
Abstract
Atrial septal defect (ASD) is characterized by a left-to-right shunt causing dilatation of the right atrium and right ventricle as well as pulmonary hyperperfusion. The detection of ASDs often occurs late in childhood or adulthood. Little is known about cardiac structure and function in neonates with ASD.
We analyzed neonatal echocardiograms from the Copenhagen Baby Heart Study, a multicenter, population-based cohort study of 27,595 neonates. We included 716 neonates with secundum-type ASDs and matched them 1:1 on sex and age at examination with neonates without ASD from the same birth cohort. Neonates with an ASD (median age 11 days, 52% female) had larger right ventricular (RV) dimensions than matched controls (RV longitudinal dimension end-diastole: 27.7 mm vs. 26.7 mm, p < 0.001; RV basal dimension end-diastole: 14.9 mm vs. 13.8 mm, p < 0.001; and RV outflow tract diameter 13.6 mm vs. 12.4 mm, p < 0.001). Atrial volumes were larger in neonates with ASD compared to controls (right atrial end-systolic volume: 2.9 ml vs. 2.1 ml, p < 0.001; and left atrial end-systolic volume 2.0 ml vs. 1.8 ml, p < 0.001). Tricuspid annular plane systolic excursion was larger in neonates with ASD than in controls (10.2 mm vs. 9.6 mm, p < 0.001). Left ventricular dimensions and function did not differ between neonates with ASD and controls. In conclusion, ASDs were associated with altered cardiac dimensions already in the neonatal period, with larger right ventricular dimensions and larger atrial volumes at echocardiography within the first 30 days after birth.
ClinicalTrials.gov Identifier: NCT02753348 (April 27, 2016).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Atrial septal defects (ASD) are among the most common congenital heart defects. The morphological defect in the atrial septum will in most cases lead to a left-to-right shunt, due to higher pressure in the left atrium. The shunt results in an increased volume load on the right side of the heart. By the time of diagnosis, several other morphological changes in the heart are frequently found. Right ventricular dilatation and right atrial enlargement are among the most common changes [1]. Due to the natural history and clinical presentation, the diagnosis of a clinically significant ASD often does not occur until late in childhood or even adulthood [2]. The decision on whether and when to close a defect depends on several factors such as symptoms, the occurrence of paradoxical embolism, the ratio of pulmonary to systemic blood flow (Qp:Qs), and whether right-sided chambers are dilated, although the available evidence is sparse [3, 4].
Little is known about cardiac structure very early in life in patients with ASD since symptoms and diagnosis often occur later [5]. In utero, all fetuses have an interatrial communication, the foramen ovale, which allows for oxygenated blood from the placenta to be shunted from right to left, bypassing the pulmonary circulation. After birth, the expansion of the lungs and the decrease in pulmonary vascular resistance lead to increased pulmonary blood flow and rising pressure in the left atrium. The pressure changes cause the septum primum to cover the foramen ovale like a flap, closing the interatrial communication [6]. In neonates with ASD, however, these physiological changes in the cardiovascular system will reverse the shunt to left to right across the atrial septum. This transition occurs after birth, but it is unclear how rapidly the shunting affects the right-sided chambers and leads to structural changes.
This study aims to investigate if cardiac morphology and function in patients with ASD are different from matched controls as early as within the first month after birth. We explore this topic by examining an unselected cohort of neonates with ASD found in a large echocardiographic screening study of neonates.
Material and Methods
We conducted a case–control study of echocardiographic parameters in neonates with ASD included in the Copenhagen Baby Heart Study.
Copenhagen Baby Heart Study
The Copenhagen Baby Heart Study (CBHS) is a multicenter, population-based cohort study with prenatal inclusion. All expectant parents in the Capital Region of Denmark were offered inclusion in the study in the period April 1st, 2016, to October 31st, 2018 [7]. A total of 27,595 neonates were included in the study, whereof 25,590 underwent transthoracic echocardiography within the first 60 days after birth. Information on maternal and infant characteristics was retrieved from medical records and health registries and stored in the CBHS database [8]. The CBHS study cohort is intended to undergo lifelong follow-up.
