
Abstract
Sildenafil, a phosphodiesterase-5 inhibitor, is a controversial treatment option for pulmonary arterial hypertension (PAH), a significant complication of bronchopulmonary dysplasia (BPD). The objective of this study was to evaluate the use of sildenafil in infants with PAH secondary to BPD. This was a retrospective review of medical records of all premature infants with PAH associated with BPD treated with sildenafil between January 2009 and May 2013 in a level 3 neonatal intensive care unit. The primary outcomes were clinical response (20 % decreases in respiratory support score or oxygen requirements) and echocardiographic response (20 % decrease in tricuspid regurgitation gradient or change of at least 1° of septal flattening). Twenty-three infants were included in the study. Significant echocardiographic and clinical responses were, respectively, observed in 71 and 35 % of cases. Most clinical responses were observed in the first 48 h of treatment, and the median time to an echocardiographic response was of 19 days. The median dose of sildenafil used was 4.4 mg/kg/day, with a median time to reach the maximum dose of 9 days. Transient hypotension was the primary reported side effect, and it was observed in 44 % of our study population. Sildenafil treatment in patients with PAH secondary to BPD was associated with an echocardiographic improvement in the majority of patients, whereas clinical improvement was observed in a minority of patients. Many infants presented with transient hypotension during the course of the treatment. Further prospective studies are required to better assess safety and efficacy of this treatment in this population.
Similar content being viewed by others

Introduction
Bronchopulmonary dysplasia (BPD) is a chronic lung disease that affects 33–46 % of extremely low birth weight (ELBW) infants [6]. Pulmonary arterial hypertension (PAH) may significantly complicate the course of BPD. Its prevalence is estimated to be approximately 17–25 % in infants with BPD [2, 12] and as high as 37 % in subgroups of infants with severe BPD [21]. Physiopathologic processes leading to the development of PAH are incompletely understood but include impairment in the normal structure, function, development and maturation of the respiratory tract and the pulmonary vascular circulation [23]. Survival rates of infants suffering from PAH complicating BPD are as low as 53 % at 2 years of age [10].
Pharmacological approaches to PAH treatment include sildenafil, a selective PDE-5 inhibitor. Sildenafil treatment has been studied in the context of persistent pulmonary hypertension of the newborn with remarkable improvement in oxygenation index and survival [4, 8, 11, 22, 24]. However, there are few data regarding its utilization in infants with PAH associated with BPD. Reported short-term effects of sildenafil in these infants include significant reduction in estimated pulmonary artery pressures without any noticeable changes in respiratory parameters [19]. In the long term, improvement in echocardiographic indices and good tolerability of the medication have been described [17].
In the absence of high-order empirical studies, sildenafil remains a controversial treatment option for the treatment of PAH in infants with BPD. To improve the available knowledge on this topic, we here describe our experience with the use of sildenafil in this population.
Materials and Methods
Study Design and Setting
We conducted a retrospective case series at CHU Sainte-Justine, Montreal, Canada. The institution’s Neonatal Intensive Care Unit (NICU) is a 65-bed level 3 unit that admits approximately 130 ELBW infants every year. This study was approved by the institutional review board.
Data Collection
All infants receiving oral sildenafil between January 2009 (date at which use of sildenafil commenced in the NICU) and May 2013 were identified from the institution’s pharmacy database. The population of interest was infants with PAH associated with BPD. Infants with diaphragmatic hernia, major cardiac malformations, postcapillary causes of pulmonary hypertension or who were transferred to another institution during their initial hospitalization were excluded from the study.
BPD was defined as requirement of supplemental oxygen at 36 weeks postmenstrual age [5]. The diagnosis of PAH was based on echocardiogram according to the presence of one or more of the following: tricuspid valve jet velocity more than or equal to 2.8 m/s in the absence of pulmonary stenosis [3], flat or left (type 2 or type 3) deviated interventricular septum when tricuspid regurgitation jet was absent, or bidirectional or right to left flow in a cardiac communication [18].
Medical records of selected infants were reviewed for data collection. Recorded infant characteristics included prenatal history, gestational age, sex, birth weight, postnatal complications, survival and age at discharge. Pharmacological data collected were: age of infant at initiation of sildenafil, sildenafil initial, maximum and median dosages, duration of treatment and reason for its cessation. The concomitant use of other PAH medications including inotropic support and steroids was noted. Side effects included worst degree of retinopathy of prematurity (ROP) before and during treatment with sildenafil, priapism and transient hypotension defined as a need to decrease sildenafil dose, skip a dose or cease treatment. Ventilator requirements (including invasive or non-invasive ventilation parameters and inspired fraction of oxygen (FiO2)) were collected 24 h before starting sildenafil, 48 h after introduction, at maximal dosage and a week after introduction. Respiratory severity scores (RSS) were calculated, when possible, using the mean FiO2 multiplied by the mean airway pressure. Echocardiographic data were recorded, when possible, at eight time points during the course of sildenafil treatment: time of sildenafil introduction, at maximum dosage, at 1, 2, 3 and 6 months after maximal dosing, at cessation of treatment and at follow-up after cessation of treatment.
