
Abstract
Purpose
Limited sampling strategy (LSS) is a precise and relatively convenient therapeutic drug monitoring method. We evaluated LSSs for mycophenolic acid (MPA) in children with nephrotic syndrome treated with mycophenolic mofetil (MMF) and validated the LSSs using two different approaches.
Methods
We measured MPA plasma concentrations in 31 children using HPLC-UV method and received 37 MPA pharmacokinetic profiles (0–12 h). For six children, MPA profiles were estimated twice after two MMF doses. LSSs were developed using multilinear regression with STATISTICA and R software and validated using validation group and bootstrap method, respectively.
Results
The best three time point equations included C1, C3, C6 (good guess 83%, bias − 2.78%; 95% confidence interval (CI) − 9.85–0.46); C1, C2, C6 (good guess 72%, bias 0.72%; 95% CI − 5.33–7.69); and C1, C2, C4 (good guess 72%, bias 2.05%; 95% CI − 4.92–13.01) for STATISTICA software. For R software, the best equations consisted of C1, C3, C6 (good guess 92%, bias − 2.69%; 95% CI − 27.18–33.75); C0, C1, C3 (good guess 84%, bias − 2.11%; 95% CI − 24.19–22.29); and C0, C1, C2 (good guess 84%, bias − 0.48%; 95% CI − 30.77–54.07). During validation, better results were obtained for R evaluations, i.e., bootstrap method.
Conclusions
The most useful equations included C0, C1, C3 and C0, C1, C2 time points; however, the most precise included C1, C3, C6 time points because of MPA enterohepatic recirculation. Better results were obtained for bootstrap validation due to greater number of patients. Validated LSS should be used only in the population for which it was developed. As there is growing evidence that underexposure of MPA is associated with insufficient treatment response, we recommend the introduction of therapeutic drug monitoring for MPA in children with nephrotic syndrome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Nephrotic syndrome, more frequently diagnosed in children, forms a group of clinical symptoms with the proteinuria [1, 2]. Children with nephrotic syndrome are vulnerable to suffer from many ailments, which may lead to cardiovascular disease, chronic kidney insufficiency, or even to the necessity of renal transplantation [1, 3]. The treatment of nephrotic syndrome is based on steroids and immunosuppressants [1, 4]; however, long-term steroid therapy unfavorably influences children’s development and their further lives [2, 5]. The immunosuppressants most frequently administered are cyclosporine (CsA), chlorambucil, and cyclophosphamide, which cause severe side effects, e.g., hematological, gonadal, and nephrological toxicities [4]. The aim of the treatment is to minimalize the incidence of proteinuria recurrence; however, in some patients, trace proteinuria may be observed, defined as protein concentration < 10 mg/kg body weight/day, which is rather related to the chronic kidney disease than nephrotic syndrome [6].
Mycophenolate mofetil (MMF), an immunosuppressive drug, is efficient in nephrotic syndrome and does not cause nephrotoxicity and additionally is well tolerated by patients [1, 4]. MMF is a pro-drug with an active moiety—mycophenolic acid (MPA). MPA is safe and effective when plasma concentrations are above the target minimum exposure. However, the necessity of monitoring MPA concentration is still a matter of debate. MPA pharmacokinetics is complex and differs between groups of patients what causes difficulties in reaching the target concentrations values. Monitoring MPA C0 would be easy and convenient; however, numerous studies showed that MPA C0 poorly correlated with the relapse rate [7]. MPA area under the time–concentration curve from 0 to 12 h (AUC0–12) tends to be a more useful tool in therapeutic drug monitoring (TDM). Still measuring total AUC0–12 is expensive, time-consuming, and inconvenient for patients, especially for children. Moreover, no specific MPA AUC0–12 target was established for children with nephrotic syndrome [8].
Limited sampling strategy (LSS) is a useful approach to assess drug pharmacokinetics and safety. Collecting only few blood samples to establish AUC0–12 is an easier than determining full pharmacokinetic profile. It is more convenient for patients and facilitates the work of nursing staff. There are studies concerning MPA LSS; however, most of them included renal transplant recipients, whereas each LSS should be evaluated and used in the same patient’s group [9, 10]. Separate LSS should be evaluated for renal or heart transplant recipients and patients suffering from lupus nephritis or nephrotic syndrome. While there are two main possible calculation methods for evaluating LSS, multiple linear regression (MLR) [11,12,13,14,15,16,17] and Bayesian approach [18, 19], there are many software solutions [18, 20, 21]. In this study, we evaluated LSS for children with nephrotic syndrome using two methods of calculation, STATISTICA and R software, and two different methods of validation, validation group and bootstrap method, respectively. We hypothesized that the results obtained using two approaches should be comparable.