Acquisition of Neonatal Echocardiograms
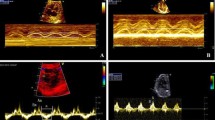
In the CBHS, the neonatal echocardiographies were performed by sonographers and specialists trained in pediatric echocardiography using Vivid E9 ultrasound equipment (GE Vingmed Ultrasound, Horten, Norway). The CBHS echocardiographic protocol was established in accordance with the American Society of Echocardiography’s guidelines for pediatric echocardiography [9] and has been described in detail previously [7]. Cardiac sector transducers 12S-D and 6S-D were used to obtain standard subxiphoid, apical, left parasternal, and suprasternal views.
Parents who had given consent to be included in CBHS were reminded by text message after giving birth to a live-born infant and booked an appointment for the echocardiographic examination using a secure website. Neonatal echocardiograms in CBHS were performed while the infants were calm or sleeping.
Analysis of Echocardiograms for Interatrial Communications
After the inclusion period, echocardiograms were reviewed offline using EchoPAC clinical software (version 113, GE Vingmed Ultrasound, Horten, Norway). To determine whether neonates had an ASD, two investigators systematically analyzed subxiphoid echocardiographic images of the atrial septum using a novel algorithm for the echocardiographic assessment of interatrial communications that was developed and validated in the CBHS and was recently published [10]. Categorization of interatrial communications was based on several echocardiographic criteria: We defined neonates as having an ASD in cases when color Doppler flow was crossing the atrial septum and when cross-sectional images showed either multiple visible communications (fenestrated ASD) or a single-visible communication with either a diameter of ≥ 4 mm or a location in the inferior part of the atrial septum. For interatrial communications with one single-visible communication on cross-sectional images, the diameter of the defect was measured.
Study Cohort
Neonates with ASD were matched 1:1 with controls from the CBHS study cohort on sex and age at the time of echocardiographic examination. We excluded neonates with syndromes, chromosomal abnormalities, or other congenital heart disease.
Measurement of Echocardiographic Parameters
For this study, we chose to investigate echocardiographic parameters of particular interest in patients with ASD. Namely, we investigated right ventricular (RV) dimensions (RV longitudinal dimension end-diastole; RV basal dimension end-diastole, and RV outflow tract (RVOT) diameter), tricuspid annular plane systolic excursion (TAPSE), atrial volumes (right atrial end-systolic volume (RAESV); left atrial end-systolic volume (LAESV)), left ventricular dimensions (left ventricular internal diameter end-diastole (LVIDd); left ventricular internal diameter end-systole (LVIDs); left ventricular posterior wall end-systole (LVPWs); left ventricular outflow tract(LVOT); interventricular septum end-diastole (IVSd)) as well as diameters for the inferior vena cava (IVC), and the main pulmonary artery (MPA). We also measured left ventricular ejection fraction (LVEF) and fractional shortening (FS). Measurements and analyses of echocardiographic parameters were done in accordance with the Recommendations for Quantification Methods During the Performance of a Pediatric Echocardiogram from the American Society of Echocardiography [11]. For the assessment of right ventricular dimensions that were not elaborately described in pediatric guidelines, we followed the Guidelines for the Echocardiographic Assessment of the Right Heart in Adults from the American Society of Echocardiography [12]. For details on echocardiographic parameters, see Supplementary Table 4.
Analyses and measurements of echocardiographic outcome parameters were made by two investigators blinded to the presence of ASD, as they did not assess images of the atrial septum with Color Doppler. Echocardiograms from neonates with ASD and matched controls were randomly distributed between the two investigators. Echocardiographic analyses were frequently supervised by a third investigator to minimize the risk of inter- and intraobserver variability.
Statistical Analyses
Continuous variables are presented as mean values (SD) or median values (IQR), where appropriate. Categorical variables are presented as absolute numbers (percentages). Comparison between cases (neonates with ASD) and matched controls was performed using Student’s t test. Bonferroni’s correction for multiple testing was applied, and p values < 0.003 were considered statistically significant (analyses for 15 echocardiographic parameters: p 0.05 / 15 = 0.003).