During the study period, management of preterm infants in the NICU was in accordance with the current practices in our NICU. Supplemental oxygen was administered to maintain oxygen saturation between 85 and 92 % for premature infants until 36 weeks of corrected age and over 90 % after that age. There was no standard protocol for the detection, investigation and treatment of PAH in infants with BPD. All echocardiograms were realized by skilled technicians in cardiology and were reviewed and interpreted by pediatric cardiologists. For the purpose of the study, all echocardiograms were reviewed by a skilled cardiology technician. Decisions regarding the treatment of PAH were made in collaboration with the cardiology, neonatology and pharmacy teams.
The primary outcomes were clinical and echocardiographic improvement in PAH. Clinical improvement was defined as a 20 % decrease in the RSS or, when not possible to calculate, an absolute 20 % decrease in the FiO2 between serial respiratory evaluations. Echocardiographic improvement was defined as a 20 % decrease in the absolute tricuspid regurgitation gradient or, when not calculated, an improvement of 1° of septal flattening between serial echocardiograms. Secondary outcomes included median dosage of sildenafil, duration of treatment, safety assessment of treatment, survival rate and oxygen requirement at discharge.
Statistical Analysis
SPSS was used to analyze the data. Continuous descriptive variables were reported as medians with interquartile ranges for non-normally distributed data and as means with standard deviations for normally distributed data. Comparisons between initial and follow-up assessments were analyzed with the Student’s paired t test. The impact of corticosteroid treatment on clinical or echocardiographic responses during sildenafil treatment was assessed using Chi-square. Statistical significance was set at an alpha of <0.05.
Results
Thirty patients were initially identified from the pharmacy database during the study period. Seven infants in total were excluded: four due to major cardiac malformations, one did not suffer from BPD, one had a diaphragmatic hernia and one was transferred to another institution during the initial hospitalization. Twenty-three patients were included in the study. Their characteristics are presented in Table 1.
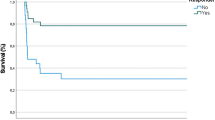
Infants were on mechanical ventilation for a median of 54 days (27). They received oxygen treatment for a median of 171 days (97) during hospitalization and a median of 228 days (262) in total including hospitalization and home oxygen. Fifteen infants (65 %) survived their initial hospitalization. One infant died of sepsis, while seven others died of terminal respiratory insufficiency and PAH. Patients’ median age at discharge was 9 weeks of corrected age (5) with a median hospital stay of 171 days (97). All but one of the survivors (93 %) were discharged with home oxygen therapy.
Clinical and echocardiographic responses are presented in Table 2. A clinical response was observed in 35 % of infants, with 75 % of them showing an effect in the first 48 h of treatment. An echocardiographic response was observed in 71 % of infants in whom echocardiographic data were complete. In two cases, the echocardiographic data were incomplete. In 76 % of the cases, the echocardiographic response was solely based on the change in degree of septal flattening. Eight patients received postnatal corticosteroids for pulmonary salvage during the first week of treatment with sildenafil. There was no correlation between a positive clinical (p = 0.60) or echocardiographic response (p = 0.63) and the use of systemic corticosteroids.
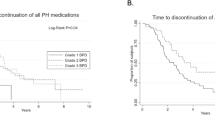
The pharmacological data of sildenafil citrate are presented in Table 3. Eight patients (53 % of survivors) were discharged with sildenafil. Twenty-one infants (91 %) received exogenous nitric oxide (NO) during their hospitalization. The median length of NO treatment alone and of concomitant use of NO and sildenafil was, respectively, 35 days (26) and 10 days (26). Bosentan was used alone in two infants with PAH (9 %) and in conjuncture with sildenafil in two cases (9 %). No patient received prostacyclin analogs.
Reasons for sildenafil cessation are presented in Table 4. The decision to discontinue sildenafil was based on the clinician’s judgment. No rebound PAH was noted after cessation of sildenafil. Regarding sildenafil’s safety profile, no life-threatening adverse event was noted. The main adverse effect that was observed was transient hypotension. It affected ten infants (43 %), but none of them required immediate intervention or inotropic support. Increase in oxygen requirement and hypotension was reported in one patient at introduction of sildenafil. No case of priapism was reported. The degree of ROP before and during sildenafil citrate treatment did not differ (p = 0.78).
