
Abstract
Objective
To compare imaging findings with histopathology in AML without visible fat (AMLwvf).
Material and methods
With IRB approval, we identified 18 AMLwvf that underwent CT between 2002-2014. A radiologist measured NECT-attenuation, corticomedullary (CM) and nephrographic (NG) enhancement, echogenicity relative to renal cortex (RC) (N = 5), T2W (T2AML/T2RC) signal-intensity (SI), and chemical-shift SI ([SIIN-PHASE − SIOPPOSED-PHASE]/SIIN-PHASE) indices (N = 6). A pathologist re-evaluated 15/18 AMLwvf for 1) < or > 25 % adipocytes/high-power-field (HPF), 2) “many or few” blood vessels. Comparisons were performed using chi-square and independent t-tests.
Results
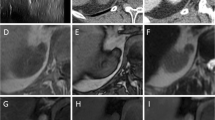
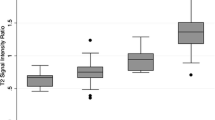
73.3 %(11/15) of AMLwvf had <25 % adipocytes/HPF and 86.7 %(13/15) had “many” blood vessels. NECT-attenuation was 41.8(±6.9) HU. 61.1 %(11/18) of AMLwvf were hyper-attenuating and 38.9 %(7/18) iso-attenuating; attenuation was associated with %-adipocytes/HPF, (p = 0.01). CM/NG enhancement were 63.3(±20.8)/51.7(±15.5) HU. 72.2 %(13/18) of AMLwvf had wash-out enhancement, with no association with amount of blood vessels at pathology, (p = 0.68). No difference in echogenicity was noted by histology (p > 0.05). All AMLwvf were T2-hypointense (SI ratio = 0.61 [±0.1]). 2/6 AMLwvf showed SI drop on chemical-shift MRI; both were iso-attenuating and were associated with >25 % adipocytes/HPF (p = 0.04).
Conclusions
AMLwvf are typically T2-hypointense and hyper-attenuating with wash-out enhancement due to abundant smooth muscle and vessels respectively. Iso-attenuating AMLwvf with microscopic fat on MRI contain more adipocytes/HPF.
Key Points
• Five percent of AML do not demonstrate detectable fat on imaging
• These AML are hyperattenuating and T2-hypointense due to abundant smooth muscle
• These AML show washout enhancement without association to vessel count at histopathology
• Iso-attenuating AML with microscopic fat on MRI show >25 % adipocytes/HPF
• The term “AML without visible fat” is proposed to reduce ambiguity





Similar content being viewed by others

References
Eble JN SG, Epstein JI, Sesterhenn IA (2004) World Health Organization classification of tumors: Pathology and genetics of tumors of the urinary system and male genital organs. . Lyon, Fr. Available via http://www.iarc.fr/en/publications/pdfs-online/pat-gen/bb7/BB7.pdf2013
Bissler JJ, Kingswood JC (2004) Renal angiomyolipomata. Kidney Int 66:924–934
Schieda N, Kielar AZ, Al Dandan O, McInnes MD, Flood TA (2015) Ten uncommon and unusual variants of renal angiomyolipoma (AML): radiologic-pathologic correlation. Clin Radiol 70(2):206–220
Schieda N, Avruch L, Flood TA (2014) Small (<1 cm) incidental echogenic renal cortical nodules: chemical shift MRI outperforms CT for confirmatory diagnosis of angiomyolipoma (AML). Insights Imaging 5(3):295–299
Schieda N, Hodgdon T, El-Khodary M, Flood TA, McInnes MD (2014) Unenhanced CT for the Diagnosis of Minimal-Fat Renal Angiomyolipoma. AJR Am J Roentgenol 203:1236–1241
Remzi M, Ozsoy M, Klingler HC et al (2006) Are small renal tumors harmless? Analysis of histopathological features according to tumors 4 cm or less in diameter. J Urol 176:896–899
Violette P, Abourbih S, Szymanski KM et al (2012) Solitary solid renal mass: can we predict malignancy? BJU Int 110:E548–E552