Material and methods
Study population
The retrospective study included 31 children (13 males and 18 females) with nephrotic syndrome, aged 3–18 years (mean age, 11 years). MMF was administered orally twice a day at the same dose (250–1000 mg) for at least 1 month prior to the pharmacokinetic study. Patients were hospitalized between 2012 and 2015 in Department of Pediatric Cardiology, Nephrology, and Hypertension, University of Medical Sciences in Poznan, Poland. The flow diagram of the patient selection is presented in Fig. 1. For children, demographical data as well as biochemical parameters were recorded.

The flow diagram of patient selection. The division into test and validation groups concerns only STATISTICA evaluations. For R evaluations, bootstrap procedure was used. The profiles were randomly divided into test group and validation group, and the procedure was performed 100 times. *Only for STATISTICA evaluations
The blood samples were collected into EDTA tubes before MMF administration (C0) and subsequently 1 h (C1), 2 h (C2), 3 h (C3), 4 h (C4), 6 h (C6), 9 h (C9) and 12 h (C12) after its administration. MMF was administrated in 12-h intervals at least for a month before blood collection for pharmacokinetic analysis; therefore, we assumed that all children were in steady state. In 12 children, blood samples were collected up to 6 h; therefore, as they were in steady state, it was assumed that C12 was equal to C0 [11]. Additionally, we observed that MPA C0 and C12 were comparable (2.78 ± 1.81 μg/mL and 2.07 ± 0.95 μg/mL for C0 and C12, respectively, p = 0.055, n = 25) for those children who had both samples collected. In six children, MPA pharmacokinetic profiles were determined twice after two MMF doses.
Children receiving CsA or MMF at not equal morning and evening doses or shorter than 1 month as well as children with too low number of blood samples collected were excluded from the study.
Four children included in the study received concomitantly steroids and seven children had trace proteinuria (< 10 mg/body weight/day) observed during blood sample collection. These two factors may be the source of potential bias.
Almost all children (n = 35) received enalapril and were supplemented with vitamins A and E (n = 30) as well as alfacalcidol (n = 18). Few children received additional antihypertensive drugs (losartanum, amlodipinum; n = 7).
All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Bioethical Committee at Poznan University of Medical Sciences. Informed consent was obtained from the parents or guardians prior to initiating the study.
Analytical methods
MPA plasma concentrations were determined using HPLC-UV method. The analytical method for MPA determination was described elsewhere [22, 23]. MPA AUC0–12 was calculated using linear trapezoidal rule and the maximal concentration (Cmax) was extracted from the determined concentrations. To compare the data, we normalized MPA AUC0–12 to the most frequently administered dose which was 500 mg b.i.d. All calculations were performed using MS Excel 2010 (Microsoft Corporation, Redmond, WA, USA).
LSSs evaluation
For evaluations, two groups with different blood sampling were considered separately. In the first group of children (C9 group), 25 profiles with the following blood samples C0, C1, C2, C3, C4, C6, C9, and C12 were included, and in the second group of children (C6 group), 37 profiles without C9 were included. The six children with MPA profiles determined twice were included in the C6 group, and the second profile for each child comprised the validation group. The demographic data were not compared statistically as group C6 comprises all patients from group C6, and both groups seemed to be very similar. The characteristics are presented in Table 1.
LSSs were evaluated using STATISTICA 13.0 software (StatSoft, Inc., Tulsa, OK, USA) and R software (R Core Team, 2013). For each measured concentration, calculated AUC0–12 and Cmax normal distributions were confirmed using Shapiro–Wilk test (STATISTICA) and Kolmogorov–Smirnov test (R). For both evaluations method, MLR was applied to develop LSSs. The MPA AUC0–12 was considered as the dependent variable, while MPA plasma concentrations at each sampling time point were the independent variables. All concentration–time profiles were completed; therefore, no estimation was done. There were no missing data to handle except for missing C12 in 12 children, which was previously described (C12 was assumed to equal C0). The equations were evaluated as follows: AUCpred = A + B × Cx + C × Cy + D × Cz, where AUCpred indicated predicted AUC; A indicated the intercept; Cx, Cy, Cz indicated the concentration for three different time points; and B, C, D indicated the coefficients for Cx, Cy, Cz, respectively.
