
Abstract
Summary
This study reviews publications to describe the signs, symptoms and impact of tumour-induced osteomalacia (TIO) on patients’ burden of disease. TIO is associated with a spectrum of signs and symptoms imposing a significant clinical burden, but the psychosocial impact of this rare disease has been poorly researched so far.
Introduction
To describe the signs, symptoms and impacts of tumour-induced osteomalacia (TIO) and summarise the state of research on the burden of disease of this ultra-rare condition.
Methods
A targeted literature review was conducted in PubMed using pre-defined search terms. Relevant articles published between 1980 and 2021 were screened for inclusion. Seventy records were selected for analysis. Data were extracted and grouped into categories and sub-categories to identify recurrent signs, symptoms and impacts of TIO and describe the burden on patients. Chord diagrams were created to analyse the relationships between different TIO outcomes and characterise the presentation of TIO.
Results
Although the number of articles on TIO published have been increasing over the past 20 years, most studies were case reports and case series (n = 65/70) and only few were studies with higher quality of evidence (n = 5/70). Most articles were based on data reported by clinicians (n = 67/70). Patients with TIO experienced a combination of outcomes including chronic pain, weakness, skeletal-related manifestations and limitations in mobility. Only a few studies (n = 2/70) analysed the burden of TIO on the emotional wellbeing and on the work life of the patient.
Conclusion
Patients with TIO present with a spectrum of signs and symptoms that impose a significant burden. The impact on the psychosocial wellbeing of patients should be further investigated, as this has been poorly researched so far. Studies with high quality of evidence should be designed to further the understanding of the burden of disease of TIO from the patient’s perspective.
Similar content being viewed by others

Introduction
Tumour-induced osteomalacia (TIO) is an ultra-rare, acquired paraneoplastic syndrome caused by high blood levels of fibroblast growth factor 23 (FGF23), a phosphate- and vitamin D-regulating hormone [1]. FGF23 is secreted by small, slowly growing tumours that are usually benign [2]. An excess of FGF23 causes hypophosphatemia, resulting from decreased renal tubular phosphate reabsorption, with a low or inappropriate level of active vitamin D [3]. As initial signs and symptoms can be non-specific and may go unrecognised, patients often present a long history of undiagnosed fractures, musculoskeletal pain, fatigue and severe myopathy [4].
Reporting of new TIO cases in the literature has increased in the past decade. Still, the overall numbers are very low: to date, approximately 1000 cases have been reported in the medical literature [5]. The only formal epidemiology study in TIO is an observational cohort study using national Danish health registries for 2008–2018 that found the incidence of TIO to be 0.13 per 100,000 and the prevalence no more than 0.70 per 100,000 people per year for the total population of the country [6].
The established treatment for TIO is the complete surgical resection of the causative tumour, which should be curative [7]. Evidence shows that FGF23 levels return to normal in most cases after surgeries, and the clinical complaints of TIO are alleviated [3]. However, in 35 to 40% of TIO patients, the pathogenic tumours cannot be localised or completely resected [7]. In these cases, treatment to increase blood phosphate is required, traditionally consisting of daily administration of oral phosphate and active vitamin D [3]. However, this treatment over the long term is not optimal, with side effects of daily treatment including frequent gastrointestinal distress, hypercalcemia, nephrocalcinosis and tertiary hyperparathyroidism [7]. In 2020, the US Food and Drug Administration (FDA) granted approval to burosumab, a fully human, monoclonal antibody to FGF23, for the treatment of patients with tumour-induced osteomalacia (TIO) associated with phosphaturic mesenchymal tumours that cannot be curatively resected or localised in adult and paediatric patients 2 years of age and older [8, 9]. Burosumab blocks excess FGF23, normalising phosphate metabolism and improving bone health. The results of two single-arm Phase II studies (NCT02304367, NCT02722798) investigating the safety and efficacy of burosumab in adults with non-resectable/non-localisable TIO have shown that the treatment restores phosphate homeostasis and improves osteomalacia, resulting in significant improvements in health-related quality of life (QoL) in patients with TIO [7, 10].
The rarity of TIO and its initial unspecific symptoms and the challenges in the localisation of the causative tumour can determine long delays in diagnosis, leading to potentially irreversible physical consequences. This has a significant impact on the QoL of people living with TIO [4].
Because of the rarity of this disease and the need to educate physicians in its clinical management, published literature reviews have tended to focus on the prevalence, diagnosis and treatment of TIO [11,12,13]. Limited research has been published that explores and describes the physical and psychosocial burden of this condition on patients and their carers/families [4].
