
Abstract
Objective
To evaluate a range of pathologically proven malignant bone tumours, including primary bone sarcoma and metastatic bone lesions, referred to a tertiary referral centre for the presence of the flow-void sign on MR imaging.
Materials and methods
A retrospective search was performed using the radiology information system and oncology database in our institution to identify patients over the age of 40 years referred with a solitary bone lesion. Patients with a range of pathologically proven malignant bone tumours, including primary bone tumours and metastatic bone lesions, were included in the study. MRI images were reviewed for the presence of the flow-void sign. The presence and type of the flow-void sign were correlated with lesion size.
Results
Two hundred and sixty-six cases were included in the study. Overall, the flow-void sign was identified in 40.9% of cases. The flow-void sign was most frequently seen in renal cell carcinoma metastasis (90.0%). The sign is highly sensitive (90%) for renal cell carcinoma metastases with a high negative predictive value (98.09%). When the flow-void sign is identified, the lesion is almost three times more likely to represent a renal cell carcinoma metastasis than any other malignant tumour in patients over the age of 40 years with a solitary bone lesion.
Conclusion
The flow-void sign is highly sensitive for renal cell carcinoma bone metastases and could negate the need for biopsy in patients with a known history of renal cell carcinoma or in whom an occult renal cell carcinoma is subsequently identified.


Similar content being viewed by others


Data Availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request.
References
Choi JA, Lee KH, Jun WS, Yi MG, Lee S, Kang HS. Osseous metastasis from renal cell carcinoma: “flow-void” sign at MR imaging. Radiology. 2003;228:629–34.
Murphy J, Patel A, James SL, Botchu R, Davies AM. “Flow-void” sign in osseous metastatic renal cell carcinoma. Clin Rad. 2019;74(2):111–5.
Feltrin LT, Ferreira JR, Mamere AE, et al. Signs of hypervascularization at magnetic resonance imaging in bone metastases from renal cell carcinoma. Radiol Bras. 2009;42:155e7.
Shi D, Zhang R. Long bone metastases of renal cell carcinoma imaging features: case report and literature review. Oncologie. 2023;25(5):571–9.
Bradley WG Jr. Carmen lecture Flow. phenomena in MRI. Am J Roentgenol. 1988;150:983e94.
Murakami R, Korogi Y, Sakamoto Y, et al. Skull metastasis from hepatocellular carcinoma. CT, MR and angiographic findings. Acta Radiol. 1995;36:597–602.
Arora RS, Alston RD, Eden TOB, Geraci M, Birch JM. The contrasting age-incidence patterns of bone tumors in teenagers and young adults: Implications for aetiology. Int J Cancer. 2012;131:1678–85. https://doi.org/10.1002/ijc.27402.
Murphey MD, Fairbairn KJ, Parman LM, Baxter KG, Parsa MB, Smith WS. Musculoskeletal angiomatous lesions: radiologic-pathologic correlation. Radiographics. 1995;15:893–917.
Mahnken AH, Tacke J, Wolter P, Buttner R, Haller JS, Gunther RW. Cross-sectional imaging of primary osseous hemangiopericytoma. Eur Radiol. 2002;12:85–9.
Iwamoto Y, Morimoto N, Chuman H, Shinohara N, Sugioka Y. The role of MR imaging in the diagnosis of alveolar soft part sarcoma: a report of 10 cases. Skeletal Radiol. 1995;24:267–70.
Suh JS, Cho J, Lee SH, et al. Alveolar soft part sarcoma: MR and angiographic findings. Skeletal Radiol. 2000;29:680–9.
Rak KM, Yakes WF, Ray RL, et al. MR imaging of symptomatic peripheral vascular malformations. AJR Am J Roentgenol. 1992;159:107–12.
Lorigan JG, O’Keeffe FN, Evans HL, Wallace S. The radiologic manifestations of alveolar soft-part sarcoma. AJR Am J Roentgenol. 1989;153:335–9.
Murakami R, Korogi Y, Sakamoto Y, et al. Skull metastasis from hepatocellular carcinoma. CT MR and angiographic findings. Acta Radiol. 1995;36(6):597–602.
Iritani Y, Kato H, Kaneko Y, et al. Two cases of flow void sign in temporal bone metastasis from follicular thyroid carcinoma. Neuroradiol J. 2023;36(3):361–5.
Bjersand AJ. Bone involvement pattern in hypervascular lesions. Skeletal Radiol. 1982;9:103–8.
Acknowledgements
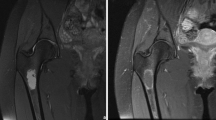
Figure 1 was published in Clinical Radiology 74 (2) Murphy J, Patel A, James SL, Botchu R, Davies AM. “Flow-void” sign in osseous metastatic renal cell carcinoma, pages 111–115. Copyright Elsevier (2019). Permission has been granted for its use in this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
Approval from the Institutional Review Board was obtained, and in keeping with the policies for a retrospective review, informed consent was not required.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Murphy, J., Rajakulasingam, R., Iqbal, A. et al. The use of the flow-void sign on MRI: highly sensitive sign in detecting bone metastases from renal cell carcinoma. Skeletal Radiol 53, 917–922 (2024). https://doi.org/10.1007/s00256-023-04512-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-023-04512-3