For STATISTICA evaluations, children were divided into two groups, test group (13 and 19 MPA profiles for C9 and C6 group, respectively) and validation group (12 and 18 MPA profiles for C9 and C6 group, respectively). For test group, the correlations between MPA plasma concentrations at single time points and AUC0–12 were firstly verified. Secondly, the equations were developed using stepwise regression with backward elimination. Finally, the number of possible equations based on samples collected during the first 3 h after drug administration was calculated according to the formula:
where k is the number of k-combinations (for equations with up to three time points) and n is the number of elements in the set (C0, C1, C2, C3; 4 elements). Subsequently, each of the possible 14 combinations was introduced manually into the software. Each developed equation was used for calculating AUCpred for children in the validation group.
For R evaluations, it was assumed that the model should include up to three time points. For C6 and C9 groups, the profiles were randomly divided into two groups (test group and validation group). This procedure was performed 100 times to obtain the most varied and random test and validation groups (bootstrap procedure). Based on the results from test groups, all possible models were assessed. For each model, AUCpred were calculated using coefficients which were medians from the previously calculated 100 coefficients. AUCpred were calculated for all profiles because all profiles were previously used for building models.
For both evaluation methods, we calculated the values of r2, adjusted r2, good guess, and root square mean error (RMSE) for each equation to analyze the agreement between AUCpred and AUCcalc. Good guess was determined by the number of profiles for AUCpred within AUC0–12 ± 15%. The bias and precision for predicting AUC0–12 was assessed based on mean prediction error (%MPE) and mean absolute error (%MAE), respectively. The accepted values for %MPE and %MAE were ± 15% and ± 10%, respectively [24]. The best model was chosen on the base of good guess, r2, and adjusted r2.
Results
Pharmacokinetic parameters
For all children included in the study, MPA concentrations from 0 to 12 h and AUC0–12 are presented in Table 1. MPA AUC0–12 was within 9.31 μg h/mL and 95.88 μg h/mL for C9 group and within 7.19 μg h/mL and 94.54 μg h/mL for C6 group. MPA AUC0–12 below 10 μg h/mL was observed in three children receiving MMF dose of 250 mg b.i.d. The dose-normalized MPA AUC0–12 was within 18.62 μg h/mL and 92.95 μg h/mL for C9 group and within 12.65 μg h/mL and 131.56 μg h/mL for C6 group. Mean MPA AUC0–12 was lower in children with proteinuria (43.80 ± 33.26 μg h/mL vs. 50.30 ± 18.53 μg h/mL for children with and without proteinuria, respectively); however, the difference was not significant. Only one child with proteinuria had MPA AUC0–12 below 10 μg h/mL. This child may have received too low MMF dose or may have not response to MMF. For six children with MPA AUC0–12 above 10 μg h/mL, proteinuria may have been related to the chronic kidney disease with tissue proteinuria without the nephrotic syndrome and concomitant edema and coagulant disorders.
LSSs equations
The best equations for both evaluations methods are presented in Tables 2 and 3. Some of the other LSSs are included in Tables A.1 and B.1 (Appendices A and B).
For evaluations with STATISTICA software 53 and 48 equations in total, consisting of one up to seven concentration time points were obtained for C9 and C6 groups, respectively. For evaluations with R software, each model composed of one, two, or three time points and 92 models and 63 models were obtained in total for C9 group and C6 group, respectively.
For STATISTICA calculations, firstly, the equations included more than three time points. In total for both groups (C6 and C9), there were one equation with six time points, four with five time points, and four with four time points (Tables 2 and 3; Table A.1). The best r2, adjusted r2, and good guess (94%) were for the equation including C0, C1, C3, C4, C6 for C6 group. The appropriate good guess (89%), r2, and adjusted r2 (> 0.900) were obtained for four time point equation (C0, C1, C3, C6) for C6 group. The equation with six time points (C0, C1, C3, C4, C9, C12) should be precise; however, its good guess amounted to only 58%.
