
Abstract
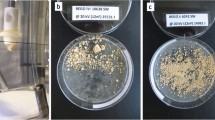
Extracorporeal shock wave lithotripsy (SWL) is less invasive compared to the other invasive modalities of stone treatment that are gaining popularity. Hence, methods to improve the efficacy of SWL are desirable. We studied the effectiveness of dual frequency on the efficacy of stone fragmentation, but minimizing treatment time. A phantom 10 mm spherical BegoStone was fragmented in vitro in a kidney model using an electromagnetic lithotripter (Storz MODULITH®SLX-F2). A total of 78 stones were fragmented each with 3000 shocks at 60 Hz or 120 Hz or a dual frequency (DF) of 60–120 Hz. For the DF setting, the first 1000 shocks were delivered at 60 Hz and the next 2000 at 120 Hz. Total weight and number of significant fragments of > 3 mm (TWSF and TNSF, respectively) and also > 2 mm was measured. Results: The mean TWSF was 0.1, 0.16, and 0.08 g for 60 Hz, 120 Hz, and DF 60–120 Hz, respectively. The TWSF of DF 60–120 Hz was significantly lower than that of 120 Hz (p = 0.02), but same as the 60 Hz (p = 0.32). The mean TNSF of > 3 mm was 2.6, 3.0, and 2.0 for 60 Hz, 120 Hz, and DF 60–120 Hz, respectively, without significant differences between each setting. However, increasing trend of TWSF, TW2 mm and TN2 mm was seen in the order of DF, 60 Hz and 120 Hz (p = 0.019, p = 0.004 and 0.017, respectively). Treatment time for 60 Hz, 120 Hz, and DF 60–120 Hz was 50, 25, and 34 min, respectively. Dual-frequency setting produced effective stone fragmentation compared to the recommended 60 Hz, while decreasing treatment time. DF variation is one other factor that may be tailored for effective stone comminution and needs clinical evaluation.


Similar content being viewed by others


References
Chaussy C, Schuller J, Schmiedt E et al (1984) Extracorporeal shock-wave lithotripsy (ESWL) for treatment of urolithiasis. Urology 23(5):59–66
Assimos D, Krambeck A, Miller NL et al (2016) Surgical management of stones: american urological association/endourological society guideline, part II. J Urol 196(4):1161–1169
Chaussy CG, Tiselius HG (2018) How can and should we optimize extracorporeal shock wave lithotripsy? Invited review. Urolithiasis 46:2–17
Paterson RF, Lifshitz DA, Lingeman JE et al (2002) Stone fragmentation during shock wave lithotripsy is improved by slowing the shock wave rate: studies with a new animal model. J Urol 168(5):2211–2215
Semins MJ, Trock BJ, Matlaga BR (2008) The effect of shock wave rate on the outcome of shock wave lithotripsy: a meta-analysis. J Urol 179(1):194–197
Li K, Lin T, Zhang C et al (2013) Optimal frequency of shock wave lithotripsy in urolithiasis treatment: a systematic review and meta-analysis of randomized controlled trials. J Urol 190(4):1260–1267
Delius M, Ueberle F, Eisenmenger W (1998) Extracorporeal shock waves act by shock wave-gas bubble interaction. Ultrasound Med Biol 24(7):1055–1059
Liu Y, Zhong P (2002) BegoStone-a new stone phantom for shock wave lithotripsy researchx. J Acoust Soc Am 112(4):1265–1268
Demirci D, Sofikerim M, Yalçin E et al (2007) Comparison of conventional and step-wise shockwave lithotripsy in management of urinary calculi. J Endourol 21:1407–1410
Honey RJ, Ray AA, Ghiculete D et al (2010) Shock wave lithotripsy: a randomized, double-blind trial to compare immediate versus delayed voltage escalation. Urology 75:38–43
Lambert EH, Walsh R, Moreno MW et al (2010) Effect of escalating versus fixed voltage treatment on stone comminution and renal injury during extracorporeal shock wave lithotripsy: a prospective randomized trial. J Urol 183:580–584
Madbouly K, El-Tiraifi AM, Seida M et al (2005) Slow versus fast shock wave lithotripsy rate for urolithiasis: a prospective randomized study. J Urol 173(1):27–130
Ng CF, Lo AK, Lee KW et al (2012) A prospective, randomized study of the clinical effects of shock wave delivery for unilateral kidney stones: 60 versus 120 shocks per minute. J Urol 188(3):837–842
Davenport K, Minervini A, Keoghane S et al (2006) Does rate matter? The results of a randomized controlled trial of 60 versus 120 shocks per minute for shock wave lithotripsy of renal calculi. J Urol 176(5):2055–2058
Yilmaz E, Batislam E, Basar M et al (2005) Optimal frequency in extracorporeal shock wave lithotripsy: prospective randomized study. Urology 66(6):1160–1164
Salem HK, Fathy H, Elfayoumy H et al (2014) Slow vs. rapid delivery rate shock wave lithotripsy for pediatric renal urolithiasis: a prospective randomized study. J Urol 191(5):1370–1374
Nguyen DP, Hnilicka S, Kiss B et al (2015) Optimization of extracorporeal shock wave lithotripsy delivery rates achieves excellent outcomes for ureteral stones: results of a prospective randomized trial. J Urol 194(2):418–423
Anglada-Curado FJ, Campos-Hernandez P, Carrasco-Valiente J et al (2013) Extracorporeal shock wave lithotripsy for distal ureteral calculi: improved efficacy using low frequency. Int J Urol 20(2):214–219
Zhu S, Cocks FH, Preminger GM et al (2002) The role of stress waves and cavitation in stone comminution in shock wave lithotripsy. Ultrasound Med Biol 28(5):661–671
Funding
Midwest Stone Institute, St. Louis, MO.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Han, C.S., Vetter, J.M., Endicott, R. et al. Dual-frequency setting for urinary stone fragmentation during shock wave lithotripsy: an in vitro study . Urolithiasis 48, 369–375 (2020). https://doi.org/10.1007/s00240-019-01162-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-019-01162-w