
Abstract
Purpose
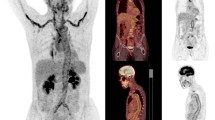
The aim of this study was to quantify the association between the CRP value and 18F–FDG PET vascular positivity in Takayasu arteritis (TAK) through a structured dedicated systematic review and meta-analysis.
Methods
From January 2000 to December 2016, the PubMed/MEDLINE database was searched for articles specifically dealing with the assessment of vascular inflammation using 18F–FDG PET and CRP biomarkers in TAK. Inclusion criteria for the qualitative analysis were (1) 18F–FDG PET used to assess the disease activity, (2) The use of the ACR criteria for the diagnosis of TAK, (3) No case mixed vasculitis (i.e., no giant cell arteritis), and (4) CRP concentration and clinical disease activity available. For the meta-analysis, PET-positive and PET-negative subgroups with the corresponding CRP concentrations were generated based on per patient data. The standard mean difference, which represents the effect of the CRP concentrations on the 18F–FDG PET vascular uptake, was computed for all studies, and then the results were pooled together.
Results
Among the 33 initial citations, nine complete articles including 210 patients fulfilled the inclusion criteria. Five studies found a significant correlation between the 18F–FDG PET and CRP concentration, one provided a trend towards association and three did not find any association between the two biomarkers. Six studies found a significant association between 18F–FDG PET and clinical disease activity, one found a trend towards association and the last two studies did not evaluate this correlation. The meta-analysis (121 patients) provided the following results: Standard Mean Deviation = 0.54 [0.15;0.92]; Chi2 = 3.35; I2 = 0%; Test for overall effect: Z = 2.70 (P = 0.007).
Conclusion
The CRP concentration only moderately reflects the 18F–FDG PET vascular positivity in TAK, suggesting dissociated information. Standardized longitudinal prospective studies are necessary to assess the value of 18F–FDG PET as an independent biomarker for subtle vascular wall inflammation detection.