For the C9 group and equations with three time points, three best equations included C1, C2, C3; C1, C3, C6; and C0, C1, C4 for STATISTICA software; however, the good guess values were rather poor for these equations (67%, 58%, 50%, respectively; Table 2). For R software, three best equations consisted of C1, C3, C6; C0, C1, C3; and C0, C1, C2. Good guess was > 80% for five best equations evaluated with R, whereas for STATISTICA evaluations, the highest good guest amounted to 67%. The values of r2 and adjusted r2 for R evaluations were > 0.800 for two best equations and for one equation (C1, C4, C9) with good guess 72%. The values of r2 and good guess were better for the equations evaluated with R software, whereas %MAE was lower for STATISTICA evaluations (Table 2; Table A.1). In Fig. 2, we compared the correlations between AUCpred and AUCcalc for the best equation (C1, C3, C6) estimated with STATISTICA and R in C9 group.

The correlations between AUCpred derived from C1, C3, C6, and AUCcalc from 0 to 12 h MPA pharmacokinetic profile in C9 group. The equations including C1, C3, and C6 were evaluated with STATISTICA (closed diamonds; dotted line) and R (open squares; solid line). The equations were 9.34 + 1.49∙C1 + 3.51∙C3 + 2.74∙C6 for STATISTICA and 7.10 + 1.21∙C1 + 3.75∙C3 + 3.08∙C6 for R
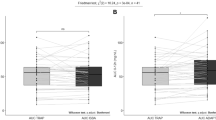
For C6 group and STATISTICA, the best three time point equations included C1, C3, C6 (with the best good guess, i.e., 83%); C1, C2, C6; and C1, C2, C4. For R software, three best equations included C1, C3, C6 (with the best good guess, i.e., 89%); C1, C2, C6; and C0, C1, C3. For STATISTICA evaluations, two equations with three time-points were characterized by r2 and adjusted r2 > 0.800 with good guess 83% and 72%. For R evaluations, good guess for seven equations was > 80%. The values of r2 and adjusted r2 were > 0.900 for four equations. For the C6 group, the values of r2, adjusted r2, and good guess were also better for the evaluations with R software; however, the differences were smaller than within C9 group for some equations as well as %MPE, %MAE, and median error were lower for STATISTICA evaluations (Table 3). In Fig. 3, we compared the correlations between AUCpred and AUCcalc for the best equation (C1, C3, C6) estimated with STATISTICA and R in C6 group.

The correlations between AUCpred derived from C1, C3, C6, and AUCcalc from 0 to 12 h MPA pharmacokinetic profile in C6 group. The equations including C1, C3, and C6 were evaluated with STATISTICA (closed diamonds; dotted line) and R (open squares; solid line). The equations were 2.55 + 1.28∙C1 + 2.98∙C3 + 4.76∙C6 for STATISTICA and 3.59 + 1.25∙C1 + 3.06∙C3 + 4.65∙C6 for R
The best equations with two time points included C1, C6 for both groups and STATISTICA calculations, whereas for R calculations, C1, C3 and C1, C6 were the best for C9 and C6 groups, respectively. The good guess values were better for the R results (Tables 2 and 3).
For one time point equation, the highest good guess was 72% (C1) for R evaluations and 58% (C6) for STATISTICA for C9 group (Table 2; Table A.1). For C6 group, the best good guess was 68% (C1) and 50% (C1) for R and STATISTICA, respectively (data not shown). In C9 group, the one time point equation with C0 was characterized by the good guess of 72% for R calculations but only of 17% for STATISTICA (data not shown). For C6 group, the good guess for C0 equations amounted to 62% for R and 28% for STATISTICA (data not shown).
Among the best 47 equations presented in Tables 2 and 3, about 41% (14/47) included C0.