This study is a review of publications identified through a targeted literature review to describe the burden of disease for people living with TIO and assess the state of research on the impact of TIO on patients’ QoL.
Methods
A targeted literature review was conducted in PubMed using pre-defined search terms designed to capture the available information on the signs, symptoms and impacts associated with TIO and the resultant burden of disease (Appendix). To capture additional sources of evidence, other publications were identified through the reference lists or citations of the identified literature (snowballing).
Selection of eligible publications
Two members of the research team screened the titles and abstracts of the articles captured in the searches for potential relevance. Articles were selected for full-text screening if they included at least one of the disease terms and at least one of the terms relating to disease burden. Only articles published between 1 January 1980 and 31 May 2021 regarding humans were eligible for inclusion. No country, language or study type restrictions were applied.
Data extraction
Data retrieved from the full text of the included articles were extracted into a Microsoft Excel workbook. Information on the publication, including source of information, year and country of publication, authors, title, study design, sample size and key demographics, was extracted. Data on the history of clinical manifestation and burden of TIO were also obtained. These included relevant disease characteristics prior to and after initial presentation as well as the impact of TIO on activities of daily living, work life and emotional wellbeing.
In the first part of the analysis, disease characteristics and impacts were grouped into categories and sub-categories using Excel to identify the frequency of recurrent signs, symptoms and impacts of TIO and describe the burden of the disease on patients reported in each of the publications. In the second part of the analysis, publications on single case reports were further investigated. The occurrence of co-reported signs and symptoms of TIO were analysed to better understand and characterise TIO’s clinical presentation. Chord diagrams were created to visualise the number of patients with co-occurring reports of TIO signs, symptoms and impacts using the software for data visualisation Flourish [14].
Assessment of evidence quality
We acknowledge the concerns about weak inferences and the high likelihood of biases associated with case reports and case series reports, which formed the vast majority of publications available for the purpose of this study (n = 65/70), and which constitute low-quality evidence [15]. Only one clinical trial, which constitutes high-quality evidence [16], was eligible for this review.
Results
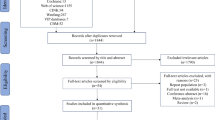
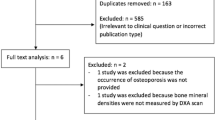
Figure 1 shows the PRISMA diagram for the selection of the eligible publications. Through the literature search on PubMed, 180 articles were identified, and 44 additional articles were captured through snowballing. After titles and abstracts were reviewed, 85 articles were selected for full-text screening. Ten were excluded because the full text was not accessible and 5 because they did not meet the inclusion criteria or were not stand-alone studies (e.g., literature reviews). A total of 70 records were included in this review.

Overview of the article selection process. aNo additional articles were identified via other databases. bArticles were excluded if their abstract and/or title did not include at least one of the disease terms AND at least one of the terms relating to disease burden. cReasons for exclusion = not appropriate after reviewing full text (n = 5); could not access article (n = 10)
Of the 70 articles included, 65 were clinical case reports and case report series (Appendix), 3 were retrospective reviews of patient medical records [13, 17, 18], 1 was a clinical trial [10] and 1 was a cross-sectional study [4]. Fifty-eight studies focussed on single patients’ cases, while 12 reviewed multiple ones (range 2–144 patients). The articles were published across a range of countries worldwide, including Japan (n = 15), the USA (n = 13), China (n = 9), Germany (n = 4), India (n = 4), Italy (n = 3) and the UK (n = 3), and they were all written in English. The majority of articles were published in the last 20 years, with one-third published in the last 10 years (Fig. 2).

Overview of number of articles included by year of publication. Figure generated using Flourish (Kiln Enterprises Ltd)
All included studies, with the exception of two, were based on data reported by the treating clinician. Only two of the articles contained data obtained directly from the patient: one using patient-reported outcome measures (PROMs) and one reporting data from a patient interview. Most studies (n = 66/70) retrieved their data from medical records. Only 3 studies reported data as measured by specific patient- or clinician-reported outcome measures: the Brief Pain Inventory (BPI); the Visual Analogue Scale (VAS) pain score; the Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-Fatigue); the 36-item Short Form (SF-36) survey scale for QoL and the Brief Pain Inventory–Short Form (BPI-sf).
