
Abstract
Background
Intussusception is a common pediatric abdominal emergency, treated with image-guided reduction. Available techniques include fluoroscopic and ultrasonographic monitoring of liquid and air.
Objective
The purpose of this study was to determine current practices and establish trends by comparing our findings with reports of previous surveys.
Materials and methods
This study is based on an e-mail survey sent to all 1,538 members of the Society for Pediatric Radiology. It included questions about demographics, presence of parents/surgeon during procedure, patient selection/preparation, use of sedation, preferred methods of reduction and technical details, approach to unsuccessful reduction, and self-reported incidence of success/perforation.
Results
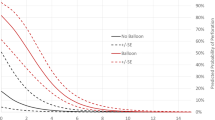
The 456 respondents (30%) reported attempting 3,834 reductions in the preceding 12 months. Of these, 96% use fluoroscopy and 4% use US guidance for reduction; 78% use air, 20% prefer fluid; 75% require intravenous access; 63% expect a surgeon to be present in hospital; 93% do not sedate. Although inflating a rectal balloon is controversial, 39% do so, and 50% employ a pressure-release valve. Seventy-two percent attempt reductions three times in the same position. In case of unsuccessful reductions, 64% wait and re-attempt later, 19% apply manual pressure, and 15% try again in left decubitus position. About 20% reattempt reduction after waiting 2 h or more.
Conclusion
By providing a better understanding of both trends in and diversity of current practice, we hope to increase the confidence with which the individual practitioner will approach each case.


Similar content being viewed by others


References
Bisset GS 3rd, Kirks DR (1988) Intussusception in infants and children: diagnosis and therapy. Radiology 168:141–145
Daneman A, Navarro O (2004) Intussusception. Part 2: an update on the evolution of management. Pediatr Radiol 34:97–108, quiz 187
Del-Pozo G, Albillos JC, Tejedor D et al (1999) Intussusception in children: current concepts in diagnosis and enema reduction. Radiographics 19:299–319
McAlister WH (1998) Intussusception: even hippocrates did not standardize his technique of enema reduction. Radiology 206:595–598
McDermott VG (1994) Childhood intussusception and approaches to treatment: a historical review. Pediatr Radiol 24:153–155
Davis CF, McCabe AJ, Raine PA (2003) The ins and outs of intussusception: history and management over the past fifty years. J Pediatr Surg 38:60–64
Daneman A, Alton DJ (1996) Intussusception. Issues and controversies related to diagnosis and reduction. Radiol Clin North A 34:743–756
Ko HS, Schenk JP, Troger J et al (2007) Current radiological management of intussusception in children. Eur Radiol 17:2411–2421
Peh WC, Khong PL, Chan KL et al (1996) Sonographically guided hydrostatic reduction of childhood intussusception using Hartmann’s solution. AJR Am J Roentgenol 167:1237–1241
Khong PL, Peh WC, Lam CH et al (2000) Ultrasound-guided hydrostatic reduction of childhood intussusception: technique and demonstration. Radiographics 20:E1
Meyer JS, Dangman BC, Buonomo C et al (1993) Air and liquid contrast agents in the management of intussusception: a controlled, randomized trial. Radiology 188:507–511
Hadidi AT, El Shal N (1999) Childhood intussusception: a comparative study of nonsurgical management. J Pediatr Surg 34:304–307
Shiels WE 2nd, Maves CK, Hedlund GL et al (1991) Air enema for diagnosis and reduction of intussusception: clinical experience and pressure correlates. Radiology 181:169–172
Curtis JL, Gutierrez IM, Kirk SR et al (2010) Failure of enema reduction for ileocolic intussusception at a referring hospital does not preclude repeat attempts at a children’s hospital. J Pediatr Surg 45:1178–1181
Blanch AJ, Perel SB, Acworth JP (2007) Paediatric intussusception: epidemiology and outcome. Emerg Med Austalas 19:45–50
Campbell JB (1989) Contrast media in intussusception. Pediatr Radiol 19:293–296
Meyer JS (1992) The current radiologic management of intussusception: a survey and review. Pediatr Radiol 22:323–325
Katz ME, Kolm P (1992) Intussusception reduction 1991: an international survey of pediatric radiologists. Pediatr Radiol 22:318–322
Schmit P, Rohrschneider WK, Christmann D (1999) Intestinal intussusception survey about diagnostic and nonsurgical therapeutic procedures. Pediatr Radiol 29:752–761
Jewell FM, Roobottom C, Duncan A (1995) Variations in the radiological management of intussusception: results of a postal survey. Br J Radiol 68:13–18
