
Abstract
Background
Despite significant advances in imaging and endoscopic diagnostic techniques, adequate localization of gastrointestinal bleeding (GIB) can be challenging. Provocative angiography (PROVANGIO) has not been part of the standard diagnostic algorithms yet. We sought to examine the ability of PROVANGIO to identify the bleeding source when conventional radiography fails.
Methods
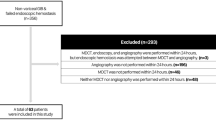
Patients undergoing PROVANGIO for GIB during 2008–2014 were retrospectively included. Demographics and periprocedural patient characteristics were recorded. PROVANGIO was performed in a multidisciplinary setting, involving interventional radiology, surgery and anesthesiology teams, ready to intervene in case of uncontrolled bleeding. The procedure included conventional angiography of the celiac, superior and inferior mesenteric arteries (SMA, IMA) followed by a stepwise bleeding provocation with anticoagulating, vasodilating and/or thrombolytic agent administration, combined with angiography.
Results
Twenty-three PROVANGIO were performed. Patients were predominantly male (15, 65.2%), and hematochezia was the most common presenting symptom (12, 52.2%). Patients with a positive PROVANGIO had lower Charlson comorbidity index (1 vs. 7, p = 0.009) and were less likely to have a prior history of GIB (14.3% vs. 87.5%, p = 0.001). PROVANGIO localized bleeding in 7 (30%) patients. In 6 out of 7 patients, the bleeding source was identified in the SMA and, in one case, in the IMA distribution. The bleeding was controlled angiographically in four cases, endoscopically in one case and surgically in the remaining two. No complications related to PROVANGIO were detected.
Conclusions
In our series, PROVANGIO safely identified the bleeding source, and provided that necessary safeguards are put into place, we recommend incorporating it in the diagnostic algorithms for GIB management.
Similar content being viewed by others


References
Oakland K (2019) Changing epidemiology and etiology of upper and lower gastrointestinal bleeding. Best Pract Res Clin Gastroenterol 42–43:101610
Billingham RP (1997) The conundrum of lower gastrointestinal bleeding. Surg Clin North Am 77(1):241–252
Farrell JJ, Friedman LS (2005) Review article: the management of lower gastrointestinal bleeding. Aliment Pharmacol Ther 21(11):1281–1298
Longstreth GF (1997) Epidemiology and outcome of patients hospitalized with acute lower gastrointestinal hemorrhage: a population-based study. Am J Gastroenterol 92(3):419–424
Johnston C, Tuite D, Pritchard R et al (2007) Use of provocative angiography to localize site in recurrent gastrointestinal bleeding. Cardiovasc Intervent Radiol 30(5):1042–1046
Wu M, Klass D, Strovski E et al (2013) Aberrant celio-mesenteric supply of the splenic flexure: provoking a bleed. World J Gastroenterol 19(39):6679–6682
Zurkiya O, Walker TG (2015) Angiographic evaluation and management of nonvariceal gastrointestinal hemorrhage. AJR Am J Roentgenol 205(4):753–763
Kim CY, Suhocki PV, Miller MJ Jr et al (2010) Provocative mesenteric angiography for lower gastrointestinal hemorrhage: results from a single-institution study. J Vasc Interv Radiol 21(4):477–483
Nusbaum M, Baum S, Blakemore WS (1969) Clinical experience with the diagnosis and management of gastrointestinal hemorrhage by selective mesenteric catheterization. Ann Surg 170(3):506–514
Lin S, Rockey DC (2005) Obscure gastrointestinal bleeding. Gastroenterol Clin North Am 34(4):679–698
Malden ES, Hicks ME, Royal HD et al (1998) Recurrent gastrointestinal bleeding: use of thrombolysis with anticoagulation in diagnosis. Radiology 207(1):147–151
Ryan JM, Key SM, Dumbleton SA et al (2001) Nonlocalized lower gastrointestinal bleeding: provocative bleeding studies with intraarterial tPA, heparin, and tolazoline. J Vasc Interv Radiol 12(11):1273–1277
Velmahos GC, Toutouzas KG, Vassiliu P et al (2002) A prospective study on the safety and efficacy of angiographic embolization for pelvic and visceral injuries. J Trauma 53(2):303–308
Rosch J, Keller FS, Wawrukiewicz AS et al (1982) Pharmacoangiography in the diagnosis of recurrent massive lower gastrointestinal bleeding. Radiology 145(3):615–619
Koval G, Benner KG, Rosch J et al (1987) Aggressive angiographic diagnosis in acute lower gastrointestinal hemorrhage. Dig Dis Sci 32(3):248–253
Bloomfeld RS, Smith TP, Schneider AM et al (2000) Provocative angiography in patients with gastrointestinal hemorrhage of obscure origin. Am J Gastroenterol 95(10):2807–2812
Shetzline MA, Suhocki P, Dash R et al (2000) Provocative angiography in obscure gastrointestinal bleeding. South Med J 93(12):1205–1208
Mernagh JR, O’Donovan N, Somers S et al (2001) Use of heparin in the investigation of obscure gastrointestinal bleeding. Can Assoc Radiol J 52(4):232–235
Widlus DM, Salis AI (2007) Reteplase provocative visceral arteriography. J Clin Gastroenterol 41(9):830–833
Kariya S, Nakatani M, Ono Y et al (2020) Provocative angiography for lower gastrointestinal bleeding. Jpn J Radiol 38(3):248–255
Acknowledgements
None.
Funding
None
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
As a retrospective chart review analysis, no informed consent was required from the individual participants. No individual participants’ identifying information is included in this article.
Ethical oversight
This study protocol was reviewed and approved by the Institutional Review Board (IRB) at the Massachusetts General Hospital.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kokoroskos, N., Naar, L., Peponis, T. et al. Provocative Angiography, Followed by Therapeutic Interventions, in the Management of Hard-To-Diagnose Gastrointestinal Bleeding. World J Surg 44, 2944–2949 (2020). https://doi.org/10.1007/s00268-020-05545-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-020-05545-8