TIO signs, symptoms and impacts
The TIO signs and symptoms described in the literature were classified in 2 overarching categories: clinical manifestations and symptoms. The impacts of TIO impacts on different QoL domains were grouped into the following categories: physical health, work life and emotional wellbeing. The pie chart in Fig. 3 shows how many times each TIO sign, symptom and impact was mentioned in the analysed literature.

Count of times each TIO outcome was reported in the literature. Figure generated using Flourish (Kiln Enterprises Ltd)
Clinical manifestations (signs)
Clinical manifestations refer to all signs of disease detected through clinical examinations. Skeletal deficits were the most frequently reported manifestations (n = 48 times). These included TIO-related fractures and pseudo-fractures, height loss and joint swelling. The muscle deficits reported were atrophy and muscle wasting (n = 4 times). Other manifestations described were nasal obstructions (n = 5 times), weight loss (n = 3 times) and visual disturbances (n = 1 times).
Symptoms
Symptoms refer to all features indicating a disease condition that are reported by the patient and that cannot be objectively detected or diagnosed through clinical tests or examination. Pain was the most reported TIO symptom (n = 124 times). It was described as generalised or localised pain in bones or joints. Other frequently reported symptoms were weakness (n = 38 times) and fatigue (n = 21 times). Stiffness (n = 5 times), spasm (n = 1 times) and body heaviness (n = 1 time) were also mentioned.
Impact of TIO on physical health
Physical impact refers to any physical consequence of the signs and symptoms of TIO experienced by patients. This included impairments of mobility (n = 28 times) and movement agility (n = 11 times), even leading to the requirement for mobility aids (n = 21 times). The mobility-related impacts described in the literature were affected gait, difficulty walking and difficulty climbing stairs. Impairment of movement agility included an array of outcomes related to an inability or limited ability to perform certain movements, such as standing, rising from a squatting position or lifting objects. Also, groups under this category were experiencing a fall and being bedridden.
Impact of TIO on work life and emotional wellbeing
Work impact refers to any consequence of TIO on a patient’s work life. The only TIO outcome on this domain of the QoL described in this review was the necessity to stop working (n = 4 times). Other consequences of TIO were categorised under emotional impact. This refers to the impact of the disease on patients’ mental wellbeing (n = 4 times), including the experience of anxiety, depression and suicide attempts.
TIO case reports
Sixty-five of the 70 articles eligible for this review were case reports and case series reports. The authors found a substantial disagreement in the literature with regard to including different study designs in literature reviews [19]. Some articles recommend against the combination of different study designs in the same analysis to avoid the risk of misleading results [19]. Given that the large majority of articles included in this analysis were case reports, the authors agreed to focus the second part of the analysis only on the case reports and case series reports. Given that the overall burden in terms of signs and symptoms had been outlined in the first part of the analysis, as a second step, case reports were further examined to try to identify potential patterns in the presentation and co-presentation of signs, symptoms and impacts of TIO (cluster analysis). Some articles described cases from multiple patients, with cases being separately analysed (n = 4/65). A total of 70 individual cases were identified to be included in this analysis. Table 1 shows the demographics of the TIO patients described in this case study analysis.
In the case reports, almost all patients described experiencing some form of generalised or localised pain associated with their TIO (n = 64/70). Several respondents also reported experiencing weakness (n = 38/70) and skeletal-related manifestations (n = 30/70). The majority of patients also reported physical impacts as outcomes of TIO, including impacts on mobility (n = 26/70), the use of mobility aids (n = 20/70) and detriments in movement agility (n = 15/70). Similarly, to the data retrieved from all the articles included in this literature review, only a few patient reports described work-life and emotional impacts. Three patients reported stopping working permanently or temporarily due to physical disabilities caused by TIO. Two patients described suffering severe impacts on their mental wellbeing after the disease onset, with one who reported anxiety and depression and one who reported a suicide attempt that was attributed to the unbearable pain caused by TIO (Table 2).
Co-presentation of signs, symptoms and impacts
Patients with TIO reported a combination of signs, symptoms and impacts of TIO. The chord diagram in Fig. 4 shows the one-to-one relationship between the 4 outcomes that were reported by the greatest number of patients, namely pain, weakness, skeletal-related manifestations and affected mobility. The 4 outcomes are arranged around a circle and are connected to one another through arcs. The size of each arc is proportional to the number of patients who reported the co-presentation of two outcomes. The diagram shows that pain and weakness were the symptoms that were co-reported by the highest number of patients (n = 35/70), followed by pain and skeletal-related manifestations (n = 27/70), and pain and affected mobility (n = 24/70). One-to-one relationship between the other outcomes was less frequent.