Discussion
The MPA pharmacokinetic parameters are highly variable, and there are numerous factors which may contribute to this variability, e.g., treatment duration, therapeutic indication, drugs co-administered, genetic, physiologic, and environmental factors, as well as kidney or liver dysfunction [8]. For TDM, MPA AUC0–12 is the most useful parameter; however, obtaining full pharmacokinetic profile is time-consuming and inconvenient for patients, especially for children [25], and there is still a need to establish target values for children with nephrotic syndrome [8]. In our previous study [22], we suggested that for those children, MPA AUC0–12 > 60 μg h/mL may be considered efficient to avoid proteinuria recurrence and ensure the safe and effective treatment. Moreover, we did not observe any toxicity in those children. Other studies showed that MPA AUC0–12 above 30 μg h/mL is recommended for children with nephrotic syndrome [26] or described fewer relapses in children with MPA AUC0–12 above 45 μg h/mL [8]. However, there are some cases where MMF is ineffective when standard doses are administered. The recent study of Kirpalani et al. [27] described the increase in MPA apparent clearance which may indicate that the unresponsiveness of MMF may be due to MPA underexposure. Therefore, it seems important to find if the reason why children do not respond to MMF is dose-related (infra or over dosing) and if so correct the dose before changing the treatment to other drugs with severe adverse effects (such as CsA or cyclophosphamide) in these children. The evaluation of MPA LSS should facilitate assessing treatment efficacy in pediatric patients.
There are two main approaches to evaluate LSS, Bayesian estimation and MLR, which can be performed using several software programs. NONMEM, a nonlinear mixed-effect modeling tool, is the gold standard for population pharmacokinetic analysis. However, working with this program is difficult because NONMEM is written in Fortran language [20, 21]. Therefore, we decided to evaluate and compare the LSSs using other software, STATISTICA and R. Both programs rely on MLR as computation methods. R software comprises powerful statistical techniques, supports object-oriented programming, and its accessible free of charge [20]. The STATISTICA line of software consists of a fully integrated line of analytic solutions which are easy to handle and offer wide options of algorithms, functions, and tests as well as effective graphic visualization.
To our knowledge, in the literature, there are only a few studies concerning LSS as the approach for monitoring MPA therapy in children and adults with nephrotic syndrome. In none of the studies, MLR method was applied for evaluations. Saint-Marcoux et al. [18] and Zhao et al. [19] evaluated LSS for children with nephrotic syndrome basing on Bayesian estimator method. Some LSS for MMF treated patients evaluated using MLR concerned pediatric patients after renal [10,11,12, 28] or liver [15, 29] transplantation as well as adults patients after renal [13, 14, 16], lung [30], heart [9, 31], and liver [15] transplantation. The equations from these studies are shown in Table 4.
We assumed that it would be the most convenient procedure for patients if the LSS evaluated includes up to three time points. Therefore, the equations with four to six time points, generated with STATISTICA, although characterized by the best good guess (up to 94%) will not be useful in clinical practice. The most convenient approach for patients would be collecting only one or two blood samples; however, in our study, the results obtained for these equations were not satisfactory comparing with the three time point equations.
The best three time point equations in our study included C1, C3, C6; C1, C2, C6; and C1, C2, C4 for evaluations with STATISTICA software and C1, C3, C6; C1, C2, C6; C0, C1, C2; and C0, C1, C3 for evaluations with R software. The same time points were included in the best equation for R calculations for both (C6 and C9) groups. The literature data with LSS for pediatric patients included C20 min, C60 min, C180 min [18], or C0, C1, C4 [19]; however, these LSS were evaluated based on Bayesian estimator. Among MLR equations found in the literature, not only none of them included C1, C2, C3 and C1, C3, C6 time points, but also none of them considered children with nephrotic syndrome. Therefore, we suggest that LSS should be validated and used only in the population for which it was developed. It is in accordance with our previous data [22] as we concluded that MPA pharmacokinetic parameters must be calculated and applied separately for patients after renal transplantation and with nephrotic syndrome. The differences may derive from the MPA pharmacokinetic intra- and intervariability.
Apart from including three time points, the most useful equations should also contain time points collected up to 3 h after drug administration because most of the children are not hospitalized but treated in clinics. Therefore, although C1, C3, C6 comprised the best equation, collecting C0, C1, C3 or C0, C1, C2 should be more practical. However, this approach in the case of MPA may lead to misprediction of AUC0–12 due to MPA enterohepatic recirculation and the occurrence of MPA second Cmax. According to the literature, the most accurate LSS should probably include at least one blood sample collected at time point close to second Cmax of MPA due to MPA enterohepatic recirculation [32].
In our study, only a few equations included C0 which is in accordance with the literature data as MPA C0 did not predict the response to the drug sufficiently [9].