Discussion
In our case series, we observed significant improvement in echocardiographic parameters in the majority of our patients (71 %) and a clinical response in a minority of them (35 %). Most (75 %) of the clinical responses were observed in the first 48 h of treatment, and the median time to observe an echocardiographic response was of 19 days. The median dose of sildenafil that was used was 4.4 mg/kg/day, with a median time to reach the maximum dose of 9 days. Transient hypotension was the main reported side effect, and it was observed in 44 % of our study population.
The discrepancy between echocardiographic and clinical response rates might be explained by several factors. Firstly, the RSS might not be the best predictor of clinical response. Ideally, an oxygenation index would be used to better assess clinical improvement in regard to pulmonary hypertension. However, in our population, arterial lines for blood gas are not available and repetitive arterial punctures are not indicated. Secondly, the vast majority of patients were receiving NO at the introduction of sildenafil. This may have attenuated the clinical effect of sildenafil and underestimated their clinical responses. Thirdly, time to reach maximal sildenafil dosage is long. It is possible that the time period when the clinical response was assessed overlapped with the period of increasing sildenafil dosage and underestimated the clinical response. It was decided to evaluate the clinical response in the first week of treatment to minimize the impact of possible spontaneous resolution of PAH with time. Fourthly, as it was hypothesized by Nyp et al. [19] in a comparable case series, the lower clinical response rate compared to the echocardiographic response could be related to ventilation perfusion mismatch present in the first days of treatment. This mismatch decreases with time. At last, time discrepancy between our clinical and echocardiographic responses could also be explained by our methodology. The echocardiographic data were only collected at introduction of treatment, when the maximum dose of sildenafil was reached and then monthly. Maybe we would have detected an earlier response to sildenafil citrate if we had collected echocardiographic data more frequently.
In this study, we relied on echocardiography for diagnosis and follow-up of PAH. Previous studies have shown that, compared to cardiac catheterization, echocardiography correctly diagnoses PAH in 79 % of cases, but correctly determines the severity of the PAH in only 47 % of cases [15]. We were aware that our echocardiographic data would provide us with estimations of PAH that may have poor correlation with direct measurements of catheterization. Cardiac catheterization would have been the gold standard but was not routinely performed since it is a very invasive and risky procedure. In this study, assessment of tricuspid regurgitation gradient was only possible in five infants and echocardiographic response was solely based on the change in the degree of septal flattening in 76 % of cases.
The median dose of sildenafil used in this study was 4.4 mg/kg/day. Even though the optimal posology of sildenafil in the neonatal population is still unknown, this dosage range seems to be in accordance with the current literature. In neonatal studies, oral sildenafil doses varied from 3.5 to 12 mg/kg/day [4, 8, 11, 24]. Pharmacokinetic studies suggested that an oral dose of 4.2 mg/kg/day of sildenafil could possibly be equivalent to the lowest recommended adult dose of 20 mg orally three times a day [1]. There was a high variability in the maximal dose, the number of days to achieve this dose and the duration of therapy. This can be explained by the lack of standardization in the management of patients with PAH associated with BPD in our center at the time of this study and the absence of guidelines in the literature.
There was a higher than expected rate of transient hypotension related to sildenafil in our population. Neonatal studies have shown conflicting data regarding the occurrence of systemic hypotension after oral or intravenous sildenafil. Most studies report a very low incidence of significant hypotension; however, patients were more likely to be on inotropic support [4, 11, 13, 22]. In our study, transient hypotension was reported in 43 % of infants but no life-threatening event occurred. The medication was stopped in two infants because of this side effect. In one patient, sildenafil was stopped early in the course of treatment because of systemic hypotension related to the drug. In the other one, the treatment was unsuccessfully introduced because of increase in oxygen requirement and hypotension. This event was possibly linked to ventilation perfusion mismatch.
Some concerns have been raised in the literature about sildenafil utilization and development or progression of ROP [14]. Further case-controlled studies in both term and preterm infants receiving sildenafil invalidated this association [7, 9]. No significant change in ROP before and after treatment with sildenafil was observed in our case series.
In a cohort of premature infants suffering from PAH and BPD, Khemani reported survival rates of 64 % at 6 months and of 53 % at 2 years after PAH diagnosis [10]. Similarly, 65 % of infants in our study survived from their initial hospitalization.