Sant GR, Heaney JA, Ucci AA Jr, Sarno RC, Meares EM Jr (1984) Computed tomographic findings in renal angiomyolipoma: an histologic correlation. Urology 24:293–296
Jinzaki M, Tanimoto A, Narimatsu Y et al (1997) Angiomyolipoma: imaging findings in lesions with minimal fat. Radiology 205:497–502
Kim JK, Kim SH, Jang YJ et al (2006) Renal angiomyolipoma with minimal fat: differentiation from other neoplasms at double-echo chemical shift FLASH MR imaging. Radiology 239:174–180
Kim JK, Park SY, Shon JH, Cho KS (2004) Angiomyolipoma with minimal fat: differentiation from renal cell carcinoma at biphasic helical CT. Radiology 230:677–684
Kim JY, Kim JK, Kim N, Cho KS (2008) CT histogram analysis: differentiation of angiomyolipoma without visible fat from renal cell carcinoma at CT imaging. Radiology 246:472–479
Simpfendorfer C, Herts BR, Motta-Ramirez GA et al (2009) Angiomyolipoma with minimal fat on MDCT: can counts of negative-attenuation pixels aid diagnosis? AJR Am J Roentgenol 192:438–443
Hindman N, Ngo L, Genega EM et al (2012) Angiomyolipoma with minimal fat: can it be differentiated from clear cell renal cell carcinoma by using standard MR techniques? Radiology 265:468–477
Zhang YY, Luo S, Liu Y, Xu RT (2013) Angiomyolipoma with minimal fat: differentiation from papillary renal cell carcinoma by helical CT. Clin Radiol 68:365–370
Chaudhry HS, Davenport MS, Nieman CM, Ho LM, Neville AM (2012) Histogram analysis of small solid renal masses: differentiating minimal fat angiomyolipoma from renal cell carcinoma. AJR Am J Roentgenol 198:377–383
Jinzaki M, Silverman SG, Akita H, Nagashima Y, Mikami S, Oya M (2014) Renal angiomyolipoma: a radiological classification and update on recent developments in diagnosis and management. Abdom Imaging 39:588–604
Yang CW, Shen SH, Chang YH et al (2013) Are there useful CT features to differentiate renal cell carcinoma from lipid-poor renal angiomyolipoma? AJR Am J Roentgenol 201:1017–1028
Milner J, McNeil B, Alioto J et al (2006) Fat poor renal angiomyolipoma: patient, computerized tomography and histological findings. J Urol 176:905–909
Jinzaki M, Silverman SG, Akita H, Nagashima Y, Mikami S, Oya M (2014) Renal angiomyolipoma: a radiological classification and update on recent developments in diagnosis and management. Abdom Imaging 39(3):588–604
Pusiol T, Piscioli I, Morini A, Pedrosa I, Rofsky NM (2013) Discordance about the use of the term minimal fat angiomyolipoma. Radiology 267:656–657
Pusiol T, Piscioli I, Scialpi M (2013) Minimal fat angiomyolipoma: a controversial subtype of classic angiomyolipoma. AJR Am J Roentgenol 201:W359
Davenport MS, Neville AM, Ellis JH, Cohan RH, Chaudhry HS, Leder RA (2011) Diagnosis of renal angiomyolipoma with Hounsfield unit thresholds: effect of size of region of interest and nephrographic phase imaging. Radiology 260:158–165
Pierorazio PM, Hyams ES, Tsai S et al (2013) Multiphasic enhancement patterns of small renal masses (</=4 cm) on preoperative computed tomography: utility for distinguishing subtypes of renal cell carcinoma, angiomyolipoma, and oncocytoma. Urology 81:1265–1271
Lee-Felker SA, Felker ER, Tan N et al (2014) Qualitative and quantitative MDCT features for differentiating clear cell renal cell carcinoma from other solid renal cortical masses. AJR Am J Roentgenol 203:W516–W524
Siegel CL, Middleton WD, Teefey SA, McClennan BL (1996) Angiomyolipoma and renal cell carcinoma: US differentiation. Radiology 198:789–793