We performed subgroup analyses on the influence of the size of the ASD, the neonates’ age at examination, and the influence of fenestrated defects vs. single defects. For analyses on the influence size of the ASD, we looked further into the subgroup where the ASD diameter measurement was feasible. We plotted the echocardiographic outcome variables that showed a difference in means between neonates with ASD and controls in the main analysis against the ASD diameters to identify potential associations and applied a linear regression model with a 95% confidence interval. For subgroup analyses on the neonates’ age at examination, we compared neonates examined at age 0–7 days old with neonates examined at age 8–30 days old. For analyses on the influence of fenestrated defects, we performed analyses on a subgroup of neonates with ASD, who had complete data on all RV parameters and atrial volumes. We compared the echocardiographic outcome variables that differed between neonates with ASD and controls in the main analysis using Student’s t test with Bonferroni’s correction for multiple testing.
Statistical analyses were performed using R statistical software v. 1.2.1335 (Boston, MA, USA).
Results
Study Cohort
We included 716 neonates with secundum-type ASD (52% female, mean age at examination 11 days) and 716 controls matched on sex and age at examination. Descriptive characteristics are shown in Table 1. Neonates with ASD and controls were comparable with regard to gestational age at birth, birth weight and length, and body surface area.
The direction of shunting in neonates with ASD was left-to-right in the majority of cases (n = 644; 90%), while a smaller proportion of neonates had an additional component of right-to-left shunting (n = 72; 10%). None of the neonates had exclusively right-to-left shunting.
Echocardiographic Parameters
Neonates with ASDs had larger RV basal diameter at end-diastole than controls as well as larger RV longitudinal dimensions. End-systolic atrial volumes were larger in neonates with ASD than in controls for both the right atrium and left atrium. Right ventricular outflow tract diameter was larger in neonates with ASD than in controls, while MPA diameter was slightly larger but did not reach statistical significance after Bonferroni correction. The tricuspid annular plane systolic excursion was larger in neonates with ASD compared to controls. Left ventricular dimensions, LV function, the IVSd, and LVOT diameter did not differ between neonates with ASD and controls; neither did the diameter of IVC at expiration. Echocardiographic characteristics for neonates with ASD and matched controls are shown in Table 2.
Influence of the Size of the ASD
Of the 716 neonates with ASD, measurement of the septal defect diameter was feasible in 348 neonates with regard to the used algorithm for the assessment of interatrial communications [10]. The mean diameter of the defects was 4.4 mm (range 3.5–10.5 mm).
Echocardiographic values for parameters that differed between neonates with ASD and controls (RV longitudinal dimension end-diastole, RV basal dimension end-diastole, RVOT, TAPSE, LAESV, and RAESV) were plotted against the size of the ASD and are shown in Supplementary Fig. 2. No clear correlation between the size of the defect and the increase in right ventricular dimensions or atrial volumes was seen. However, when fitting linear regression models to the plots, a slight positive association between the diameter of ASD and RAESV was found (p = 0.02). TAPSE also increased slightly with increasing diameter of ASD (p = 0.01).
Influence of the Neonatal Age at Examination
To investigate whether differences in echocardiographic parameters between neonates with and without ASD were present at birth or developed during the first month of life, we divided the cohort into two subgroups based on the neonates’ age at examination. Specifically, we compared neonates with ASD examined during the first week after birth (0 to 7 days old) with neonates from the control group examined at the same age. Likewise, we compared neonates with ASD examined at age 8 to 30 days with controls (Table 3).
For the echocardiographic parameters that showed differences in means between neonates with ASD and controls in the main analyses, the majority also differed between groups in this subgroup analysis at either age at examination. The exception from this was RV longitudinal dimension end-diastole which did not differ between cases and controls during the first week after birth.
