
Abstract
Background
Outpatient arthroplasty programs are becoming well established. Adverse event rates have been demonstrated to be no worse than inpatient arthroplasty in the literature for selected patients. The purpose of this study was to determine our rate of outpatient total knee arthroplasty (TKA), examine justification for exclusions, and estimate the proportion of TKAs that can occur safely on an outpatient basis.
Methods
Retrospective case series of 400 consecutive TKAs from Oct 2014 to Mar 2017. Patient demographics, allocation to outpatient surgery vs standard admission, and reason for exclusion from outpatient surgery were recorded. Ninety-day Emergency department (ED) visits, readmission rates, and length of stay (LOS) were compared between groups using independent sample t test and Chi-squared test.
Results
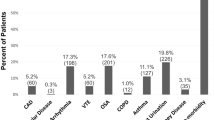
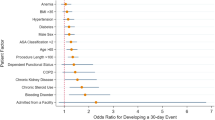
Outpatients were younger (p = 0.001), had lower BMI (p < 0.001), and ASA scores (p < 0.001) than inpatients. One hundred twenty-five (31%) TKAs were assigned to outpatient surgery and 123 achieved discharge on the same day. There was no difference in 90-day ED visits (p = 0.889) or readmission rates (p = 0.338) between groups. Reasons for exclusion from outpatient surgery included medical (absolute 43% and relative 31%), distance > one hour from hospital (18%), no help (7%), and other/unclear (10%). LOS was significantly longer for medical than non-medical exclusions (p < 0.001) and for the absolute compared to relative medical exclusions (p = 0.004).
Conclusion
Outpatient TKA is safe in selected patients, and inclusion can likely be broadened by addressing modifiable exclusions and narrowing medical exclusions. We found that 55% of our TKA population could be appropriate for outpatient surgery.



Similar content being viewed by others

References
Berger RA, Sanders S, Gerlinger T, Della Valle C, Jacobs JJ, Rosenberg AG (2005) Outpatient total knee arthroplasty with a minimally invasive technique. J Arthroplast 20:33–38
Berger RA, Kusuma SK, Sanders SA, Thill ES, Sporer SM (2009) The feasibility and perioperative complications of outpatient knee arthroplasty. Clin Orthop Relat Res 467(6):1443–1449. https://doi.org/10.1007/s11999-009-0736-7
Lovald ST, Ong KL, Malkani AL, Lau EC, Schmier JK, Kurtz SM, Manley MT (2014) Complications, mortality, and costs for outpatient and short-stay total knee arthroplasty patients in comparison to standard-stay patients. J Arthroplast 29(3):510–515
Huang A, Ryu J-J, Dervin G (2017) Cost savings of outpatient versus standard inpatient total knee arthroplasty. Can J Surg 60(1):57
Dorr LD, Thomas DJ, Zhu J, Dastane M, Chao L, Long WT (2010) Outpatient total hip arthroplasty. J Arthroplast 25(4):501–506. https://doi.org/10.1016/j.arth.2009.06.005
Meneghini RM, Ziemba-Davis M, Ishmael MK, Kuzma AL, Caccavallo P (2017) Safe selection of outpatient joint arthroplasty patients with medical risk stratification: the “outpatient arthroplasty risk assessment score”. J Arthroplast 32(8):2325–2331
O'Reilly M, Mohamed K, Foy D, Sheehan E (2018) Educational impact of joint replacement school for patients undergoing total hip and knee arthroplasty: a prospective cohort study. Int Orthop. https://doi.org/10.1007/s00264-018-4039-z
Bovonratwet P, Ondeck NT, Nelson SJ, Cui JJ, Webb ML, Grauer JN (2017) Comparison of outpatient vs inpatient total knee arthroplasty: an ACS-NSQIP analysis. J Arthroplast 32(6):1773–1778
Lovecchio F, Alvi H, Sahota S, Beal M, Manning D (2016) Is outpatient arthroplasty as safe as fast-track inpatient arthroplasty? A propensity score matched analysis. J Arthroplast 31(9):197–201