There are limitations to this study. First, this was a retrospective study of a small number of preterm infants. Second, it would have been interesting to compare our population to a control group of infants with PAH and BPD not treated with sildenafil. Since there was no systematic screening for PAH among BPD infants in our NICU, it was not possible to identify such a control group. Third, the fact that the majority of infants were receiving NO before introduction of sildenafil may have underestimated the effectiveness of the treatment. Fourth, our study cohort includes patients with severe respiratory disease, thus limiting the generalizability of this study. Fifth, our definition of systemic hypotension may have overestimated its incidence. Finally, 76 % of the echocardiographic responses were solely based on assessment of the degree of septal flattening. Other echocardiographic parameters to assess pulmonary artery pressure and right ventricular function could be evaluated in this patient population to improve PAH assessment. Appreciation of the pulmonary pressure is now also based on evaluation of systolic and diastolic function by tissue Doppler imaging, including systolic velocities on the lateral right ventricular wall, myocardial performance index measurement and tricuspid annular plane systolic excursion [20]. The left diastolic function could also be assessed since it is impaired in cases of PAH [16]. These studies are time-consuming and were not done systematically in this study population. We have since modified our monitoring protocol to target these patients and provide a complete echocardiographic study. The supplementary information will aid in better understanding the phenomenon of PAH and its impact on patients.
Conclusion
Sildenafil treatment in patients with PAH complicating BPD was associated with an echocardiographic improvement in the majority of patients, whereas clinical improvement was only observed in a minority of patients. Dosage used in our center seems to be in accordance with the current literature. Many infants presented with transient hypotension during the course of the treatment. Further prospective studies are required to better assess safety and efficacy of this treatment in this population.
References
Ahsman MJ, Witjes BC, Wildschut ED, Sluiter I, Vulto AG, Tibboel D, Mathot RA (2010) Sildenafil exposure in neonates with pulmonary hypertension after administration via a nasogastric tube. Arch Dis Child Fetal Neonatal Ed 95(2):F109–F114. doi:10.1136/adc.2009.168336
An HS, Bae EJ, Kim GB, Kwon BS, Beak JS, Kim EK, Kim HS, Choi JH, Noh CI, Yun YS (2010) Pulmonary hypertension in preterm infants with bronchopulmonary dysplasia. Korean Circ J 40(3):131–136. doi:10.4070/kcj.2010.40.3.131
Badesch DB, Champion HC, Sanchez MA, Hoeper MM, Loyd JE, Manes A, McGoon M, Naeije R, Olschewski H, Oudiz RJ, Torbicki A (2009) Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol 54(1 Suppl):S55–S66. doi:10.1016/j.jacc.2009.04.011
Baquero H, Soliz A, Neira F, Venegas ME, Sola A (2006) Oral sildenafil in infants with persistent pulmonary hypertension of the newborn: a pilot randomized blinded study. Pediatrics 117(4):1077–1083. doi:10.1542/peds.2005-0523
Ehrenkranz RA, Walsh MC, Vohr BR, Jobe AH, Wright LL, Fanaroff AA, Wrage LA, Poole K (2005) Validation of the national institutes of health consensus definition of bronchopulmonary dysplasia. Pediatrics 116(6):1353–1360. doi:10.1542/peds.2005-0249
Fanaroff AA, Stoll BJ, Wright LL, Carlo WA, Ehrenkranz RA, Stark AR, Bauer CR, Donovan EF, Korones SB, Laptook AR, Lemons JA, Oh W, Papile LA, Shankaran S, Stevenson DK, Tyson JE, Poole WK (2007) Trends in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet Gynecol 196(2):147. doi:10.1016/j.ajog.2006.09.014 e141–148
Fang AY, Guy KJ, Konig K (2013) The effect of sildenafil on retinopathy of prematurity in very preterm infants. J Perinatol 33(3):218–221. doi:10.1038/jp.2012.84
Herrera TR, Concha GP, Holberto CJ, Loera GR, Rodríguez BI (2006) Oral sildenafil as an alternative treatment in the persistent pulmonary hypertension in newborns. Rev Mex Pediatr 74(4):159–163