Influence of Fenestrated Defects vs. Single Defects
We found no differences in right ventricular dimensions or atrial volumes between neonates with single defects (n = 139) and neonates with fenestrated defects (n = 134) apart from a slightly larger RAESV in neonates with single defects compared to neonates with fenestrated defects (2.9 ml. vs. 2.6 ml, p = 0.006; p < 0.008 considered statically significant after Bonferroni correction; data not shown).
Discussion
This is the largest study to date examining cardiac structure and function in neonates with secundum-type ASD. Neonates with ASD exhibited larger dimensions of the RV, the RVOT, and both atria as early as within the first month after birth. We demonstrated this through echocardiography in a cohort of 716 neonates with ASD, as compared to a control group of 716 neonates without ASD.
The dimensions of the right heart chambers are included in the evaluation of the hemodynamic significance of an ASD. These structural changes are considered secondary to the ASD and the changes in blood flow, but it remains unknown at which timepoint the pathophysiological changes occur [13, 14]. Our results indicate that the morphological changes occur very early in the neonate, after only a few days of shunting over the ASD.
In the fetal circulation, both the physiological foramen ovale and the abnormal ASD allow for right-to-left shunting. Hence, in utero, there should be no significant differences in blood flow between fetuses with the physiological foramen ovale and fetuses with an ASD. At the transition to postnatal life, the pulmonary circulation opens, with a significant reduction in pulmonary vascular resistance and a redirection of blood flow through the lungs and back into the left atrium. Normally, the primum septum acting as a flap will close the interatrial communication, and the circulation will continue as a parallel circulation with almost equal volumes on the left and the right sides. In the situation of an ASD, however, a defect remains, through which the right atrium will receive a larger volume of blood. The immediate effect of an increased blood flow and volume load in a compliant system will be dilatation. In our subgroup analyses, we looked specifically at neonates with an ASD aged 0–7 days at the time of echocardiographic examination and found likewise the right atrium and RV to be larger than in matched controls. These results emphasize that only a few days of left-to-right shunting over the ASD have an impact on the right-sided chambers.
In adults, the compliance of the ventricles decreases with increasing age [15, 16]. In the fetal heart, compliance is considerably lower than in adults, while in the neonatal heart, the compliance of the ventricles is higher than in fetal state, yet lower than in adults. The RV has a higher compliance than the LV regardless of age [17]. A possible explanation for the lower compliance in the neonatal heart might be a relatively high amount of collagen, especially type I collagen, mainly providing rigidity [18]. As a result of the relatively low compliance, the intraventricular pressure and wall tension will rise comparably fast in response to volume overload in the neonatal heart. The left-to-right shunt in ASD causes a volume overload on the right side of the heart, and from our results, we can hypothesize that the resulting increase in pressure and wall tension will lead to morphological changes even in the presence of small shunts and even after only a few days of shunting.
The RVOT is recommended to be part of the assessment of the RV in adults [12] but normative data on infants and children are limited. In accordance with our findings, Koestenberger et al. showed RVOT diameter to be enlarged in children with secundum ASD (n = 115, age range 2 days–18 years) [19]. An increased pulmonary blood flow in patients with ASD will over time possibly lead to enlargement of the MPA as well. In our results, the MPA diameter was slightly larger in neonates with ASDs but did not reach statistical significance after Bonferroni correction.
TAPSE is a recommended tool for assessing right ventricular systolic function in standard echocardiographic exams [11], even though its clinical significance in pediatric patients is not well established. We found TAPSE to be larger in neonates with ASD than in controls although the mean values for both groups were within previously published normal ranges for TAPSE in neonates [20]. Koestenberger et al. investigated TAPSE in patients with unrepaired isolated secundum ASDs (n = 200, age range 0–21 years) and found no significant difference when compared to a control group [21]. In accordance with our findings, Arce et al. looked specifically at the longitudinal motion of the atrioventricular annuli in children including a group with right ventricular overload due to ASD (n = 25, age range 1–37 years) and found an exaggerated normal pattern of movement with a higher than normal absolute and percentual displacement of the tricuspid lateral ring [22].