Similar content being viewed by others


References
Maksimowicz-McKinnon K, Hoffman GS. Takayasu arteritis: what is the long-term prognosis? Rheum Dis Clin N Am. 2007;33:777–86. vi
Borg FA, Dasgupta B. Treatment and outcomes of large vessel arteritis. Best Pract Res Clin Rheumatol. 2009;23:325–37.
Kerr GS, Hallahan CW, Giordano J, Leavitt RY, Fauci AS, Rottem M, et al. Takayasu arteritis. Ann Intern Med. 1994;120:919–29.
Hoffman GS, Ahmed AE. Surrogate markers of disease activity in patients with Takayasu arteritis. A preliminary report from the international network for the study of the systemic Vasculitides (INSSYS). Int J Cardiol. 1998;66 Suppl 1:S191–4. discussion S195
Belhocine T, Blockmans D, Hustinx R, Vandevivere J, Mortelmans L. Imaging of large vessel vasculitis with (18)FDG PET: illusion or reality? A critical review of the literature data. Eur J Nucl Med Mol Imaging. 2003;30:1305–13.
Walter MA, Melzer RA, Schindler C, Müller-Brand J, Tyndall A, Nitzsche EU. The value of [18F]FDG-PET in the diagnosis of large-vessel vasculitis and the assessment of activity and extent of disease. Eur J Nucl Med Mol Imaging. 2005;32:674–81.
Direskeneli H, Aydin SZ, Merkel PA. Assessment of disease activity and progression in Takayasu’s arteritis. Clin Exp Rheumatol. 2011;29:S86–91.
Fuchs M, Briel M, Daikeler T, Walker UA, Rasch H, Berg S, et al. The impact of 18F-FDG PET on the management of patients with suspected large vessel vasculitis. Eur J Nucl Med Mol Imaging. 2012;39:344–53.
Soussan M, Nicolas P, Schramm C, Katsahian S, Pop G, Fain O, et al. Management of large-vessel vasculitis with FDG-PET: a systematic literature review and meta-analysis. Medicine (Baltimore). 2015;94:e622.
Jamar F, Buscombe J, Chiti A, Christian PE, Delbeke D, Donohoe KJ, et al. EANM/SNMMI guideline for 18F-FDG use in inflammation and infection. J Nucl Med. 2013;54:647–58.
Grayson PC, Tomasson G, Cuthbertson D, Carette S, Hoffman GS, Khalidi NA, et al. Association of vascular physical examination findings and arteriographic lesions in large vessel vasculitis. J Rheumatol. 2012;39:303–9.
Webb M, Chambers A, Al-Nahhas A, Mason JC, Maudlin L, Rahman L, et al. The role of 18F-FDG PET in characterising disease activity in Takayasu arteritis. Eur J Nucl Med Mol Imaging. 2004;31:627–34.
Andrews J, Al-Nahhas A, Pennell DJ, Hossain MS, Davies KA, Haskard DO, et al. Non-invasive imaging in the diagnosis and management of Takayasu’s arteritis. Ann Rheum Dis. 2004;63:995–1000.
Kobayashi Y, Ishii K, Oda K, Nariai T, Tanaka Y, Ishiwata K, et al. Aortic wall inflammation due to Takayasu arteritis imaged with 18F-FDG PET coregistered with enhanced CT. J Nucl Med. 2005;46:917–22.
Lee SG, Ryu J-S, Kim HO, Oh JS, Kim YG, Lee C-K, et al. Evaluation of disease activity using F-18 FDG PET-CT in patients with Takayasu arteritis. Clin Nucl Med. 2009;34:749–52.
Arnaud L, Haroche J, Malek Z, Archambaud F, Gambotti L, Grimon G, et al. Is (18)F-fluorodeoxyglucose positron emission tomography scanning a reliable way to assess disease activity in Takayasu arteritis? Arthritis Rheum. 2009;60:1193–200.
Tezuka D, Haraguchi G, Ishihara T, Ohigashi H, Inagaki H, Suzuki J, et al. Role of FDG PET-CT in Takayasu arteritis: sensitive detection of recurrences. JACC Cardiovasc Imaging. 2012;5:422–9.
Lee K-H, Cho A, Choi Y-J, Lee S-W, Ha Y-J, Jung S-J, et al. The role of (18) F-fluorodeoxyglucose-positron emission tomography in the assessment of disease activity in patients with takayasu arteritis. Arthritis Rheum. 2012;64:866–75.
Karapolat I, Kalfa M, Keser G, Yalçin M, Inal V, Kumanlioğlu K, et al. Comparison of F18-FDG PET/CT findings with current clinical disease status in patients with Takayasu’s arteritis. Clin Exp Rheumatol. 2013;31:S15–21.
Alibaz-Oner F, Dede F, Ones T, Turoglu HT, Direskeneli H. Patients with Takayasu’s arteritis having persistent acute-phase response usually have an increased major vessel uptake by 18F-FDG-PET/CT. Mod Rheumatol. 2015;25:752–5.
Cohen J. Statistical power analysis for the Behavioral sciences. 2nd ed. Hillsdale: Erlbaum; 1988.
Takeshima N, Sozu T, Tajika A, Ogawa Y, Hayasaka Y, Furukawa TA. Which is more generalizable, powerful and interpretable in meta-analyses, mean difference or standardized mean difference? BMC Med Res Methodol. 2014;14:30.
Henes JC, Müller M, Krieger J, Balletshofer B, Pfannenberg AC, Kanz L, et al. [18F] FDG-PET/CT as a new and sensitive imaging method for the diagnosis of large vessel vasculitis. Clin Exp Rheumatol. 2008;26:S47–52.
Santhosh S, Mittal BR, Gayana S, Bhattacharya A, Sharma A, Jain S. F-18 FDG PET/CT in the evaluation of Takayasu arteritis: an experience from the tropics. J Nucl Cardiol. 2014;21:993–1000.
Dhingra R, Talwar KK, Chopra P, Kumar R. An enzyme linked immunosorbent assay for detection of anti-aorta antibodies in Takayasu arteritis patients. Int J Cardiol. 1993;40:237–42.
Park MC, Lee SW, Park YB, Lee SK, Choi D, Shim WH. Post-interventional immunosuppressive treatment and vascular restenosis in Takayasu’s arteritis. Rheumatol (Oxford). 2006;45:600–5.
Chauhan SK, Tripathy NK, Sinha N, Nityanand S. T-cell receptor repertoire of circulating gamma delta T-cells in Takayasu’s arteritis. Clin Immunol. 2006;118:243–9.
Park M-C, Park Y-B, Jung SY, Lee KH, Lee S-K. Anti-endothelial cell antibodies and antiphospholipid antibodies in Takayasu’s arteritis: correlations of their titers and isotype distributions with disease activity. Clin Exp Rheumatol. 2006;24:S10–6.
Saadoun D, Garrido M, Comarmond C, Desbois AC, Domont F, Savey L, et al. Th1 and Th17 cytokines drive inflammation in Takayasu arteritis. Arthritis Rheumatol. 2015;67:1353–60.
Noris M, Daina E, Gamba S, Bonazzola S, Remuzzi G. Interleukin-6 and RANTES in Takayasu arteritis: a guide for therapeutic decisions? Circulation. 1999;100:55–60.
Tripathi M, Chandrashekar N, Phom H, Gupta DK, Bajpai M, Bal C, et al. Evaluation of dilated upper renal tracts by technetium-99m ethylenedicysteine F+O diuresis renography in infants and children. Ann Nucl Med. 2004;18:681–7.
Mason JC. Takayasu arteritis--advances in diagnosis and management. Nat Rev Rheumatol. 2010;6:406–15.
Besson FL, Parienti J-J, Bienvenu B, Prior JO, Costo S, Bouvard G, et al. Diagnostic performance of 18F-fluorodeoxyglucose positron emission tomography in giant cell arteritis: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2011;38:1764–72.
Zhao S, Kuge Y, Kohanawa M, Takahashi T, Kawashima H, Temma T, et al. Extensive FDG uptake and its modification with corticosteroid in a granuloma rat model: an experimental study for differentiating granuloma from tumors. Eur J Nucl Med Mol Imaging. 2007;34:2096–105.
Stellingwerff MD, Brouwer E, Lensen K-JDF, Rutgers A, Arends S, van der Geest KSM, et al. Different scoring methods of FDG PET/CT in Giant cell Arteritis: need for standardization. Medicine (Baltimore). 2015;94:e1542.
Incerti E, Tombetti E, Fallanca F, Baldissera EM, Alongi P, Tombolini E, et al. (18)F-FDG PET reveals unique features of large vessel inflammation in patients with Takayasu’s arteritis. Eur J Nucl Med Mol Imaging. 2017;44:1109–18.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Rights and permissions
About this article

Cite this article
Gomez, L., Chaumet-Riffaud, P., Noel, N. et al. Effect of CRP value on 18F–FDG PET vascular positivity in Takayasu arteritis: a systematic review and per-patient based meta-analysis. Eur J Nucl Med Mol Imaging 45, 575–581 (2018). https://doi.org/10.1007/s00259-017-3798-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-017-3798-x