Rosenfeld K, McHugh K (1999) Survey of intussusception reduction in England, Scotland and Wales: how and why we could do better. Clin Radiol 54:452–458
Hannon E, Williams R, Allan R et al (2014) UK intussusception audit: a national survey of practice and audit of reduction rates. Clin Radiol 69:344–349
Stephenson CA, Seibert JJ, Strain JD et al (1989) Intussusception: clinical and radiographic factors influencing reducibility. Pediatr Radiol 20:57–60
Barr LL, Stansberry SD, Swischuk LE (1990) Significance of age, duration, obstruction and the dissection sign in intussusception. Pediatr Radiol 20:454–456
Gorenstein A, Raucher A, Serour F et al (1998) Intussusception in children: reduction with repeated, delayed air enema. Radiology 206:721–724
Tareen F, Ryan S, Avanzini S et al (2011) Does the length of the history influence the outcome of pneumatic reduction of intussusception in children? Pediatr Surg Int 27:587–589
Fike FB, Mortellaro VE, Holcomb GW 3rd et al (2012) Predictors of failed enema reduction in childhood intussusception. J Pediatr Surg 47:925–927
Del-Pozo G, Gonzalez-Spinola J, Gomez-Anson B et al (1996) Intussusception: trapped peritoneal fluid detected with US — relationship to reducibility and ischemia. Radiology 201:379–383
Britton I, Wilkinson AG (1999) Ultrasound features of intussusception predicting outcome of air enema. Pediatr Radiol 29:705–710
Kong MS, Wong HF, Lin SL et al (1997) Factors related to detection of blood flow by color Doppler ultrasonography in intussusception. J Ultrasound Med 16:141–144
Touloukian RJ, O’Connell JB, Markowitz RI et al (1987) Analgesic premedication in the management of ileocolic intussusception. Pediatrics 79:432–434
Ilivitzki A, Shtark LG, Arish K et al (2012) Deep sedation during pneumatic reduction of intussusception. Pediatr Radiol 42:562–565
Hsiao JY, Kao HA, Shih SL (1988) Intravenous glucagon in hydrostatic reduction of intussusception: a controlled study of 63 patients. Zhonghua Minguo Xiao Er Ke Yi Xue Hui 29:242–247
Franken EA Jr, Smith WL, Chernish SM et al (1983) The use of glucagon in hydrostatic reduction of intussusception: a double-blind study of 30 patients. Radiology 146:687–689
Schmitz-Rode T, Müller-Leisse C, Alzen G (1991) Comparative examination of various rectal tubes and contrast media for the reduction of intussusceptions. Pediatr Radiol 21:341–345
Daneman A, Alton DJ, Ein S et al (1995) Perforation during attempted intussusception reduction in children — a comparison of perforation with barium and air. Pediatr Radiol 25:81–88
Phelan E, de Campo JF, Malecky G (1988) Comparison of oxygen and barium reduction of ileocolic intussusception. AJR Am J Roentgenol 150:1349–1352
Beres AL, Baird R (2013) An institutional analysis and systematic review with meta-analysis of pneumatic versus hydrostatic reduction for pediatric intussusception. Surgery 154:328–334
Sargent MA, Wilson BP (1991) Are hydrostatic and pneumatic methods of intussusception reduction comparable? Pediatr Radiol 21:346–349
Grasso SN, Katz ME, Presberg HJ et al (1994) Transabdominal manually assisted reduction of pediatric intussusception: reappraisal of this historical technique. Radiology 191:777–779
Vazquez JL, Ortiz M, Doniz MC et al (2012) External manual reduction of paediatric idiopathic ileocolic intussusception with US assistance: a new, standardised, effective and safe manoeuvre. Pediatr Radiol 42:1197–1204
Vazquez JL, Ortiz M, Doniz MC et al (2012) External manual reduction of paediatric idiopathic ileocolic intussusception with ultrasound assistance. Pediatr Radiol 42:1195–1196
Saxton V, Katz M, Phelan E et al (1994) Intussusception: a repeat delayed gas enema increases the nonoperative reduction rate. J Pediatr Surg 29:588–589
Connolly B, Alton DJ, Ein SH et al (1995) Partially reduced intussusception: when are repeated delayed reduction attempts appropriate? Pediatr Radiol 25:104–107
Acknowledgments
We would like to acknowledge the assistance of Dr. Mark Lubell, Department of Environmental Science and Policy, University of California, Davis, in developing the survey.
Conflicts of interest
Dr. Stein-Wexler has a small financial interest in Lucy LLC, a company that produces a simulation device for learning intussusception reduction.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Stein-Wexler, R., O’Connor, R., Daldrup-Link, H. et al. Current methods for reducing intussusception: survey results. Pediatr Radiol 45, 667–674 (2015). https://doi.org/10.1007/s00247-014-3214-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-014-3214-7