Co-presentation patterns of 2 TIO outcomes in case reports. Note that the sum of the co-presentation patterns does not reflect the overall number of patients reporting each outcome, as the same patient might have reported more than one co-presentation pattern. Figure generated using Flourish (Kiln Enterprises Ltd)
Figure 5 further examines the number of patients who reported a combination of 3 TIO outcomes. More specifically, the diagrams show how many patients reported the co-presentation of pain and weakness, and pain and skeletal-related manifestations with impaired movement agility and affected mobility. Overall, the number of patients describing these combinations of 3 TIO outcomes was low (range 9–14/70). The greatest number of patients reported the co-presentation of pain, weakness and skeletal-related manifestations (n = 17/70).

Co-presentation patterns of pain and weakness and pain and skeletal-related manifestations with another TIO outcome. Note that the sum of the co-presentation patterns does not reflect the overall number of patients reporting each outcome, as the same patient might have reported more than one co-presentation pattern. Figure generated using Flourish (Kiln Enterprises Ltd)
Discussion
The aim of this study was to describe the clinical manifestations of TIO and their impact on the burden of disease for people living with TIO as reported in the available literature on this condition.
The majority of the articles were published in the past 20 years, indicating an increasing interest in this ultra-rare disease as well as an improvement in detection and diagnosis. At present, the vast majority of published research on this topic relies on case reports and case series, which are low in the hierarchy of evidence quality [16]. This highlights the need for the design of stronger studies, with a better quality of evidence, to be conducted on the burden of TIO particularly capturing wider aspects of health related QoL. This will allow predictions to be formulated and the findings transferred to the wider patient population. Nonetheless, the contribution of case studies and case series to medical advancements is recognised, particularly in the case of rare and ultra-rare diseases [20]. The inclusion of case reports in literature reviews, such as this one, summarises the state of the research on this topic and increases its usefulness in clinical practice [21].
The data collected showed that TIO presents itself with a spectrum of signs and symptoms which contribute to a substantial burden of disease. Pain was the outcome of TIO most frequently reported in the reviewed literature. Almost all case reports analysed described forms of generalised or localised pain associated with the disease. The only study included in this review that used a specific PROM to collect data on pain (the Brief Pain Inventory–Short Form) found that patients with TIO experienced moderate pain that interfered severely with their activities of daily living and affected their mood [4]. Additionally, the study found that all patients experienced bone pain [4]. This is significant in the characterisation of the burden of disease, as, in general, chronic pain has been associated with a reduction in QoL [22]. Outside the TIO setting, Hadi et al. [23] found patients suffering from chronic pain to have a reduced overall QoL compared with other patients with long-term health conditions. The authors highlighted the impact of pain on various domains of QoL, including a reduced ability to function well in day-to-day living and interferences with social life and mood. Patients involved in the study also described the negative impacts of chronic pain on their professional and social lives and on their ability to sleep and to engage in physical activities [23]. Patients suffering chronic pain also seem to have a predisposition to depression [24], and the co-occurrence of depression and pain may exacerbate other physical and psychological symptoms [25]. Interestingly, although pain was the most frequently reported symptom in the articles included in this review, a clear causative relation between pain and depression was reported only in one case study. The article described the experience of a patient with TIO who attempted suicide due to the unbearable bone pain suffered before the diagnosis [26]. The other articles reviewed did not investigate the relation between pain and depression. This might be because almost all articles reported data from clinicians who focussed on the clinical manifestations and symptoms of the disease and may have not captured the wider health related QoL impacts of TIO such as depression. Although pain might contribute to the burden of disease for patients with TIO, the treatment options currently available for the condition, including complete removal of the causative tumour and medical treatment with conventional therapy of burosumab in the case of inoperable tumours, have shown to resolve pain symptoms of TIO in most cases [11]. Day et al. [27] describe the experience of a woman with TIO treated with burosumab, whose pain symptoms had improved after 7 weeks from treatment initiation, significantly reducing her burden of disease and allowing her to recover most of her functional abilities.
