
Abstract
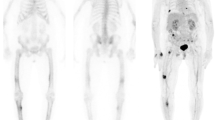
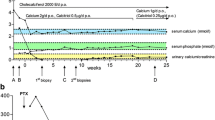
Bone lytic lesions are a possible complication of pseudohypoparathyroidism type 1B, in undertreated adult patients. Whole body [18F] F-fluorocholine PET/CT is a useful imaging tool to assess brown tumor progression in this context. We describe the case of a 33-year-old woman, referred for the diagnostic evaluation of lytic bone lesions of the lower limbs, in the context of asymptomatic pseudohypoparathyroidism. She had been treated with alfacalcidol and calcium during her childhood. Treatment was discontinued at the age of 18 years old because of the lack of symptoms. A femur biopsy revealed a lesion rich in giant cells, without malignancy, consistent with a brown tumor. Laboratory tests showed a parathyroid level at 1387 pg/ml (14–50). Whole-body Fluorocholine PET/CT revealed hypermetabolism of bone lesions. The final diagnosis was brown tumors related to hyperparathyroidism complicating an untreated pseudohypoparathyroidism. Genetic testing confirmed PHP type 1B. Pseudohypoparathyroidism with radiographic evidence of hyperparathyroid bone disease, is a very rare condition due to parathyroid hormone resistance in target organs, i.e., kidney resistance, but with conserved bone cell sensitivity. It has been reported in only a few cases of pseudohypoparathyroidism type Ib. Long-term vitamin D treatment was required to correct bone hyperparathyroidism. With this rationale, the patient was treated with calcium, alfacalcidol, and cholecalciferol. One-year follow-up showed complete resolution of pain, improvement in serum calcium, and regression of bone lesions on [18F]F-fluorocholine PET/CT. This case illustrates the usefulness of [18F]F-fluorocholine PET/CT for the imaging of brown tumors in pseudohypoparathyroidism type 1B, and emphasizes the importance of calcium and vitamin D treatment in adult patients, to avoid the deleterious effects of high parathyroid hormone on skeletal integrity.

Similar content being viewed by others

Data availability
The data that support the findings of this manuscript are available within the paper and from the corresponding author upon reasonable request.
References
Mantovani G (2011) Clinical review: pseudohypoparathyroidism: diagnosis and treatment. J Clin Endocrinol Metab 96:3020–3030. https://doi.org/10.1210/jc.2011-1048
Eubanks PJ, Stabile BE (1998) Osteitis fibrosa cystica with renal parathyroid hormone resistance: a review of pseudohypoparathyroidism with insight into calcium homeostasis. Arch Surg 133:673–676. https://doi.org/10.1001/archsurg.133.6.673
Albright F, Burnett CH, Smith PH, Parson W (1942) Pseudo-hypoparathyroidism-example of “Seabright-Bantam syndrome”; report of three cases. Endocrinology 30:922–932
Tashjian AH Jr, Frantz AG, Lee JB (1966) Pseudohypoparathyroidism: assays of parathyroid hormone and thyrocalcitonin. Proc Natl Acad Sci U S A56:1138–1142. https://doi.org/10.1073/pnas.56.4.1138
Mann JB, Alterman S, Hills AG (1962) Albright’s hereditary osteodystrophy comprising pseudohypoparathyroidism and pseudo-pseudohypoparathyroidism. With a report of two cases representing the complete syndrome occurring in successive generations. Ann Intern Med 56:315–342. https://doi.org/10.7326/0003-4819-56-2-315
Kidd GS, Schaaf M, Adler RA, Lassman MN, Wray HL (1980) Skeletal responsiveness in pseudohypoparathyroidism. A spectrum of clinical disease. Am J Med 68:772–781. https://doi.org/10.1016/0002-9343(80)90270-3
Jacquet-Francillon N, Prevot N (2023) Brown tumors in nuclear medicine: a systematic review. Ann Nucl Med. https://doi.org/10.1007/s12149-023-01832-1
Costello JM, Dent CE (1963) hypo-hyperparathyroidism. ArchDis Child 38:397–407. https://doi.org/10.1136/adc.38.200.397
Nusynowitz ML, Frame B, Kolb FO (1976 Mar) The spectrum of the hypoparathyroid states: A classification based on physiologic principles. Medicine (Baltimore). 55(2):105–119. https://doi.org/10.1097/00005792-197603000-00001
Kolb FO, Steinbach HL (1962) Pseudohypoparathyroidism with secondary hyperparathyroidism and osteitis fibrosa. J Clin Endocrinol Metab 22:59–70. https://doi.org/10.1210/jcem-22-1-59
Ramnitz MS, Gourh P, Goldbach-Mansky R, Wodajo F, Ichikawa S, Econs MJ, White KE et al (2016) Phenotypic and genotypic characterization and treatment of a cohort with familial tumoral calcinosis/hyperostosis-hyperphosphatemia syndrome. J Bone Miner Res 31:1845–1854. https://doi.org/10.1002/jbmr.2870
Frame B, Hanson CA, Frost HM, Block M, Arnstein AR (1972) Renal resistance to parathyroid hormone with osteitis fibrosa: "pseudohypohyperparathyroidism". Am J Med 52:311–321. https://doi.org/10.1016/0002-9343(72)90018-6
Neary NM, El-Maouche D, Hopkins R, Libutti SK, Moses AM, Weinstein LS (2012) Development and treatment of tertiary hyperparathyroidism in patients with pseudohypoparathyroidism type 1B. J Clin Endocrinol Metab 97:3025–3030. https://doi.org/10.1210/jc.2012-1655
Sinha TK, DeLuca HF, Bell NH (1977) Evidence for a defect in the formation of 1alpha,25-dihydroxyvitamin D in pseudohypoparathyroidism. Metabolism 26:731–738. https://doi.org/10.1016/0026-0495(77)90060-9
Bell NH, Khairi MRA, Johnston CC Jr et al (1978) Effects of 1. 25-dihvdroxvvitamin D on calcium metabolism and quantitative bone histology in pseudohypoparathyroidism. In: Talmage RV CDH (ed) Endocrinology of calcium metabolism: proceedings of the sixth parathyroid conference. Vancouver, Canada, Amsterdam, Excerpta Medica, pp 33–38
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gonnelli, S., Briot, K., Cormier, C. et al. Multiple brown tumors: a bone complication due to long-term untreated pseudohypoparathyroidism. Osteoporos Int 35, 195–199 (2024). https://doi.org/10.1007/s00198-023-06878-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-023-06878-5