In general, the results obtained using STATISTICA and R were different and better for R. Apart from two best three time point equations for C6 group which are the same, the subsequent equations differ. The best equation for C9 group for STATISTICA (C1, C2, C3) is the sixth for R calculations. The second best equation for STATISTICA (C1, C3, C6) is the best for R. Better values of r2, adjusted r2, and good guess were obtained for LSS generated with R program. The difference may be explained by different validations for both computing methods. At the same time, %MPE and %MAE were lower for STATISTICA results. The difference is smaller for C6 group as this group was more numerous. The greater number of patients contributed to the better results for STATISTICA in C6 group than C9 group. We assumed that test group and validation group should be more numerous to achieve better results with STATISTICA.
The limitation of our study is the fact that we were unable to collect the samples more frequently, especially within the first 2 h after MMF administration. More studies on the larger number of pediatric patients are needed to confirm our observations. Other limitations are the inclusion of only Caucasian children, children receiving steroids, and children with trace proteinuria during the day of blood collection. These factors may influence MPA exposure and limit the generalizability of the study.
Conclusion
The best equations in our study included C1, C3, C6; C0, C1, C3; and C0, C1, C2. The most useful in everyday practice equations include C0, C1, C3 and C0, C1, C2; however, the most precise is the equation including C1, C3, C6 time points. Better results were obtained with R software.
For validation method, the number of patients is essential; therefore, better results were obtained with R calculations and the bootstrap validation as validation groups for STATISTICA calculations were smaller.
The proposed equations may be an useful implement for MPA monitoring in children with nephrotic syndrome treated with MMF as there is growing evidence that underexposure of MPA is associated with insufficient treatment response. Still, it is important to remember that properly validated LSS should be used only in the population for which it was developed.
References
Ostalska-Nowicka D, Malinska A, Silska M, Perek B, Zachwieja J, Nowicki M (2011) Mycophenolate mofetil (MMF) treatment efficacy in children with primary and secondary glomerulonephritis. Arch Med Sci AMS 7:1042–1048. https://doi.org/10.5114/aoms.2011.26618
Guha P, De A, Ghosal M (2009) Behavior profile of children with nephrotic syndrome. Indian J Psychiatry 51:122–126. https://doi.org/10.4103/0019-5545.49452
Cadnapaphornchai MA, Tkachenko O, Shchekochikhin D, Schrier RW (2014) The nephrotic syndrome: pathogenesis and treatment of edema formation and secondary complications. Pediatr Nephrol 29:1159–1167. https://doi.org/10.1007/s00467-013-2567-8
Lombel RM, Gipson DS, Hodson EM (2013) Treatment of steroid-sensitive nephrotic syndrome: new guidelines from KDIGO. Pediatr Nephrol 28:415–426. https://doi.org/10.1007/s00467-012-2310-x
Tönshoff B, Höcker B, Weber LT (2005) Steroid withdrawal in pediatric and adult renal transplant recipients. Pediatr Nephrol 20:409–417. https://doi.org/10.1007/s00467-004-1765-9
Noone DG, Iijima K, Parekh R (2018) Idiopathic nephrotic syndrome in children. Lancet 392:61–74. https://doi.org/10.1016/S0140-6736(18)30536-1
Hackl Á, Cseprekál O, Gessner M, Liebau MC, Habbig S, Ehren R, Müller C, Taylan C, Dötsch J, Weber LT (2016) Mycophenolate mofetil therapy in children with idiopathic nephrotic syndrome: does therapeutic drug monitoring make a difference? Ther Drug Monit 38:274–279. https://doi.org/10.1097/FTD.0000000000000258
Tellier S, Dallocchio A, Guigonis V, Saint-Marcoux F, Llanas B, Ichay L, Bandin F, Godron A, Morin D, Brochard K, Gandia P, Bouchet S, Marquet P, Decramer S, Harambat J (2016) Mycophenolic acid pharmacokinetics and relapse in children with steroid–dependent idiopathic nephrotic syndrome. Clin J Am Soc Nephrol 11:1777–1782. https://doi.org/10.2215/CJN.00320116
