
Abstract
Objective
Tarsal coalition is known to cause abnormal talocrural stress, hindfoot malalignment, and ankle sprains. These can all be associated with osteochondritis dissecans (OCD) of the talar dome. We present the first detailed description of a series of talar OCDs occurring in patients with tarsal coalition, with the goal of determining whether there is an increased prevalence of OCDs among patients with tarsal coalition.
Materials and methods
We studied ankle MRIs in 57 patients with tarsal coalitions, excluding those with a reported inciting traumatic event. The MRIs were performed on magnetic field strengths ranging from 0.3 to 1.5 T and included axial, coronal, and sagittal T1 and T2 or PD fat-suppressed sequences. We evaluated the morphology and location of classically described OCDs in these patients, type and location of concomitant tarsal coalition, and, when available, the presence of pes planus and hindfoot valgus on weight-bearing radiographs. Chi-squared analysis was used to compare categorical variables and a Student’s t test was used for parametric continuous variables. Additionally, logistic regression was used to compute the odds ratio of talar OCD associated with patient age, gender, laterality, pes planus status, hindfoot valgus status, and coalition type.
Results
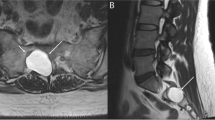
Eighty-nine percent of tarsal coalitions were non-osseous coalitions and the calcaneonavicular space was the most common site of abnormal tarsal connection (54.4%). In the 29 patients with tarsal coalitions and talar OCDs, OCDs commonly occurred medially (75.9%). In the sagittal plane, talar OCDs occurred centrally, with only one case sparing the central talar dome. The mean surface area of the 29 OCDs was 89.7 mm2. Both osseous coalition and hindfoot valgus were associated with smaller talar OCD mean surface area (p = 0.015 and p = 0.0001, respectively). There was no association between depth and surface area of talar OCD with either coalition location or presence of pes planus (coalition location: p = 0.455 for depth and p = 0.295 for surface area; presence of pes planus: p = 0.593 for depth and p = 0.367 for surface area).
Conclusion
Talar OCD prevalence is higher in patients with tarsal coalition than that reported for the general population. This occurrence may relate to altered biomechanics and repetitive talocrural stress owing to altered subtalar motion, particularly given the findings of increased odds of talar OCD in older patients, as well as weak associations between OCD surface area and both non-osseous coalition and hindfoot alignment. However, we did not find any specific OCD morphologic features attributable to the precise location of the tarsal coalition.





Similar content being viewed by others


References
Berndt AL, Harty M. Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Jt Surg Am. 1959;41:988–1020.
Kraeutler MJ, Chahla J, Dean CS, Mitchell JJ, Santini-Araujo MG, Pinney SJ, et al. Current concepts review update: osteochondral lesions of the talus. Foot Ankle Int. 2017;38:331–42. https://doi.org/10.1177/1071100716677746.
Mccullough C, Venugopal V. Osteochondritis dissecans of the talus. Clin Orthop. 1979:264–8.
Shea MP, Manoli A. Osteochondral lesions of the talar dome. Foot Ankle. 1993;14:48–55. https://doi.org/10.1177/107110079301400110.
Ray RB, EJJ C. Osteochondritis dissecans of the talus. JBJS. 1947;29:697.
Campbell CJ, Ranawat CS. osteochondritis dissecans: the question of etiology. J Trauma Acute Care Surg. 1966;6:201.
Wagoner G, Cohn BNE. Osteochondritis dissecans: a résumé of the theories of etiology and the consideration of heredity as an etiologic factor. Arch Surg. 1931;23:1–25. https://doi.org/10.1001/archsurg.1931.01160070004001.
Verhagen RAW, Maas M, MGW D, Tol JL, Krips R, van Dijk CN. Prospective study on diagnostic strategies in osteochondral lesions of the talus. J Bone Joint Surg (Br). 2005;87-B:41–6. https://doi.org/10.1302/0301-620X.87B1.14702.
Gianakos AL, Yasui Y, Hannon CP, Kennedy JG. Current management of talar osteochondral lesions. World J Orthop. 2017;8:12–20. https://doi.org/10.5312/wjo.v8.i1.12.
Chu IT, Kim YS, Yoo SH, Oh IS. The incidences and locations of osteochondral lesions of the talus in ankle fracture. J Korean Orthop Assoc. 2004;39:494–7. https://doi.org/10.4055/jkoa.2004.39.5.494.
