
Abstract
Background
To evaluate the clinical value of preoperative markers in predicting occult metastases in resectable pancreatic body and tail cancer judged by a recent multidetector computed tomography (MDCT) scan of the abdomen.
Methods
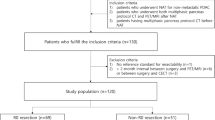
The data from a retrospective collected database from 2010 to 2019 with 699 patients who had MDCT scan predicted resectable mass in pancreatic body and tail and were pathological confirmed as adenocarcinoma after surgery. Receiver operating characteristic (ROC) curve was plotted for serum CA19-9, CA125, CEA and tumor size measured by MDCT. The optimal cut-off point-related sensitivity and specificity were calculated, respectively.
Results
Occult metastases were found in 73 (73/699, 10.4%) pancreatic body and tail cancer patients underwent exploration. The area under curve (AUC) for CA19-9, CA125, CEA and tumor size were 0.624, 0.733, 0.561 and 0.697, respectively. The optimal cut-off for CA19-9, CA125 and tumor size is 226 U/ml, 22.1 U/ml and 3.3 cm, respectively. The sensitivity and specificity of CA19-9 for predicting occult metastases were 67.1% and 60.4%, 72.6% and 64.7% for CA125, 80.8% and 51.4% for tumor size.
Conclusion
CA125 is superior to CA19-9 and tumor size for predicting occulting metastases in MDCT scan suggested resectable pancreatic body and tail cancer. The high level of CA125 (≥ 22.1 U/ml) is regarded as high risk for occulting metastases, and laparoscopy should be applied for these patients.


Similar content being viewed by others

References
Siegel RL, Miller KD, Jemal A (2017) Cancer statistics. CA Cancer J Clin 67:7–30
Chen W, Zheng R, Baade PD et al (2016) Cancer statistics in China. CA Cancer J Clin 66:115–132
Ryan DP, Hong TS, Bardeesy N (2014) Pancreatic adenocarcinoma. N Engl J Med 371:1039–1049
Parikh PY, Lillemoe KD (2015) Surgical management of pancreatic cancer–distal pancreatectomy. Semin Oncol 42:110–122
De Rosa A, Cameron IC, Gomez D (2016) Indications for staging laparoscopy in pancreatic cancer. HPB (Oxford) 18:13–20
Scialpi M, Reginelli A, D’Andrea A et al (2016) Pancreatic tumors imaging: an update. Int J Surg 28:S142–S155
Sefrioui D, Blanchard F, Toure E et al (2017) Diagnostic value of CA19.9, circulating tumour DNA and circulating tumour cells in patients with solid pancreatic tumours. Br J Cancer 117:1017–1025
La Greca G, Sofia M, Lombardo R et al (2012) Adjusting CA19-9 values to predict malignancy in obstructive jaundice: influence of bilirubin and C-reactive protein. World J Gastroenterol 18:4150–4155
Luo G, Liu C, Guo M et al (2017) Potential biomarkers in lewis negative patients with pancreatic cancer. Ann Surg 265:800–805
Luo G, Xiao Z, Long J et al (2013) CA125 is superior to CA19-9 in predicting the resectability of pancreatic cancer. J Gastrointest Surg 17:2092–2098
Al-Hawary MM, Francis IR, Chari ST et al (2014) Pancreatic ductal adenocarcinoma radiology reporting template: consensus statement of the society of abdominal radiology and the american pancreatic association. Radiology 270:248–260
Sheridan MB, Ward J, Guthrie JA et al (1999) Dynamic contrast-enhanced MR imaging and dual-phase helical CT in the preoperative assessment of suspected pancreatic cancer: a comparative study with receiver operating characteristic analysis. AJR Am J Roentgenol 173:583–590
Farma JM, Santillan AA, Melis M et al (2008) PET/CT fusion scan enhances CT staging in patients with pancreatic neoplasms. Ann Surg Oncol 15(9):2465–2471
Oba A, Inoue Y, Ono Y et al (2020) Radiologically occult metastatic pancreatic cancer: how can we avoid unbeneficial resection? Langenbecks Arch Surg 405:35–41
Liu X, Fu Y, Chen Q et al (2018) Predictors of distant metastasis on exploration in patients with potentially resectable pancreatic cancer. BMC Gastroenterol 18:168