To a lesser extent, the articles reviewed described skeletal manifestations, in particular fractures, pseudo-fractures, and weakness, as outcomes of TIO. Several studies reported impacts on physical health, particularly on patients’ mobility, movement agility and the need to use mobility aids. Physical-related impacts have been documented as some of the most challenging consequences experienced by patients suffering from different forms of chronic hypophosphatemia, including TIO [28]. Hypophosphatemic patients have previously described reduced or impaired mobility as an additional source of pain and fatigue, which limits their ability to take part in social and leisure activities. Patients explained that simple day-to-day chores such as getting in and out of bed, driving a car or standing up from a squatting position required a great amount of energy and caused a lot of pain [28]. Studies on another form of hypophosphatemia (X-linked hypophosphatemia, XLH) analysed the intertwining of pain, stiffness, reduced mobility and fatigue in patients affected by XLH. These were associated with impacts on the psychological wellbeing and an overall reduction in QoL [29, 30]. Although the consequences of such skeletal manifestations and physical impacts on psychological and social wellbeing have not been documented specifically for patients with TIO, they might represent a significant burden for patients suffering from it. It is important to note that this was not discovered in the reviewed literature. This might be due to the majority of the data analysed being reported by clinicians and not by patients. As in the case of pain symptoms, the available treatment options for TIO might be effective in reducing the burden of skeletal manifestations. Jan De Beur et al. [7] analysed the experience of patients treated with burosumab. At treatment initiation, most patients presented skeletal manifestations of TIO, including fractures, pseudo fractures and impaired physical functioning. The treatment was associated with enhanced fracture/pseudo fracture healing, decreases in the number of new fractures, and improvements in physical functioning.
Noticeably, very few articles included in this review explore the impacts of TIO on work life and emotional wellbeing. Despite the rising number of clinical publications on TIO over the past 10 years, only 5 articles among the ones analysed in this review reported TIO’s emotional and work life burden. However, studies have shown how outcomes such as chronic pain, restricted mobility, weakness and fatigue can have significant psychological and social consequences on patients [22, 24]. The spectrum of signs and symptoms associated with TIO might have complex psychosocial consequences. The Voice of the Patient Report [28] provides an overview of the perspectives of adults living with forms of chronic hypophosphatemia (including TIO). Patients with hypophosphatemia reported a fear of becoming completely incapacitated and dependent on carers/family members due to their condition. Patients described the financial burden of the disease as a source of additional stress and anxiety [28].
This review identified a few patterns in the co-presentation of signs and symptoms of TIO. It is evident that the majority of patients with TIO experience localised or generalised pain co-occurring with skeletal problems and weakness. Awareness of this cluster of signs and symptoms may assist with diagnosis. The review of case reports and case series did not allow for the identification of other presentation patterns. Broader observations of the clinical presentation of the disease with larger patient samples may help identify clear presentation patterns of signs and symptoms. Previous literature is aligned in recommending physicians to measure the blood serum phosphate of a patient presenting with unexplained symptoms such as pain, fractures, muscle weakness, fatigue and decreased mobility as a first step to establish the presence of hypophosphatemia [5, 11, 12]. Patients with TIO will have abnormally low serum phosphorus levels [12].Serum phosphate assessment is yet not part of the routine evaluation in many clinical centres, which causes many diagnoses of hypophosphatemia to be missed, ultimately delaying the diagnosis of TIO [5, 7].
Population-based epidemiological studies, such as the one conducted by Abrahamsen et al. [6] using national health registries, could facilitate a better understanding of the patient population, TIO prevalence and incidence, and disease presentation and prognosis. Furthermore, comprehensive disease knowledge can help researchers conduct adequate studies with limited patient samples and increase understanding of the disease burden on patients’ QoL [31]. As recommended by Seefried et al. [32], in a review which documents the burden of disease of XLH, long-term observational data are needed to understand the progression of disease burden and its impact on patients’ QoL and potential risk factors for declining physical, emotional and social function.
Further research is also needed to better understand the psychosocial dimension of this disease to inform treatment and support programs for TIO patients. This should be done through the collection of patient-reported data as only a minority of studies included in this review and none of the case studies presented data directly reported by patients; rather, the data were reported by clinicians or extracted from medical records. Developing standards for assessing self-perceived QoL in TIO patients would support clinicians in evaluating patients’ needs, inform treatment strategies and support longitudinal monitoring of disease outcomes.
Limitations
This literature review does not distinguish between TIO signs and symptoms presenting before or after treatment. In most cases, surgical removal of the causative tumour has shown to bring serum phosphate and FGF-23 levels back to normal over time, alleviating the clinical complaints of TIO [3]. Other medical therapies, such as burosumab, while not curative, have shown to be effective in the control of TIO [5], resulting in significant improvements in patients’ health-related QoL [7, 10]. Therefore, the burden of disease of TIO may be significantly different before and after treatment.