Thordarson DB. Talar body fractures. Orthop Clin North Am. 2001;32:65–77. https://doi.org/10.1016/S0030-5898(05)70194-2.
De Smet AA, Fisher DR, Burnstein MI, Graf BK, Lange RH. Value of MR imaging in staging osteochondral lesions of the talus (osteochondritis dissecans): results in 14 patients. Am J Roentgenol. 1990;154:555–8. https://doi.org/10.2214/ajr.154.3.2106221.
Flick AB, Gould N. Osteochondritis dissecans of the talus (transchondral fractures of the talus): review of the literature and new surgical approach for medial dome lesions. Foot Ankle. 1985;5:165–85. https://doi.org/10.1177/107110078500500403.
Canale S, Belding R. Osteochondral lesions of the talus. J Bone Jt Surg. 1980;62:97–102.
Raikin SM, Elias I, Zoga AC, Morrison WB, Besser MP, Schweitzer ME. Osteochondral lesions of the talus: localization and morphologic data from 424 patients using a novel anatomical grid scheme. Foot Ankle Int. 2007;28:154–61. https://doi.org/10.3113/FAI.2007.0154.
Orr JD, Dutton JR, Fowler JT. Anatomic location and morphology of symptomatic, operatively treated osteochondral lesions of the talus. Foot Ankle Int. 2012;33:1051–7. https://doi.org/10.3113/FAI.2012.1051.
Hembree WC, Wittstein JR, Vinson EN, Queen RM, LaRose CR, Singh K, et al. Magnetic resonance imaging features of osteochondral lesions of the talus. Foot Ankle Int. 2012;33:591–7. https://doi.org/10.3113/FAI.2012.0591.
Hintermann B, Regazzoni P, Lampert C, Stutz G, Gächter A. Arthroscopic findings in acute fractures of the ankle. J Bone Joint Surg (Br). 2000;82:345–51.
Stufkens SA, Knupp M, Horisberger M, Lampert C, Hintermann B. Cartilage lesions and the development of osteoarthritis after internal fixation of ankle fractures: a prospective study. J Bone Joint Surg Am. 2010;92:279–86. https://doi.org/10.2106/JBJS.H.01635.
Leontaritis N, Hinojosa L, Panchbhavi VK. Arthroscopically detected intra-articular lesions associated with acute ankle fractures. JBJS. 2009;91:333. https://doi.org/10.2106/JBJS.H.00584.
Bosien WR, Staples OS, Russell SW. Residual disability following acute ankle sprains. JBJS. 1955;37:1237.
Wodicka R, Ferkel E, Ferkel R. Osteochondral lesions of the ankle. Foot Ankle Int. 2016;37:1023–34. https://doi.org/10.1177/1071100716654691.
Ozal ST, Akca A, Cakmakci E. Is there a relationship between talar osteochondral lesions and foot angles? Radiol Med (Torino). 2016;121:801–4. https://doi.org/10.1007/s11547-016-0663-0.
DiGiovanni BF, Fraga CJ, Cohen BE, Shereff MJ. Associated injuries found in chronic lateral ankle instability. Foot Ankle Int. 2000;21:809–15. https://doi.org/10.1177/107110070002101003.
Ferkel RD, Chams RN. Chronic lateral instability: arthroscopic findings and long-term results. Foot Ankle Int. 2007;28:24–31. https://doi.org/10.3113/FAI.2007.0005.
Bohne WHO. Tarsal coalition. Curr Opin Pediatr. 2001;13:29–35.
Sakellariou A, Claridge RJ. Tarsal coalition: aetiology, diagnosis and treatment. Curr Orthop. 1998;12:135–42. https://doi.org/10.1016/S0268-0890(98)90069-X.
Lawrence DA, Rolen MF, Haims AH, Zayour Z, Moukaddam HA. Tarsal coalitions: radiographic, CT, and MR imaging findings. HSS J. 2014;10:153–66. https://doi.org/10.1007/s11420-013-9379-z.
Afolayan JO, Dinneen A, Sakellariou A. Tarsal coalitions – what you need to know. Orthop Traumatol. 2016;30:30–40. https://doi.org/10.1016/j.mporth.2016.02.004.
Yvars MF. Osteochondral fractures of the dome of the talus. Clin Orthop. 1976:185–91.
Slullitel PAI, Tripodi ML, Bosio ST, Puigdevall M, Maenza R. Massive osteochondral lesion of the talus in a skeletally immature patient associated with a tarsal coalition and valgus hindfoot. J Foot Ankle Surg. 2017;56:1257–62. https://doi.org/10.1053/j.jfas.2017.04.025.