We also found the left atrial volume to be larger in neonates with ASDs than in neonates without ASD. Left atrial enlargement in patients with ASD has previously been described as a consequence of the volume overload similar to right-sided enlargements [23]. An alternative pathophysiological hypothesis could be a primary dilatation of the atria in utero. In the stretched atrial wall, the septum primum may not sufficiently cover the foramen ovale, leading to a secundum-type ASD.
The dimensions and function of the LV, LVOT, and interventricular septum did not differ between neonates with ASD and controls, which is in accordance with earlier studies [24].
A limitation of all echocardiographic studies includes interobserver variability. For the present study, we sought to minimize interobserver variability by having the echocardiographic analyses performed by only two investigators, who had received equal training and a thorough introduction to the measurements and methods used for this study. Also, the investigators were blinded to whether the neonates had an ASD or not, by not accessing the images with color Doppler over the atrial septum. Repeatability and reproducibility of neonatal echocardiography in the CBHS have previously been tested, showing good inter- and intraobserver agreement for most measurements [25]. Potential limitations of the CBHS data and cohort have been discussed previously [7, 8]. Neonates born preterm were under-represented in the CBHS cohort, limiting the generalizability of results to preterm infants.
The CBHS is presenting robust echocardiographic data on the largest cohort of neonates to date. Neonatal echocardiograms of > 25,000 neonates were performed, using a TTE protocol in accordance with international standards. However, as the cohort was not specifically set up for the assessment of children with shunts, we have limited data on right-sided dimensions. Echocardiographic techniques are steadily being improved with advanced analyses being made possible by for example 3D echocardiography and strain imaging [26]. For optimal assessment of right ventricular dimensions, magnetic resonance imaging would also have been preferred since it is considered the gold standard and superior to echocardiography [27].
The neonates included in our study were not diagnosed with ASD due to symptoms but found this early after birth because they were part of a large population-based cohort study with echocardiographic examination. This unselected cohort of neonates with ASD is unique, allowing us to report echocardiographic characteristics in neonates with and without ASD from the same birth cohort.
In our subgroup analyses, we found a slight positive association between the diameter of the ASD and RAESV, and TAPSE, but no clear pattern for the other echocardiographic variables. Studies specifically on cohorts of patients with small ASDs show that morbidity and mortality are seen even in cases where the ASD is considered small and hemodynamically insignificant [28,29,30,31].
The cohort of neonates with ASD in the present study might include neonates where the defects are both asymptomatic and smaller than usually seen in clinical settings. The reported morphological differences between neonates with ASD and controls found in this study may be relatively small in absolute numbers but reached convincing statistical significance due to a large number of included subjects. However, the study design with the large cohort of neonates in the CBHS and the method with thorough and blinded echocardiographic analyses for this present study validate our findings and make up the strengths of our study. This new knowledge of early morphological changes contributes to our pathophysiological and anatomical understanding of ASDs.
Conclusion
Neonates aged 0–30 days with ASDs had larger right ventricular dimensions and larger atrial volumes than matched controls. These findings indicate that the morphological cardiac changes typical for ASDs are found very early in life after only a few days of left-to-right shunting.
Data Availability
The data that support the findings of this study are not publicly available due to the privacy of research participants. The data will be shared upon reasonable request to the corresponding author.