Otero JE, Gholson JJ, Pugely AJ, Gao Y, Bedard NA, Callaghan JJ (2016) Length of hospitalization after joint arthroplasty: does early discharge affect complications and readmission rates? J Arthroplast 31(12):2714–2725
Den Hartog Y, Mathijssen N, Hannink G, Vehmeijer S (2015) Which patient characteristics influence length of hospital stay after primary total hip arthroplasty in a ‘fast-track’setting? Bone Joint J 97(1):19–23
Kolisek FR, McGrath MS, Jessup NM, Monesmith EA, Mont MA (2009) Comparison of outpatient versus inpatient total knee arthroplasty. Clin Orthop Relat Res 467(6):1438–1442
Gauthier-Kwan OY, Dobransky JS, Dervin GF (2018) Quality of recovery, Postdischarge hospital utilization, and 2-year functional outcomes after an outpatient Total knee arthroplasty program. J Arthroplast 33(7):2159–2164.e2151. https://doi.org/10.1016/j.arth.2018.01.058
Argenson J-NA, Husted H, Lombardi A Jr, Booth RE, Thienpont E (2016) Global forum: an international perspective on outpatient surgical procedures for adult hip and knee reconstruction. JBJS 98(13):e55
Courtney PM, Boniello AJ, Berger RA (2017) Complications following outpatient total joint arthroplasty: an analysis of a national database. J Arthroplast 32(5):1426–1430
Su EP, Perna M, Boettner F, Mayman DJ, Gerlinger T, Barsoum W, Randolph J, Lee G (2012) A prospective, multi-center, randomised trial to evaluate the efficacy of a cryopneumatic device on total knee arthroplasty recovery. J Bone Joint Surg Br 94(11 Suppl a):153–156. https://doi.org/10.1302/0301-620x.94b11.30832
Song MH, Kim BH, Ahn SJ, Yoo SH, Kang SW, Kim YJ, Kim DH (2016) Peri-articular injections of local anaesthesia can replace patient-controlled analgesia after total knee arthroplasty: a randomised controlled study. Int Orthop 40(2):295–299. https://doi.org/10.1007/s00264-015-2940-2
Li D, Yang Z, Xie X, Zhao J, Kang P (2016) Adductor canal block provides better performance after total knee arthroplasty compared with femoral nerve block: a systematic review and meta-analysis. Int Orthop 40(5):925–933. https://doi.org/10.1007/s00264-015-2998-x
Li Z, Cheng W, Sun L, Yao Y, Cao Q, Ye S, Qi L, Xu S, Wu X, Jing J (2018) Mini-subvastus versus medial parapatellar approach for total knee arthroplasty: a prospective randomized controlled study. Int Orthop 42(3):543–549. https://doi.org/10.1007/s00264-017-3703-z
Courtney PM, Melnic CM, Gutsche J, Hume EL, Lee GC (2015) Which patients need critical care intervention after total joint arthroplasty? : A prospective study of factors associated with the need for intensive care following surgery. Bone Joint J 97-B(11):1512–1518. https://doi.org/10.1302/0301-620X.97B11.35813
Sutton JC III, Antoniou J, Epure LM, Huk OL, Zukor DJ, Bergeron SG (2016) Hospital discharge within 2 days following total hip or knee arthroplasty does not increase major-complication and readmission rates. JBJS 98(17):1419–1428
Pulido L, Parvizi J, Macgibeny M, Sharkey PF, Purtill JJ, Rothman RH, Hozack WJ (2008) In hospital complications after total joint arthroplasty. J Arthroplast 23(6):139–145
Edelstein AI, Kwasny MJ, Suleiman LI, Khakhkhar RH, Moore MA, Beal MD, Manning DW (2015) Can the American College of Surgeons risk calculator predict 30-day complications after knee and hip arthroplasty? J Arthroplast 30(9):5–10
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was reviewed and approved by the institutional ethics committee and the authors have no conflicts of interest to disclose.
Conflict of interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Gillis, M.E., Dobransky, J. & Dervin, G.F. Defining growth potential and barriers to same day discharge total knee arthroplasty. International Orthopaedics (SICOT) 43, 1387–1393 (2019). https://doi.org/10.1007/s00264-018-4100-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-018-4100-y