
Abstract
Purpose
Minimally invasive alternatives to transurethral resection of the prostate (TURP) such as prostate arterial embolization (PAE) and photoselective vaporization of the prostate (PVP) are being explored as adjuncts in the care of patients with benign prostatic hyperplasia. However, there are conflicting reports of the costs of these procedures. The purpose of this study was to compare the direct and indirect hospital costs of TURP, PAE and PVP.
Materials and Methods
A chart review was performed in patients who underwent TURP, PVP and PAE from April 2015 to March 2017. All hospital costs were collected in accordance with the Ontario Case Costing Initiative, a standardized medical case costing system. Costs were characterized as direct or indirect and fixed or variable. Probabilistic sensitivity analysis was conducted to study cost uncertainty.
Results
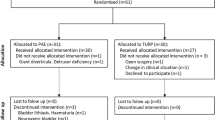
During the study period, a total of 209 men underwent TURP, 28 PVP and 21 PAE. Mean age (years) was as follows: TURP 71.43; PVP 73.66; PAE 70.77 (p = 0.366). Mean length of stay (days) was as follows: TURP 1.63; PVP 1.55; PAE 1 (p = 0.076). Total costs of the PAE group ($3829, SD $1582) were less than both PVP ($5719, SD $1515) and TURP groups ($5034, SD $1997, p < 0.001). There was no significant difference in direct costs between the groups. Monte Carlo simulation demonstrated that PAE was the least costly alternative majority of the time.
Conclusions
The total hospital costs of PAE at our institution are significantly lower than those of PVP and TURP.

Adapted from “Hospital Production Function Model,” Ontario Case Costing Guide, Ministry of Health and Long-Term Care