Pawinski T, Kunicki PK, Sobieszczanska-Malek M, Gralak B, Szlaska I (2009) A limited sampling strategy for estimating mycophenolic acid area under the curve in adult heart transplant patients treated with concomitant cyclosporine. J Clin Pharm Ther 34:89–101. https://doi.org/10.1111/j.1365-2710.2008.00973.x
Weber LT, Hoecker B, Armstrong VW, Oellerich M, Tönshoff B (2006) Validation of an abbreviated pharmacokinetic profile for the estimation of mycophenolic acid exposure in pediatric renal transplant recipients. Ther Drug Monit 28:623–631. https://doi.org/10.1097/01.ftd.0000246766.12872.12
David-Neto E, Araujo LMP, Sumita NM et al (2003) Mycophenolic acid pharmacokinetics in stable pediatric renal transplantation. Pediatr Nephrol 18:266–272. https://doi.org/10.1007/s00467-002-1057-1
Filler G (2004) Abbreviated mycophenolic acid AUC from CO, C1, C2, and C4 is preferable in children after renal transplantation on mycophenolate mofetil and tacrolimus therapy. Transpl Int 17:120–125. https://doi.org/10.1111/j.1432-2277.2004.tb00415.x
Teshima D, Maiguma T, Kaji H, Otsubo K, Kitagawa N, Okabe Y, Sugitani A, Tanaka M, Oishi R (2008) Estimation of the area under the curve for mycophenolic acid in adult renal transplant patients with concomitant tacrolimus using a limited sampling strategy. J Clin Pharm Ther 33:159–163. https://doi.org/10.1111/j.1365-2710.2008.00896.x
Cai W, Ye C, Sun X, Qin K, Qin Y, Zhao D, Wu F, Hu Y, Li H, Tan L (2015) Limited sampling strategy for predicting area under the concentration–time curve for mycophenolic acid in Chinese adults receiving mycophenolate mofetil and tacrolimus early after renal transplantation. Ther Drug Monit 37:304–310. https://doi.org/10.1097/FTD.0000000000000165
Zicheng Y, Weixia Z, Hao C, Hongzhuan C (2007) Limited sampling strategy for the estimation of mycophenolic acid area under the plasma concentration-time curve in adult patients undergoing liver transplant. Ther Drug Monit 29:207–214. https://doi.org/10.1097/FTD.0b013e318040ce0b
Cai W, Cai Q, Xiong N, Qin Y, Lai L, Sun X, Hu Y (2018) Limited sampling strategy for estimating mycophenolic acid exposure on day 7 post-transplant for two mycophenolate mofetil formulations derived from 20 Chinese renal transplant recipients. Transplant Proc 50:1298–1304. https://doi.org/10.1016/j.transproceed.2018.02.068
Brooks EK, Tett SE, Isbel NM, McWhinney B, Staatz CE (2018) Evaluation of multiple linear regression–based limited sampling strategies for enteric-coated mycophenolate sodium in adult kidney transplant recipients. Ther Drug Monit 40:195–201. https://doi.org/10.1097/FTD.0000000000000486
Saint-Marcoux F, Guigonis V, Decramer S, Gandia P, Ranchin B, Parant F, Bessenay L, Libert F, Harambat J, Bouchet S, Broux F, Compagnon P, Marquet P (2011) Development of a Bayesian estimator for the therapeutic drug monitoring of mycophenolate mofetil in children with idiopathic nephrotic syndrome. Pharmacol Res 63:423–431. https://doi.org/10.1016/j.phrs.2011.01.009
Zhao W, Elie V, Baudouin V, Bensman A, André JL, Brochard K, Broux F, Cailliez M, Loirat C, Jacqz-Aigrain E (2010) Population pharmacokinetics and Bayesian estimator of mycophenolic acid in children with idiopathic nephrotic syndrome. Br J Clin Pharmacol 69:358–366. https://doi.org/10.1111/j.1365-2125.2010.03615.x
Li J, Yan K, Hou L, du X, Zhu P, Zheng L, Zhu C (2017) An algorithm and R program for fitting and simulation of pharmacokinetic and pharmacodynamic data. Eur J Drug Metab Pharmacokinet 42:499–518. https://doi.org/10.1007/s13318-016-0358-x
Pradhan S, Song B, Lee J, Chae JW, Kim KI, Back HM, Han N, Kwon KI, Yun HY (2017) Performance comparison of first-order conditional estimation with interaction and Bayesian estimation methods for estimating the population parameters and its distribution from data sets with a low number of subjects. BMC Med Res Methodol 17:154. https://doi.org/10.1186/s12874-017-0427-0