Farrelly C, Delaney H, McDermott R, Malone D (2008) Do all non-calcified echogenic renal lesions found on ultrasound need further evaluation with CT? Abdom Imaging 33:44–47
Sasiwimonphan K, Takahashi N, Leibovich BC, Carter RE, Atwell TD, Kawashima A (2012) Small (<4 cm) renal mass: differentiation of angiomyolipoma without visible fat from renal cell carcinoma utilizing MR imaging. Radiology 263:160–168
Karlo CA, Donati OF, Burger IA et al (2013) MR imaging of renal cortical tumours: qualitative and quantitative chemical shift imaging parameters. Eur Radiol 23:1738–1744
Ramamurthy NK, Moosavi B, McInnes MD, Flood TA, Schieda N (2015) Multiparametric MRI of solid renal masses: pearls and pitfalls. Clin Radiol 70(3):304–16
Chung MS, Choi HJ, Kim MH, Cho KS (2014) Comparison of t2-weighted MRI with and without fat suppression for differentiating renal angiomyolipomas without visible fat from other renal tumors. AJR Am J Roentgenol 202:765–771
Choi HJ, Kim JK, Ahn H, Kim CS, Kim MH, Cho KS (2011) Value of T2-weighted MR imaging in differentiating low-fat renal angiomyolipomas from other renal tumors. Acta Radiol 52:349–353
Ferre R, Cornelis F, Verkarre V, et al (2015) Double-echo gradient chemical shift MR imaging fails to differentiate minimal fat renal angiomyolipomas from other homogeneous solid renal tumors. Eur J Radiol 84(3):360–365
Hodgdon T, McInnes MD, Schieda N, Flood TA, Lamb L, Thornhill RE (2015) Can Quantitative CT Texture Analysis be Used to Differentiate Fat-poor Renal Angiomyolipoma from Renal Cell Carcinoma on Unenhanced CT Images? Radiology:142215
Pedrosa I, Sun MR, Spencer M et al (2008) MR imaging of renal masses: correlation with findings at surgery and pathologic analysis. Radiographics 28:985–1003
Campbell N, Rosenkrantz AB, Pedrosa I (2014) MRI phenotype in renal cancer: is it clinically relevant? Top Magn Reson Imaging 23:95–115
Schieda N vdPC, Moosavi B, McInnes MDF, Mai KT, Flood TA (2015) Intracellular lipid in papillary renal cell carcinoma (RCC) at chemical-shift MRI: Radiologic-Pathologic correlation. Eur Radiol. doi:10.1007/s00330-015-3610-x
Cornelis F, Tricaud E, Lasserre AS et al (2014) Routinely performed multiparametric magnetic resonance imaging helps to differentiate common subtypes of renal tumours. Eur Radiol 24:1068–1080
Lassel EA, Rao R, Schwenke C, Schoenberg SO, Michaely HJ (2014) Diffusion-weighted imaging of focal renal lesions: a meta-analysis. Eur Radiol 24:241–249
Tanaka H, Yoshida S, Fujii Y et al (2011) Diffusion-weighted magnetic resonance imaging in the differentiation of angiomyolipoma with minimal fat from clear cell renal cell carcinoma. Int J Urol 18:727–730
Acknowledgments
The scientific guarantor of this publication is Nicola Schieda, MD FRCP(C). The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. One of the authors has significant statistical expertise. Institutional review board approval was obtained. Written informed consent was waived by the institutional review board. Methodology: retrospective, cross-sectional study, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Hakim, S.W., Schieda, N., Hodgdon, T. et al. Angiomyolipoma (AML) without visible fat: Ultrasound, CT and MR imaging features with pathological correlation. Eur Radiol 26, 592–600 (2016). https://doi.org/10.1007/s00330-015-3851-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-015-3851-8