angiography (MRA): a comparison between the whole-heart and volume-targeted methods using a T2-prepared SSFP sequence. J Cardiovasc Magn Reson 8:703–707
Chang S, Cham MD, Hu S, Wang Y (2008) 3-T navigator parallel-imaging coronary MR angiography: targeted-volume versus whole-heart acquisition. AJR Am J Roentgenol 191:38–42
Leipsic J, Abbara S, Achenbach S et al (2014) SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr 8:342–358
Pang J, Bhat H, Sharif B et al (2014) Whole-heart coronary MRA with 100% respiratory gating efficiency: self-navigated three-dimensional retrospective image-based motion correction (TRIM). Magn Reson Med 71:67–74
Yonezawa M, Nagata M, Kitagawa K et al (2014) Quantitative analysis of 1.5-T whole-heart coronary MR angiograms obtained with 32-channel cardiac coils: a comparison with conventional quantitative coronary angiography. Radiology 271:356–364
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44:837–845
Knuuti J, Ballo H, Juarez-Orozco LE et al (2018) The performance of non-invasive tests to rule-in and rule-out significant coronary artery stenosis in patients with stable angina: a meta-analysis focused on post-test disease probability. Eur Heart J 39:3322–3330
Kim WY, Danias PG, Stuber M et al (2001) Coronary magnetic resonance angiography for the detection of coronary stenoses. N Engl J Med 345:1863–1869
Nakamura M, Kido T, Kido T et al (2018) Non-contrast compressed sensing whole-heart coronary magnetic resonance angiography at 3T: a comparison with conventional imaging. Eur J Radiol 104:43–48
Hirai K, Kido T, Kido T et al (2020) Feasibility of contrast-enhanced coronary artery magnetic resonance angiography using compressed sensing. J Cardiovasc Magn Reson 22:15
He Y, Pang J, Dai Q, Fan Z, An J, Li D (2016) Diagnostic performance of self-navigated whole-heart contrast-enhanced coronary 3-T MR angiography. Radiology 281:401–408
Liu X, Zhao X, Huang J et al (2007) Comparison of 3D free-breathing coronary MR angiography and 64-MDCT angiography for detection of coronary stenosis in patients with high calcium scores. AJR Am J Roentgenol 189:1326–1332
Xie Y, Kim YJ, Pang J et al (2017) Coronary atherosclerosis T1-weighed characterization with integrated anatomical reference: comparison with high-risk plaque features detected by invasive coronary imaging. JACC Cardiovasc Imaging 10:637–648
Zhang L, Song X, Dong L et al (2018) Additive value of 3T cardiovascular magnetic resonance coronary angiography for detecting coronary artery disease. J Cardiovasc Magn Reson 20:29
Windecker S, Kolh P, Alfonso F et al (2014) 2014 ESC/EACTS guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 35:2541–2619
Kim RJ, Wu E, Rafael A et al (2000) The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med 343:1445–1453
Nagel E, Greenwood JP, McCann GP et al (2019) Magnetic resonance perfusion or fractional flow reserve in coronary disease. N Engl J Med 380:2418–2428
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 81873891, for Yi-Ning Wang), the National Key R&D Program during the 13th Five-Year period (Grant No. 2016YFC1300402, for Yi-Ning Wang and Zheng-Yu Jin), the Non-profit Central Research Institute Fund of the Chinese Academy of Medical Sciences (Grant No. 2018RC320004, for Yi-Ning Wang), and the Fundamental Research Funds for the Central Universities of the Peking Union Medical College (Grant No. 3332020008, for Lu Lin).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Guarantor
The scientific guarantor of this publication is Zheng-Yu Jin.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Ethical approval
The study was approved by the Institutional Review Board of Peking Union Medical College Hospital, Beijing, China.
Informed consent
Written informed consent was obtained from all patients in this study.
Methodology
• prospective
• diagnostic study
• performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Yining Wang is the first corresponding author and Zheng-Yu Jin is the second corresponding author of this work.
Rights and permissions
About this article

Cite this article
Lin, L., Wang, L., Zhang, XN. et al. A clinical strategy to improve the diagnostic accuracy of 1.5-T non-contrast MR coronary angiography for detection of coronary artery disease: combination of whole-heart and volume-targeted imaging. Eur Radiol 31, 1894–1904 (2021). https://doi.org/10.1007/s00330-020-07135-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-020-07135-7