References
Akula VS, Durgaprasad R, Velam V, Kasala L, Rodda M, Erathi HV (2016) Right ventricle before and after atrial septal defect device closure. Echocardiography 33:1381–1388. https://doi.org/10.1111/echo.13250
Campbell M (1970) Natural history of atrial septal defect. Br Heart J 32:820. https://doi.org/10.1136/hrt.32.6.820
Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, Colman JM, Crumb SR, Dearani JA, Fuller S, Gurvitz M, Khairy P, Landzberg MJ, Saidi A, Valente AM, Van Hare GF (2019) 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol 73:e698–e800. https://doi.org/10.1016/j.jacc.2018.08.1029
Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller GP, Lung B, Kluin J, Lang IM, Meijboom F, Moons P, Mulder BJM, Oechslin E, Roos-Hesselink JW, Schwerzmann M, Sondergaard L, Zeppenfeld K, Ernst S, Ladouceur M, Aboyans V, Alexander D, Christodorescu R, Corrado D, D’Alto M, De Groot N, Delgado V, Di Salvo G, Dos Subira L, Eicken A, Fitzsimons D, Frogoudaki AA, Gatzoulis M, Heymans S, Hörer J, Houyel L, Jondeau G, Katus HA, Landmesser U, Lewis BS, Lyon A, Mueller CE, Mylotte D, Petersen SE, Sonia Petronio A, Roffi M, Rosenhek R, Shlyakhto E, Simpson IA, Sousa-Uva M, Torp-Pedersen CT, Touyz RM, Van De Bruaene A, Babu-Narayan SV, Budts W, Chessa M, Diller GP, Iung B, Kluin J, Lang IM, Meijboom F, Moons P, Mulder BJM, Oechslin E, Roos-Hesselink JW, Schwerzmann M, Sondergaard L, Zeppenfeld K (2021) 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J 42:563–645. https://doi.org/10.1093/eurheartj/ehaa554
Hanséus K, Björkhem G, Lundström NR (1988) Soeroso S (1988) Cross-sectional echocardiographic measurement of right atrial and right ventricular size in children with atrial septal defect before and after surgery. Pediatr Cardiol 94(9):231–236. https://doi.org/10.1007/BF02078414
Rudolph AM (1970) The changes in the circulation after birth. Their importance in congenital heart disease. Circulation 41:343–359. https://doi.org/10.1161/01.CIR.41.2.343
Sillesen A-S, Raja AA, Pihl C, Vøgg ROB, Hedegaard M, Emmersen P, Sundberg K, Tabor A, Vedel C, Zingenberg H, Kruse C, Wilken-Jensen C, Nielsen TH, Jørgensen FS, Jeppesen DL, Søndergaard L, Kamstrup PR, Nordestgaard BG, Frikke-Schmidt R, Vejlstrup N, Boyd HA, Bundgaard H, Iversen K (2019) Copenhagen Baby Heart Study: a population study of newborns with prenatal inclusion. Eur J Epidemiol 34:79–90. https://doi.org/10.1007/s10654-018-0448-y
Vøgg ROB, Basit S, Raja AA, Sillesen A-S, Pihl C, Vejlstrup N, Jonsen EH, Larsen OW, Zingenberg H, Boyd HA, Iversen KK, Bundgaard H (2021) Cohort profile: the Copenhagen Baby Heart Study (CBHS). Int J Epidemiol 2021:1–15. https://doi.org/10.1093/IJE/DYAB147
Lai WW, Geva T, Shirali GS, Frommelt PC, Humes RA, Brook MM, Pignatelli RH, Rychik J (2006) Guidelines and standards for performance of a pediatric echocardiogram: a report from the task force of the Pediatric Council of the American Society of Echocardiography. J AM Soc Echocardiogr. https://doi.org/10.1016/j.echo.2006.09.001
Dannesbo S, Blixenkrone-Moeller E, Pihl CA, Sillesen A-S, Voegg ROB, Davidsen AS, Lind LE, Jeppesen DL, Kruse C, Noerager B, Dodd JK, Jorgensen FS, Raja AA, Colan SD, Mertens L, Hjortdal VE, Vejlstrup N, Anderson RH, Bundgaard H, Iversen K (2022) A novel algorithm for classification of interatrial communications within the oval fossa in the newborn - Results from the Copenhagen Baby Heart Study. Accepted for publication Oct 2022. Cardiol Young 1–8. https://doi.org/10.1017/S1047951122003365