Lamb D. The ball and socket ankle joint; a congenital abnormality. J Bone Joint Surg (Br). 1958;40-B:240–3.
Smet AAD, Ilahi OA, Graf BK. Reassessment of the MR criteria for stability of osteochondritis dissecans in the knee and ankle. Skelet Radiol. 1996;25:159–63. https://doi.org/10.1007/s002560050054.
Hepple S, Winson IG, Glew D. Osteochondral lesions of the talus: a revised classification. Foot Ankle Int. 1999;20:789–93. https://doi.org/10.1177/107110079902001206.
Elias I, Jung JW, Raikin SM, Schweitzer MW, Carrino JA, Morrison WB. Osteochondral lesions of the talus: change in MRI findings over time in talar lesions without operative intervention and implications for staging systems. Foot Ankle Int. 2006;27:157–66. https://doi.org/10.1177/107110070602700301.
You JY, Lee GY, Lee JW, Lee E, Kang HS. An osteochondral lesion of the distal tibia and fibula in patients with an osteochondral lesion of the talus on MRI: prevalence, location, and concomitant ligament and tendon injuries. AJR Am J Roentgenol. 2016;206:366–72. https://doi.org/10.2214/AJR.15.14861.
Carrara C, Caravaggi P, Belvedere C, Leardini A. Radiographic angular measurements of the foot and ankle in weight-bearing: a literature review. Foot Ankle Surg. 2020;26:509–17. https://doi.org/10.1016/j.fas.2019.07.008.
Abousayed M, Alley M, Shakked R, Rosenbaum A. Adult-acquired flatfoot deformity. Jbjs Rev. 2017;5. https://doi.org/10.2106/JBJS.RVW.16.00116.
Lee KM, Chung CY, Park MS, Lee SH, Cho JH, Choi IH. Reliability and validity of radiographic measurements in hindfoot varus and valgus. J Bone Joint Surg Am. 2010;92:2319–27. https://doi.org/10.2106/JBJS.I.01150.
Newman JS, Newberg AH. Congenital tarsal coalition: multimodality evaluation with emphasis on CT and MR imaging. RadioGraphics. 2000;20:321–32. https://doi.org/10.1148/radiographics.20.2.g00mc03321.
Zhou B, Tang K, Hardy M. Talocalcaneal coalition combined with flatfoot in children: diagnosis and treatment: a review. J Orthop Surg. 2014;9. https://doi.org/10.1186/s13018-014-0129-9.
Lemley F, Berlet G, Hill K, Philbin T, Isaac B, Lee T. Current concepts review: tarsal coalition. Foot Ankle Int. 2006;27:1163–9. https://doi.org/10.1177/107110070602701229.
Bauer M, Jonsson K, Linden B. Osteochondritis dissecans of the ankle. A 20-year follow-up study. J Bone Joint Surg (Br). 1987;69-B:93–6. https://doi.org/10.1302/0301-620X.69B1.3818743.
Lambers KTA, Saarig A, Turner H, Stufkens SAS, Doornberg JN, Kerkhoffs GMMJ, et al. Prevalence of osteochondral lesions in rotational type ankle fractures with syndesmotic injury. Foot Ankle Int. 2019;40:159–66. https://doi.org/10.1177/1071100718804818.
Brahme F. Upper talar enarthrosis. Acta Radiol. 1961;(os-55):221–4. https://doi.org/10.1177/028418516105500307.
Jastifer JR, Gustafson PA, Labomascus A, Snoap T. Ball and socket ankle: mechanism and computational evidence of concept. J Foot Ankle Surg. 2017;56:773–5. https://doi.org/10.1053/j.jfas.2017.02.019.
Hutchinson ID, Baxter JR, Gilbert S, Hogan MV, Ling J, Saunders SM, et al. How do hindfoot fusions affect ankle biomechanics: a cadaver model. Clin Orthop. 2016;474:1008–16. https://doi.org/10.1007/s11999-015-4671-5.
Acknowledgements
The authors would like to thank their mentors for teaching them tools to practice their profession.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Cheng, K.Y., Fuangfa, P., Shirazian, H. et al. Osteochondritis dissecans of the talar dome in patients with tarsal coalition. Skeletal Radiol 51, 191–200 (2022). https://doi.org/10.1007/s00256-021-03800-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-021-03800-0