Maithel SK, Maloney S, Winston C et al (2008) Preoperative CA 19–9 and the yield of staging laparoscopy in patients with radiographically resectable pancreatic adenocarcinoma. Ann Surg Oncol 15:3512–3520
Kamisawa T, Wood LD, Itoi T et al (2016) Pancreatic cancer. Lancet 388:73–85
Engle DD, Tiriac H, Rivera KD et al (2019) The glycan CA19-9 promotes pancreatitis and pancreatic cancer in mice. Science 364:1156–1162
Zhang S, Wang YM, Sun CD et al (2008) Clinical value of serum CA19-9 levels in evaluating resectability of pancreatic carcinoma. World J Gastroenterol 14:3750–3753
Fujioka S, Misawa T, Okamoto T et al (2007) Preoperative serum carcinoembryonic antigen and carbohydrate antigen 19–9 levels for the evaluation of curability and resectability in patients with pancreatic adenocarcinoma. J Hepatobiliary Pancreat Surg 14:539–544
Suker M, Koerkamp BG, Coene PP et al (2019) Yield of staging laparoscopy before treatment of locally advanced pancreatic cancer to detect occult metastases. Eur J Surg Oncol 45:1906–1911
Schlieman MG, Ho HS, Bold RJ (2003) Utility of tumor markers in determining resectability of pancreatic cancer. Arch Surg 138:951–956
Slaar A, Eshuis WJ, van der Gaag NA et al (2011) Predicting distant metastasis in patients with suspected pancreatic and periampullary tumors for selective use of staging laparoscopy. World J Surg 35:2528–2534
Yoshida T, Matsumoto T, Morii Y et al (2002) Staging with helical computed tomography and laparoscopy in pancreatic head cancer. Hepatogastroenterology 49:1428–1431
Liang C, Qin Y, Zhang B et al (2017) Oncogenic KRAS Targets MUC16/CA125 in Pancreatic Ductal Adenocarcinoma. Mol Cancer Res 15:201–212
Xu HX, Li S, Wu CT et al (2018) Postoperative serum CA19-9, CEA and CA125 predicts the response to adjuvant chemoradiotherapy following radical resection in pancreatic adenocarcinoma. Pancreatology 18:671–677
Yang C, Cheng H, Luo G et al (2017) The metastasis status and tumor burden-associated CA125 level combined with the CD4/CD8 ratio predicts the prognosis of patients with advanced pancreatic cancer: a new scoring system. Eur J Surg Oncol 43:2112–2118
Liu L, Xu HX, Wang WQ et al (2016) Serum CA125 is a novel predictive marker for pancreatic cancer metastasis and correlates with the metastasis-associated burden. Oncotarget 7:5943–5956
Ayhan A, Gultekin M, Celik NY et al (2007) Occult metastasis in early ovarian cancers: risk factors and associated prognosis. Am J Obstet Gynecol 196:81e1-6
Chi DS, Venkatraman ES, Masson V et al (2000) The ability of preoperative serum CA-125 to predict optimal primary tumor cytoreduction in stage III epithelial ovarian carcinoma. Gynecol Oncol 77:227–231
Fang T, Wang H, Wang Y et al (2019) Clinical significance of preoperative serum CEA, CA125, and CA19-9 levels in predicting the resectability of cholangiocarcinoma. Dis Markers 2019:6016931
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grant numbers 81625016, 81871940, 81902417), Scientific Innovation Project of Shanghai Education Committee (2019-01-07-00-07-E00057), the Shanghai Natural Science Foundation (Grant number 17ZR1406300), the Shanghai Cancer Center Foundation for Distinguished Young Scholars (Grant number YJJQ201803) and the Fudan University Personalized Project for “Double Top” Original Research (Grant number XM03190633).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Cheng, H., Luo, G., Jin, K. et al. Predictive Values of Preoperative Markers for Resectable Pancreatic Body and Tail Cancer Determined by MDCT to Detect Occult Metastases. World J Surg 45, 2185–2190 (2021). https://doi.org/10.1007/s00268-021-06047-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-021-06047-x