Lopez L, Colan SD, Frommelt PC, Ensing GJ, Kendall K, Younoszai AK, Lai WW, Geva T, York N (2010) Recommendations for quantification methods during the performance of a pediatric echocardiogram: a report from the pediatric measurements writing group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J Am Soc Echocardiogr 23:465–495. https://doi.org/10.1016/j.echo.2010.03.019
Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB, York N (2010) Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography Endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr 23:685–713. https://doi.org/10.1016/j.echo.2010.05.010
Aǧaç MT, Akyüz AR, Acar Z, Akdemir R, Korkmaz L, Kíríş A, Erkuş E, Erkan H, Çelik Ş (2012) Evaluation of right ventricular function in early period following transcatheter closure of atrial septal defect. Echocardiography 29:358–362. https://doi.org/10.1111/j.1540-8175.2011.01558.x
Jost CHA, Oechslin E, Seifert B, Maly F, Fatio R, Turina J, Jenni R (2002) Remodelling after surgical repair of atrial septal defects within the oval fossa. Cardiol Young 12:506–512. https://doi.org/10.1017/S1047951102000926
Fujimoto N, Hastings JL, Bhella PS, Shibata S, Gandhi NK, Carrick-Ranson G, Palmer D, Levine BD (2012) Effect of ageing on left ventricular compliance and distensibility in healthy sedentary humans. J Physiol C 590:1871–1880. https://doi.org/10.1113/jphysiol.2011.218271
Arbab-Zadeh A, Dijk E, Prasad A, Fu Q, Torres P, Zhang R, Thomas JD, Palmer D, Levine BD (2004) Effect of aging and physical activity on left ventricular compliance. Circulation 110:1799–1805. https://doi.org/10.1161/01.CIR.0000142863.71285.74
Desai A, Macrae D (2022) Cardiovascular Physiology in Infants and Children. In: da Cruz EM, Ivy D, Hraska V, Jaggers J (eds). Pediatric and Congenital Cardiology, Cardiac Surgery and Intensive Care. Springer, London
Marijianowski MMH, van der Loos CM, Mohrschladt MF, Becker AE (1994) The neonatal heart has a relatively high content of total collagen and type I collagen, a condition that may explain the less compliant state. J Am Coll Cardiol 23:1204–1208. https://doi.org/10.1016/0735-1097(94)90612-2
Koestenberger M, Ravekes W, Avian A, Grangl G, Burmas A, Raith W, Cvirn G, Grillitsch M, Gamillscheg A (2016) Right Ventricular Outflow Tract (RVOT) changes in children with an atrial septal defect: focus on RVOT velocity time integral, RVOT diameter, and RVOT systolic excursion. Echocardiography 33:1389–1396. https://doi.org/10.1111/echo.13246
Koestenberger M, Ravekes W, Everett AD, Stueger HP, Heinzl B, Gamillscheg A, Cvirn G, Boysen A, Fandl A, Nagel B (2009) Right ventricular function in infants, children and adolescents: reference values of the Tricuspid Annular Plane Systolic Excursion (TAPSE) in 640 healthy patients and calculation of z score values. J Am Soc Echocardiogr 22:715–719. https://doi.org/10.1016/j.echo.2009.03.026
Koestenberger M, Nagel B, Ravekes W, Everett AD, Stueger HP, Heinzl B, Sorantin E, Cvirn G, Gamillscheg A (2011) Tricuspid annular plane systolic excursion and right ventricular ejection fraction in pediatric and adolescent patients with tetralogy of Fallot, patients with atrial septal defect, and age-matched normal subjects. Clin Res Cardiol 100:67–75. https://doi.org/10.1007/s00392-010-0213-z
Arce OX, Knudson OA, Ellison MC, Baselga P, Ivy DD, DeGroff C, Valdes-Cruz L (2002) Longitudinal motion of the atrioventricular annuli in children: Reference values, growth related changes, and effects of right ventricular volume and pressure overload. J Am Soc Echocardiogr 15:906–916. https://doi.org/10.1067/mje.2002.121436
Roberts-Thomson KC, John B, Worthley SG, Brooks AG, Stiles MK, Lau DH, Kuklik P, Shipp NJ, Kalman JM, Sanders P (2009) Left atrial remodeling in patients with atrial septal defects. Hear Rhythm 6:1000–1006. https://doi.org/10.1016/j.hrthm.2009.03.050