Kehat R, Bonsall DJ, North R, Connors B (2010) Ocular findings of oral sildenafil use in term and near-term neonates. J AAPOS 14(2):159–162. doi:10.1016/j.jaapos.2009.12.161
Khemani E, McElhinney DB, Rhein L, Andrade O, Lacro RV, Thomas KC, Mullen MP (2007) Pulmonary artery hypertension in formerly premature infants with bronchopulmonary dysplasia: clinical features and outcomes in the surfactant era. Pediatrics 120(6):1260–1269. doi:10.1542/peds.2007-0971
Khorana M, Yookaseam T, Layangool T, Kanjanapattanakul W, Paradeevisut H (2011) Outcome of oral sildenafil therapy on persistent pulmonary hypertension of the newborn at Queen Sirikit National Institute of Child Health. J Med Assoc Thai 94(Suppl 3):64–73
Kim DH, Kim HS, Choi CW, Kim EK, Kim BI, Choi JH (2012) Risk factors for pulmonary artery hypertension in preterm infants with moderate or severe bronchopulmonary dysplasia. Neonatology 101(1):40–46. doi:10.1159/000327891
Limjoco J, Paquette L, Ramanathan R, Seri I, Friedlich P (2013) Changes in mean arterial blood pressure during sildenafil use in neonates with meconium aspiration syndrome or sepsis. Am J Ther. doi:10.1097/MJT.0b013e31826fc4ec
Marsh CS, Marden B, Newsom R (2004) Severe retinopathy of prematurity (ROP) in a premature baby treated with sildenafil acetate (Viagra) for pulmonary hypertension. Br J Ophthalmol 88(2):306–307
Mourani PM, Sontag MK, Younoszai A, Ivy DD, Abman SH (2008) Clinical utility of echocardiography for the diagnosis and management of pulmonary vascular disease in young children with chronic lung disease. Pediatrics 121(2):317–325. doi:10.1542/peds.2007-1583
Mourani PM, Ivy DD, Rosenberg AA, Fagan TE, Abman SH (2008) Left ventricular diastolic dysfunction in bronchopulmonary dysplasia. J Pediatr 152(2):291–293. doi:10.1016/j.jpeds.2007.11.006
Mourani PM, Sontag MK, Ivy DD, Abman SH (2009) Effects of long-term sildenafil treatment for pulmonary hypertension in infants with chronic lung disease. J Pediatr 154(3):379–384. doi:10.1016/j.jpeds.2008.09.021 e371–372
Mourani PM, Sontag MK, Younoszai A, Miller JI, Kinsella JP, Baker CD, Poindexter BB, Ingram DA, Abman SH (2015) Early pulmonary vascular disease in preterm infants at risk for bronchopulmonary dysplasia. Am J Respir Crit Care Med 191(1):87–95. doi:10.1164/rccm.201409-1594OC
Nyp M, Sandritter T, Poppinga N, Simon C, Truog WE (2012) Sildenafil citrate, bronchopulmonary dysplasia and disordered pulmonary gas exchange: any benefits? J Perinatol Off J Calif Perinat Assoc 32(1):64–69. doi:10.1038/jp.2011.131
Patel N, Mills JF, Cheung MM (2009) Assessment of right ventricular function using tissue Doppler imaging in infants with pulmonary hypertension. Neonatology 96(3):193–199. discussion 200-192. doi:10.1159/000215585
Slaughter JL, Pakrashi T, Jones DE, South AP, Shah TA (2011) Echocardiographic detection of pulmonary hypertension in extremely low birth weight infants with bronchopulmonary dysplasia requiring prolonged positive pressure ventilation. J Perinatol 31(10):635–640. doi:10.1038/jp.2010.213
Steinhorn RH, Kinsella JP, Pierce C, Butrous G, Dilleen M, Oakes M, Wessel DL (2009) Intravenous sildenafil in the treatment of neonates with persistent pulmonary hypertension. J Pediatr 155(6):841–847. doi:10.1016/j.jpeds.2009.06.012 e841
Stenmark KR, Abman SH (2005) Lung vascular development: implications for the pathogenesis of bronchopulmonary dysplasia. Annu Rev Physiol 67:623–661. doi:10.1146/annurev.physiol.67.040403.102229
Vargas-Origel A, Gomez-Rodriguez G, Aldana-Valenzuela C, Vela-Huerta MM, Alarcon-Santos SB, Amador-Licona N (2010) The use of sildenafil in persistent pulmonary hypertension of the newborn. Am J Perinatol 27(3):225–230. doi:10.1055/s-0029-1239496
Acknowledgments
We thank Johanne Therien and Vivianne Therrien for technical support.
Conflict of interest
The authors do not have any conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Trottier-Boucher, M.N., Lapointe, A., Malo, J. et al. Sildenafil for the Treatment of Pulmonary Arterial Hypertension in Infants with Bronchopulmonary Dysplasia. Pediatr Cardiol 36, 1255–1260 (2015). https://doi.org/10.1007/s00246-015-1154-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-015-1154-0