Sobiak J, Resztak M, Ostalska-Nowicka D, Zachwieja J, Gąsiorowska K, Piechanowska W, Chrzanowska M (2015) Monitoring of mycophenolate mofetil metabolites in children with nephrotic syndrome and the proposed novel target values of pharmacokinetic parameters. Eur J Pharm Sci 77:189–196. https://doi.org/10.1016/j.ejps.2015.06.017
Elbarbry FA, Shoker AS (2007) Liquid chromatographic determination of mycophenolic acid and its metabolites in human kidney transplant plasma: pharmacokinetic application. J Chromatogr B 859:276–281. https://doi.org/10.1016/j.jchromb.2007.09.036
van der MAF, Marcus MAE, Touw DJ et al (2011) Optimal sampling strategy development methodology using maximum a posteriori Bayesian estimation. Ther Drug Monit 33:133–146. https://doi.org/10.1097/FTD.0b013e31820f40f8
Martial LC, Jacobs BAW, Cornelissen EAM, de Haan AFJ, Koch BCP, Burger DM, Aarnoutse RE, Schreuder MF, Brüggemann RJM (2016) Pharmacokinetics and target attainment of mycophenolate in pediatric renal transplant patients. Pediatr Transplant 20:492–499. https://doi.org/10.1111/petr.12695
Tong K, Mao J, Fu H, Shen H, Liu A, Shu Q, du L (2016) The value of monitoring the serum concentration of mycophenolate mofetil in children with steroid-dependent/frequent relapsing nephrotic syndrome. Nephron 132:327–334. https://doi.org/10.1159/000445070
Kirpalani A, Rothfels L, Sharma AP, Cuellar CR, Filler G (2019) Nephrotic state substantially enhances apparent mycophenolic acid clearance. Clin Nephrol 91:162–171. https://doi.org/10.5414/CN109583
Filler G, Feber J, Lepage N, Weiler G, Mai I (2002) Universal approach to pharmacokinetic monitoring of immunosuppressive agents in children. Pediatr Transplant 6:411–418. https://doi.org/10.1034/j.1399-3046.2002.02039.x
Attard TM, Dhawan A, Tredger JM et al (2008) Mycophenolic acid metabolite levels in pediatric liver transplantation: correlation with a limited sampling strategy. J Appl Res 8:135–142
Ting LSL, Partovi N, Levy RD, Riggs KW, Ensom MHH (2006) Limited sampling strategy for predicting area under the concentration-time curve of mycophenolic acid in adult lung transplant recipients. Pharmacother J Hum Pharmacol Drug Ther 26:1232–1240. https://doi.org/10.1592/phco.26.9.1232
Baraldo M, Isola M, Feruglio MT, Francesconi A, Franceschi L, Tursi V, Livi U, Furlanut M (2005) Therapeutic mycophenolic acid monitoring by means of limited sampling strategy in orthotopic heart transplant patients. Transplant Proc 37:2240–2243. https://doi.org/10.1016/j.transproceed.2005.03.090
Staatz CE, Tett SE (2007) Clinical pharmacokinetics and pharmacodynamics of mycophenolate in solid organ transplant recipients. Clin Pharmacokinet 46:13–58. https://doi.org/10.2165/00003088-200746010-00002
Acknowledgments
The authors would like to acknowledge the nursing staff that participated in the sample collection.
Authors’ individual contributions
JS, TP, DO-N, and MC designed the study; JS, MR, DO-N, and JZ collected the data; JS and MR carried out the quantifications of analytes in blood; JS, TP, and PŻ carried out the statistical analyses; JS, TP, and MC analyzed data; and JS and TP wrote the first draft of the manuscript. All authors contributed to, and have approved, the final manuscript.
Funding
This study was financially supported by Poznan University of Medical Sciences, Poland (grant number 502-14-03306413-10156).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the Bioethical Committee at Poznan University of Medical Sciences.
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
Informed consent to participate was obtained from all parents or guardians of individual participants included in the study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Sobiak, J., Resztak, M., Pawiński, T. et al. Limited sampling strategy to predict mycophenolic acid area under the curve in pediatric patients with nephrotic syndrome: a retrospective cohort study. Eur J Clin Pharmacol 75, 1249–1259 (2019). https://doi.org/10.1007/s00228-019-02701-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-019-02701-5