Kim WH, Otsuji Y, Seward JB, Tei C (1999) Estimation of left ventricular function in right ventricular volume and pressure overload. Detection of early left ventricular dysfunction by Tei index. Jpn Heart J 40:145–154
Sillesen A-S, Pihl C, Raja AA, Davidsen AS, Lind LE, Dannesbo S, Navne J, Raja R, Vejlstrup N, Lange T, Bundgaard H, Iversen K (2019) Repeatability and reproducibility of neonatal echocardiography: the Copenhagen Baby Heart Study. J Am Soc Echocardiogr 32:895-905.e2. https://doi.org/10.1016/j.echo.2019.02.015
Breatnach CR, Levy PT, James AT, Franklin O, El-Khuffash A (2016) Novel echocardiography methods in the functional assessment of the newborn heart. Neonatology 110:248–260. https://doi.org/10.1159/000445779
Puchalski MD, Williams RV, Askovich B, Minich LLA, Mart C, Tani LY (2007) Assessment of right ventricular size and function: echo versus magnetic resonance imaging. Congenit Heart Dis 2:27–31. https://doi.org/10.1111/J.1747-0803.2007.00068.X
Udholm S, Rex C, Eckerström F, Onat M, Nyboe C, Hjortdal VE (2019) Small unrepaired atrial septal defects display impaired exercise capacity compared with healthy peers. Congenit Heart Dis 14:372–379. https://doi.org/10.1111/chd.12740
Udholm S, Nyboe C, Dantoft TM, Jørgensen T, Rask CU, Hjortdal VE (2019) Small atrial septal defects are associated with psychiatric diagnoses, emotional distress, and lower educational levels. Congenit Heart Dis 14:803–810. https://doi.org/10.1111/chd.12808
Udholm S, Nyboe C, Karunanithi Z, Christensen AI, Redington A, Nielsen-Kudsk JE, Hjortdal VE (2019) Lifelong burden of small unrepaired atrial septal defect: results from the Danish National Patient Registry. Int J Cardiol 283:101–106. https://doi.org/10.1016/j.ijcard.2019.02.024
Nyboe C, Karunanithi Z, Nielsen-Kudsk JE, Hjortdal VE (2018) Long-term mortality in patients with atrial septal defect: A nationwide cohort-study. Eur Heart J 39:993–998. https://doi.org/10.1093/eurheartj/ehx687
Acknowledgements
We thank all study participants of the CBHS. We also thank Søren Kaas for his valuable contribution to this CBHS study.
Funding
Open access funding provided by National Hospital. This work is supported by the Novo Nordic Foundation, the Danish Heart Association, the Danish Children’s Heart Foundation, Candy’s Foundation, the Toyota Foundation, the Herlev-Gentofte Hospital Research Foundation, and the Gangsted Foundation. The funders have no role in the design and conduct of the study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by AMD, SD, and LH. The first draft of the manuscript was written by AMD and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of Interest
HB receives lecture fees from Amgen, MSD, BMS, and Sanofi.
Ethics Approval
The CBHS complies with the 1964 Helsinki Declaration and its later amendments and was approved by the Danish Data Protection Agency (I-suite 04546, HGH-2016–53) and the Regional Ethics Committee (H-16001518).
Consent to Participate
Parents gave written-informed consent prior to inclusion in the study.
Consent to Publish.
All the authors transfer, assign, or otherwise convey all copyright ownership, including any and all rights exclusively to the journal, in the event that such work is published by the journal.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dehn, A.M., Dannesbo, S., Sellmer, A. et al. Atrial Septal Defect: Larger Right Ventricular Dimensions and Atrial Volumes as Early as in the First Month After Birth—a Case–Control Study Including 716 Neonates. Pediatr Cardiol 44, 1578–1586 (2023). https://doi.org/10.1007/s00246-023-03211-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-023-03211-z