
Abstract
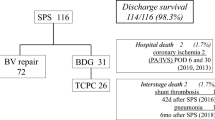
The study aimed to revisit the in-hospital predictors of shunt thrombosis (ST) in the foreground of the pulmonary artery size in patients who received modified Blalock–Taussig shunt (mBTS) as the first-stage palliation. Data from 80 patients who received mBTS as their initial palliative procedure between February 2012 and January 2017 was retrospectively collected. The median age and weight of the patients at the time of their mBTS procedure was 4 days (IQR 2–22 days) and 3.2 kg (IQR 2.8–3.7 kg), respectively. Of the 80 patients in the study, 11 (13.8%) developed ST. The diameter and corresponding z scores of the pulmonary arteries were significantly lower in patients with ST. The median shunt size/shunted pulmonary artery size (S/PA) ratio was considerably higher in patients with ST. In logistic regression analysis, pulmonary artery hypoplasia (PAH) [odds ratio (OR) = 13.7 (0.06–0.21), p < 0.001], S/PA ratio ≥ 0.9 [OR = 8.1 (0.03–0.53), p = 0.03], prematurity [OR = 9.5 (0.05–0.33), p = 0.003], and shunt size/weight (S/W) ratio ≥ 1.3 [OR = 6.4 (0.04–0.67), p = 0.012] were found to have a significant impact on ST. The best combination of sensitivity and specificity of the S/W (0.73 and 0.75) and the S/PA ratio (0.73 and 0.80) were achieved at the cut-off value of 1.3 and 0.9, respectively. The Youden index of S/PA was 0.52. While the area under the curve (AUC) of the S/W ratio was 0.686 ± 0.12 (p = 0.049), the AUC of the S/PA ratio was 0.791 ± 0.08 (p = 0.002). In conclusion, instead of weight, considering the size of the target pulmonary artery and thereby, the S/PA ratio would be more instructive in determining shunt size. There were a high number of patients in our study who showed PAH having received a shunt size based on their body weight. By contrast, our results showed that the S/PA ratio of ≥ 0.9 would be a good predictor of in-hospital ST.



Similar content being viewed by others

References
Bove T, Vandekerckhove K, Panzer J, De Groote K, De Wolf D, Francois K (2015) Disease-specific outcome analysis of palliation with the modified Blalock-Taussig shunt. World J Pediatr Congenit Heart Surg 6(1):67–74
Guzzetta NA, Foster GS, Mruthinti N, Kilgore PD, Miller BE, Kanter KR (2013) In-hospital shunt occlusion in infants undergoing a modified blalock-taussig shunt. Ann Thorac Surg 96(1):176–182
Myers JW, Ghanayem NS, Cao Y, Simpson P, Trapp K, Mitchell ME, Tweddell JS, Woods RK (2014) Outcomes of systemic to pulmonary artery shunts in patients weighing less than 3 kg: analysis of shunt type, size, and surgical approach. J Thorac Cardiovasc Surg 147(2):672–677
Shibata M, Itatani K, Oka N, Yoshii T, Nakamura Y, Kitamura T, Horai T, Miyaji K (2015) Optimal graft size of modified Blalock-Taussig shunt for biventricular circulation in neonates and small infants. Int Heart J 56(5):533–536
Jonas R (2014) Three-stage management of single ventricle. In: Jonas R (ed) Comprehensive surgical management of congenital heart disease, vol 1, 2nd edn. CRC Press, Florida, pp 479–515
Chittithavorn V, Duangpakdee P, Rergkliang C, Pruekprasert N (2017) Risk factors for in-hospital shunt thrombosis and mortality in patients weighing less than 3 kg with functionally univentricular heart undergoing a modified Blalock-Taussig shunt. Interact Cardiovasc Thorac Surg 25(3):407–413
Alsoufi B, Gillespie S, Mori M, Clabby M, Kanter K, Kogon B (2016) Factors affecting death and progression towards next stage following modified Blalock-Taussig shunt in neonates. Eur J Cardiothorac Surg 50(1):169–177
Dirks V, Pretre R, Knirsch W, Valsangiacomo Buechel ER, Seifert B, Schweiger M, Hubler M, Dave H (2013) Modified Blalock Taussig shunt: a not-so-simple palliative procedure. Eur J Cardiothorac Surg 44(6):1096–1102
Hobbes B, d’Udekem Y, Zannino D, Konstantinov IE, Brizard C, Brink J (2017) Determinants of adverse outcomes after systemic-to-pulmonary shunts in biventricular circulation. Ann Thorac Surg 104(4):1365–1370
Petrucci O, O’Brien SM, Jacobs ML, Jacobs JP, Manning PB, Eghtesady P (2011) Risk factors for mortality and morbidity after the neonatal Blalock-Taussig shunt procedure. Ann Thorac Surg 92(2):642–651
Pettersen MD, Du W, Skeens ME, Humes RA (2008) Regression equations for calculation of z scores of cardiac structures in a large cohort of healthy infants, children, and adolescents: an echocardiographic study. J Am Soc Echocardiogr 21(8):922–934
Vitanova K, Leopold C, Pabst von Ohain J, Wolf C, Beran E, Lange R, Cleuziou J (2018) Risk factors for failure of systemic-to-pulmonary artery shunts in biventricular circulation. Pediatr Cardiol. https://doi.org/10.1007/s00246-018-1898-4
Alkhulaifi AM, Lacour-Gayet F, Serraf A, Belli E, Planche C (2000) Systemic pulmonary shunts in neonates: early clinical outcome and choice of surgical approach. Ann Thorac Surg 69(5):1499–1504
Dorobantu DM, Pandey R, Sharabiani MT, Mahani AS, Angelini GD, Martin RP, Stoica SC (2016) Indications and results of systemic to pulmonary shunts: results from a national database. Eur J Cardiothorac Surg 49(6):1553–1563
McKenzie ED, Khan MS, Samayoa AX, Vener DS, Ishak YM, Santos AB, Heinle JS, Fraser CD Jr (2013) The Blalock-Taussig shunt revisited: a contemporary experience. J Am Coll Surg 216(4):699–704
Odim J, Portzky M, Zurakowski D, Wernovsky G, Burke RP, Mayer JE Jr, Castaneda AR, Jonas RA (1995) Sternotomy approach for the modified Blalock-Taussig shunt. Circulation 92(9 Suppl):II256–I261
Talwar S, Kumar MV, Muthukkumaran S, Airan B (2014) Is sternotomy superior to thoracotomy for modified Blalock-Taussig shunt? Interact Cardiovasc Thorac Surg 18(3):371–375
Kandakure PR, Dharmapuram AK, Ramadoss N, Babu V, Rao IM, Murthy KS (2010) Sternotomy approach for modified Blalock-Taussig shunt: is it a safe option? Asian Cardiovasc Thorac Ann 18(4):368–372
Acknowledgements
We would like to express our gratitude for the proof-read done by the Proof-Reading-Service.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Ethical Approval
The study was in accordance with the ethical standard of the institutional research committee and with the World Medical Association Declaration of Helsinki – Ethical Principles for Medical Research involving Human Subjects, adopted in 1964 and its later amendments; or with comparable ethical standards.
Additional information
The original version of this article was revised: The alignment error in Table 1 has been corrected.
Rights and permissions
About this article

Cite this article
Şişli, E., Tuncer, O.N., Şenkaya, S. et al. Blalock–Taussig Shunt Size: Should it be Based on Body Weight or Target Branch Pulmonary Artery Size?. Pediatr Cardiol 40, 38–44 (2019). https://doi.org/10.1007/s00246-018-1958-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-018-1958-9