
Abstract
Background
Under-triaged trauma patients have worse clinical outcomes. We evaluated the capability of four pre-hospital variables to identify this population at the lowest level trauma activation (level 3).
Methods
A retrospective review of adult trauma activations from 2004 to 2014 was completed. Pre-hospital vital signs and Glasgow Coma Scale were converted to categorical variables. Patients were under-triaged based on meeting current level 1 or 2 criteria, or requiring a pre-defined critical intervention. Logistic regression was used to determine the association between the pre-hospital variables and under-triaged patients. Odds ratios and 95% confidence intervals were calculated for a comprehensive model, grouping all causes of under-triage as a single unit, and 16 individual models, one for each under-triage criterion. A new level 2 criterion was generated and internally validated.
Results
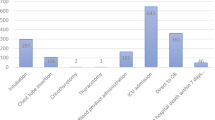
In total, 12,332 activations occurred during the study period. Four hundred and sixty-six (5.9%) patients were under-triaged. Compared to patients with a normal respiratory rate (RR), tachypneic patients were more likely to be under-triaged for any reason, OR 1.7 [1.3–2.1], p < 0.001. In the individual event analysis, tachypneic patients were more likely to have flail chest, OR 22 [2.9–168.3], p = 0.003; require a chest tube, OR 3 [1.8–4.9], p < 0.001; or require emergent intubation, OR 1.6 [1.1–2.8], p = 0.04, compared to patients with a normal RR. The data-driven triage modification was tachypnea with suspected thoracic injury which reduced the under-triage rate by 1.2%.
Conclusion
Tachypnea with suspected thoracic injury is the strongest level 2 triage modification to reduce level 3 under-triage.
Similar content being viewed by others


References
Sasser SM, Hunt RC, Faul M et al (2012) Guidelines for field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2011. MMWR Recomm Rep 61(1):1–20
Rotondo MM, Cribari CM, Smith SM (2014) Resources for optimal care of the injured patient. Comm Trauma Am Coll Surg 1:1
Cohen R, Adini B, Radomislensky I, Givon A, Rivkind AI, Peleg K (2012) Involvement of surgical residents in the management of trauma patients in the emergency room: does the presence of an attending physician affect outcomes? World J Surg 36(3):539–547. https://doi.org/10.1007/s00268-012-1428-0
Cox JA, Bernard AC, Bottiggi AJ et al (2014) Influence of in-house attending presence on trauma outcomes and hospital efficiency. J Am Coll Surg 218(4):734–738. https://doi.org/10.1016/j.jamcollsurg.2013.12.027
Durham R, Shapiro D, Flint L (2005) In-house trauma attendings: is there a difference? Am J Surg 190(6):960–966. https://doi.org/10.1016/j.amjsurg.2005.08.028
Helling TS, Nelson PW, Shook JW, Lainhart K, Kintigh D (2003) The presence of in-house attending trauma surgeons does not improve management or outcome of critically injured patients. J Trauma 55(1):20–25. https://doi.org/10.1097/01.TA.0000071621.39088.7B
Mains C, Scarborough K, Bar-Or R et al (2009) Staff commitment to trauma care improves mortality and length of stay at a level I trauma center. J Trauma 66(5):1315–1320. https://doi.org/10.1097/TA.0b013e31819d96d8
Porter JM, Ursic C (2001) Trauma attending in the resuscitation room: does it affect outcome? Am Surg 67(7):611–614
Tinkoff GH, O’Connor RE (2002) Validation of new trauma triage rules for trauma attending response to the emergency department. J Trauma 52(6):1153–1158 (discussion 1158–1159)
Lehmann R, Brounts L, Lesperance K et al (2009) A simplified set of trauma triage criteria to safely reduce overtriage: a prospective study. Arch Surg 144(9):853–858. https://doi.org/10.1001/archsurg.2009.153
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Yonge, J.D., Bohan, P.K., Watson, J.J. et al. The Respiratory Rate: A Neglected Triage Tool for Pre-hospital Identification of Trauma Patients. World J Surg 42, 1321–1326 (2018). https://doi.org/10.1007/s00268-017-4353-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-017-4353-4