Similar content being viewed by others


Change history
02 January 2019
The original version of this article published previously contained an error.
References
Getzenberg RH, Kulkarni P. Etiology and pathogenesis. In: Kaplan SA, McVary KT, editors. Male lower urinary tract symptoms and benign prostatic hyperplasia. Chichester: Wiley; 2014. p. 218.
McConnell JD, Barry MJ, Bruskewitz RC. Benign prostatic hyperplasia: diagnosis and treatment. Agency for health care policy and research. Clin Pract Guidel Quick Ref Guide Clin. 1994;8:1–17.
Chapple CR. Lower urinary tract symptoms suggestive of benign prostatic obstruction–Triumph: design and implementation. Eur Urol. 2001;39(Suppl. 3):31–6.
Taub DA, Wei JT. The economics of benign prostatic hyperplasia and lower urinary tract symptoms in the United States. Curr Urol Rep. 2006;7:272–81.
Hueber PA, Zorn KC. Canadian trend in surgical management of benign prostatic hyperplasia and laser therapy from 2007–2008 to 2011–2012. Can Urol Assoc J. 2013;7(9–10):e582–6.
Borboroglu PG, Kane CJ, Ward JF, Roberts JL, Sands JP. Immediate and postoperative complications of transurethral prostatectomy in the 1990s. J Urol. 1999;162(4):1307–10.
Rassweiler J, Teber D, Kuntz R, Hofmann R. Complications of transurethral resection of the prostate (TURP)—incidence, management, and prevention. Eur Urol. 2006;50(5):969–79.
Wasson JH, Reda DJ, Bruskewitz RC, Elinson J, Keller AM, Henderson WG. A comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia. N Engl J Med. 1995;332(2):75–9.
Madersbacher S, Lackner J, Brössner C, et al. Reoperation, myocardial infarction and mortality after transurethral and open prostatectomy: a nation-wide, long-term analysis of 23,123 cases. Eur Urol. 2005;47(4):499–504.
Al-Ansari A, Younes N, Sampige VP, et al. GreenLight HPS 120-W laser vaporization versus transurethral resection of the prostate for treatment of benign prostatic hyperplasia: a randomized clinical trial with midterm follow-up. Eur Urol. 2010;58:349–55.
Bouchier-Hayes DM, Van AS, Bugeja P, et al. A randomized trial of photoselective vaporization of the prostate using the 80-W potassium-titanyl-phosphate laser vs transurethral prostatectomy, with a 1-year follow-up. BJU Int. 2010;105:964–9.
Capitan C, Blazquez C, Martin MD, et al. GreenLight HPS 120-W laser vaporization versus transurethral resection of the prostate for the treatment of lower urinary tract symptoms due to benign prostatic hyperplasia: a randomized clinical trial with 2-year follow-up. Eur Urol. 2011;60:734–9.
Goh AC, Gonzalez RR. Photoselective laser vaporization prostatectomy versus transurethral prostate resection: a cost analysis. J Urol. 2010;183:1469–73.
Liatsikos E, Kyriazis I, Kallidonis P, et al. Photoselective GreenLight laser vaporization versus transurethral resection of the prostate in Greece: a comparative cost analysis. J Endourol. 2012;26:168–73.
Whelan A. Prospective trial of GreenLight PVP (HPS120) versus transurethral resection of the prostate in the treatment of lower urinary tract symptoms in Ontario, Canada; 2013.
DeMeritt JS, Elmasri FF, Esposito MP, Rosenberg GS. Relief of benign prostatic hyperplasia-related bladder outlet obstruction after transarterial polyvinyl alcohol prostate embolization. J Vasc Interv Radiol. 2000;11(6):767–70.
Carnevale FC, Antunes AA, da Motta Leal Filho JM, de Oliveira Cerri LM, Baroni RH, Marcelino AS, Freire GC, Moreira AM, Srougi M, Cerri GG. Prostatic artery embolization as a primary treatment for benign prostatic hyperplasia: preliminary results in two patients. Cardiovasc Intervent Radiol. 2010;33(2):355–61.
Gao YA, Huang Y, Zhang R, et al. Benign prostatic hyperplasia: prostatic arterial embolization versus transurethral resection of the prostate–a prospective, randomized, and controlled clinical trial. Radiology. 2014;270(3):920–8.
Pisco JM, et al. Medium- and long-term outcome of prostate artery embolization for patients with benign prostatic hyperplasia: results in 630 patients. J Vasc Intvent Radiol. 2016;27:1115–22.
Uflacker A, Haskal ZJ, Bilhim T, Patrie J, Huber T, Pisco JM. Meta-analysis of prostatic artery embolization for benign prostatic hyperplasia. J Vasc Interv Radiol. 2016. https://doi.org/10.1016/j.jvir.2016.08.004.
Guidance document for the costing of health care resources in the Canadian setting, 2nd edn. Ottawa: CADTH; 2016.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B. 1995;57:289–300.
Bank of Canada. Annual exchange rates. Bank of Canada, 2017. https://www.bankofcanada.ca/rates/exchange/annual-average-exchange-rates/. Accessed 7 July 2018.
Lukacs B, Loeffler J, Bruyre F, et al. Photoselective vaporization of the prostate with Greenlight 120-W laser compared with monopolar transurethral resection of the prostate: a multicenter randomized controlled trial. Eur Urol. 2012;61:1165–73.
Whelan JP, Bowen JM, Burke N, et al. A prospective trial of GreenLight PVP (HPS120) versus transurethral resection of the prostate in the treatment of lower urinary tract symptoms in Ontario, Canada. J Can Urol Assoc. 2013;7:335–41.
Whitty JA, Crosland P, Hewson K, Narula R, Nathan TR, Campbell PA, Keller A, Scuffham PA. A cost-minimisation analysis comparing photoselective vaporisation (PVP) and transurethral resection of the prostate (TURP) for the management of symptomatic benign prostatic hyperplasia (BPH) in Queensland, Australia. BJU Int. 2014;113(Suppl 2):21–8.
Bagla S, Smirniotopoulos J, Orlando J, Piechowiak R. Cost analysis of prostate artery embolization (PAE) and transurethral resection of the prostate (TURP) in the treatment of benign prostatic hyperplasia. Cardiovasc Interv Radiol. 2017;40(11):1694–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
For this type of study, formal consent is not required.
Informed Consent
This study has obtained IRB approval from research ethics board (University Health Network), and the need for informed consent was waived.
Consent for Publication
For this type of study, consent for publication is not required.
Rights and permissions
About this article

Cite this article
Brown, A.D., Stella, S.F. & Simons, M.E. Minimally Invasive Treatment for Benign Prostatic Hyperplasia: Economic Evaluation from a Standardized Hospital Case Costing System. Cardiovasc Intervent Radiol 42, 520–527 (2019). https://doi.org/10.1007/s00270-018-2132-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-018-2132-8