
Abstract
Background
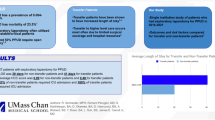
Delay to theatre for patients with intra-abdominal sepsis is cited as a particular risk factor for death. Our aim was to evaluate the potential relationship between hourly delay from admission to surgery and post-operative mortality in patients with perforated peptic ulcer (PPU).
Methods
All patients entered in the National Emergency Laparotomy Audit who had an emergency laparotomy for PPU within 24 h of admission from December 2013 to November 2017 were included. Time to theatre from admission was modelled as a continuous variable in hours. Outcome was 90-day mortality. Logistic regression adjusting for confounding factors was performed.
Results
3809 patients were included, and 90-day mortality rate was 10.61%. Median time to theatre was 7.5 h (IQR 5–11.6 h). The odds of death increased with time to operation once adjustment for confounding variables was performed (per hour after admission adjusted OR 1.04 95% CI 1.02–1.07). In patients who were physiologically shocked (N = 334), there was an increase of 6% in risk-adjusted odds of mortality for every hour Em Lap was delayed after admission (OR 1.06 95% CI 1.01–1.11).
Conclusion
Hourly delay to theatre in patients with PPU is independently associated with risk of death by 90 days. Therefore, we suggest that surgical source control should occur as soon as possible after admission regardless of time of day.


Similar content being viewed by others

References
NELA Project Team (2015) The first patient report of the national emergency laparotomy audit, London
NELA Project Team (2016) The second patient report of the national emergency laparotomy audit, London
NELA Project Team (2017) The third patient report of the national emergency laparotomy audit, London
NELA Project Team (2018) The fourth patient report of the national emergency laparotomy audit, London
Al-Temimi MH, Griffee M, Enniss TM et al (2012) When is death inevitable after emergency laparotomy? Analysis of the American College of Surgeons National Surgical Quality Improvement Program Database. J Am Coll Surg 215:503–511. https://doi.org/10.1016/J.JAMCOLLSURG.2012.06.004
Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, Gurka D, Kumar A, Cheang MM (2006) Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 34:159–1589
Levy MM, Dellinger RP, Townsend SR, Linde-Zwirble WT, Marshall JC, Bion J, Schorr C, Artigas A, Ramsay G, Beale R, Parker MM, Gerlach HM, on behalf of the SSC (2010) The surviving sepsis campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med 38:367–374
Prospective A, Study O, Ferrer R et al (2009) Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study. Am J Respir Crit Care Med 180:861–866. https://doi.org/10.1164/rccm.200812-1912OC
Sterling SA, Miller WR, Pryor J et al (2016) The impact of timing of antibiotics on outcomes in severe sepsis and septic shock: a systematic review and meta-analysis. Crit Care Med 43:1907–1915. https://doi.org/10.1097/CCM.0000000000001142.The
Azuhata T, Kinoshita K, Kawano D et al (2014) Time from admission to initiation of surgery for source control is a critical determinant of survival in patients with gastrointestinal perforation with associated septic shock. Crit Care 18:1–10. https://doi.org/10.1186/cc13854
Vester-andersen M, Lundstrøm LH, Buck DL et al (2016) Association between surgical delay and survival in high-risk emergency abdominal surgery. A population-based Danish cohort study. Scand J Gastroenterol 51:121–128. https://doi.org/10.3109/00365521.2015.1066422
Buck DL, Møller MH, Register C (2013) Surgical delay is a critical determinant of survival in perforated. Br J Surg 100:1045–1049. https://doi.org/10.1002/bjs.9175
Fong IW (1983) Septic complications of perforated peptic ulcer. Can J Surg 26:370–372
Opal SM, Rubenfeld GD, Van Der PT et al (2016) The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 315:801–810. https://doi.org/10.1001/jama.2016.0287
Eugene N, Oliver CM, Bassett MG et al (2018) Development and internal validation of a novel risk adjustment model for adult patients undergoing emergency laparotomy surgery: the National Emergency Laparotomy Audit risk model. Br J Anaesth 121:739–748. https://doi.org/10.1016/j.bja.2018.06.026
Oliver CM, Bassett MG, Poulton TE et al (2018) Organisational factors and mortality after an emergency laparotomy: multilevel analysis of 39 903 National Emergency Laparotomy Audit patients. Br J Anaesth 121:1346–1356. https://doi.org/10.1016/j.bja.2018.07.040
von Elm E, Altman DG, Egger M et al (2007) Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 335:806–808. https://doi.org/10.1136/bmj.39335.541782.AD
Thorsen K, Søreide JA, Søreide K (2017) Long-term mortality in patients operated for perforated peptic ulcer: factors limiting longevity are dominated by older age, comorbidity burden and severe postoperative complications. World J Surg 41:410–418. https://doi.org/10.1007/s00268-016-3747-z
Lolle I, Møller MH, Rosenstock SJ (2016) Association between ulcer site and outcome in complicated peptic ulcer disease: a Danish nationwide cohort study. Scand J Gastroenterol. https://doi.org/10.1080/00365521.2016.1190398
National Confidential Enquiry into Patient Outcome and Death (2005) Abdominal aortic aneurysm: a service in need of surgery?
The Royal College of Surgeons (Eng) (2018) The high-risk general surgical patient: raising the standard, London
Huddart S, Peden CJ, Swart M et al (2015) Use of a pathway quality improvement care bundle to reduce mortality after emergency laparotomy. Br J Surg 102:57–66. https://doi.org/10.1002/bjs.9658
FLOELA Project Team (2018) Fluid optimisation in emergency laparotomy
Acknowledgements
The authors wish to acknowledge the work of all past and present members of the National Emergency Laparotomy Audit Project team who have been involved in the running and progression of the Audit and the NHS staff who have submitted data to NELA over the last 4 years.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Boyd-Carson, H., Doleman, B., Cromwell, D. et al. Delay in Source Control in Perforated Peptic Ulcer Leads to 6% Increased Risk of Death Per Hour: A Nationwide Cohort Study. World J Surg 44, 869–875 (2020). https://doi.org/10.1007/s00268-019-05254-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-019-05254-x