This analysis is largely based on data from case reports and case series. Although case studies might provide detailed information on a rare condition and insights for further research, they lack in scientific rigour and their findings may not be transferable to other settings and other patients.
All but 2 articles reported data retrieved from a single healthcare professional’s perspective, which may have led to reporting biases. The limited use of PROMs in the included literature is also a true limitation in the characterisation of patients’ burden of TIO. This might partially explain the underreporting of certain TIO outcomes in this review, specifically those related to the psychological sphere.
Conclusions
At present, the vast majority of research on TIO relies on case reports and case series. This underlines the need for the design of studies with a better quality of evidence to be conducted on the burden of TIO, particularly relation to psychosocial and wellbeing which is rarely described in the literature to date.
People with TIO present with a spectrum of signs and symptoms that impose a significant burden. These patients experience chronic pain, weakness, skeletal-related clinical manifestations and limitations in mobility. Based on this analysis, although certain signs and symptoms are frequently co-presented, it was not possible to identify any characteristic pattern related to TIO that could aid early recognition, which could be a focus of further research to ease the diagnosis of TIO and avoid clinical delays.
References
Chong WH, Molinolo AA, Chen CC, Collins MT (2011) Tumor-induced osteomalacia. Endocr Relat Cancer 18:R53-77. https://doi.org/10.1530/ERC-11-0006
Hautmann AH, Hautmann MG, Kolbl O, Herr W, Fleck M (2015) Tumor-induced osteomalacia: an up to-date review. Curr Rheumatol Rep 17:512. https://doi.org/10.1007/s11926-015-0512-5
Yin Z, Du J, Yu F, Xia W (2018) Tumor-induced osteomalacia. Osteoporos Sarcopenia 4:119–127. https://doi.org/10.1016/j.afos.2018.12.001
Jerkovich F, Nunez S, Mocarbel Y et al (2021) Burden of disease in patients with tumor-induced osteomalacia. JBMR Plus 5:e10436. https://doi.org/10.1002/jbm4.10436
Florenzano P, Hartley IR, Jimenez M, Roszko K, Gafni RI, Collins MT (2021) Tumor-induced osteomalacia. Calcif Tissue Int 108:128–142. https://doi.org/10.1007/s00223-020-00691-6
Abrahamsen B, Smith CD, Minisola S (2021) Epidemiology of tumor-induced osteomalacia in Denmark. Calcif Tissue Int 109:147–156. https://doi.org/10.1007/s00223-021-00843-2
Jan de Beur SM, Miller PD, Weber TJ et al (2021) Burosumab for the treatment of tumor-induced osteomalacia. J Bone Miner Res 36:627–635. https://doi.org/10.1002/jbmr.4233
Lamb YN (2018) Burosumab: first global approval. Drugs 78:707–714. https://doi.org/10.1007/s40265-018-0905-7
Portale AA, Carpenter TO, Brandi ML, Briot K, Cheong HI, Cohen-Solal M, Crowley R, Jan De Beur S, Eastell R, Imanishi Y (2019) Continued beneficial effects of burosumab in adults with X-linked hypophosphatemia: results from a 24-week treatment continuation period after a 24-week double-blind placebo-controlled period. Calcif Tissue Int 105:271–284. https://doi.org/10.1007/s00223-019-00568-3
Imanishi Y, Ito N, Rhee Y, Takeuchi Y, Shin CS, Takahashi Y, Onuma H, Kojima M, Kanematsu M, Kanda H (2021) Interim analysis of a phase 2 open-label trial assessing burosumab efficacy and safety in patients with tumor-induced osteomalacia. J Bone Miner Res 36:262–270. https://doi.org/10.1002/jbmr.4184
Brandi ML, Clunie GPR, Houillier P, Jan de Beur SM, Minisola S, Oheim R, Seefried L (2021) Challenges in the management of tumor-induced osteomalacia (TIO). Bone 152:116064. https://doi.org/10.1016/j.bone.2021.116064
Dahir K, Zanchetta MB, Stanciu I et al (2021) Diagnosis and management of tumor-induced osteomalacia: perspectives from clinical experience. J Endocr Soc 5:bvab099. https://doi.org/10.1210/jendso/bvab099
Jiang Y, Xia WB, Xing XP et al (2012) Tumor-induced osteomalacia: an important cause of adult-onset hypophosphatemic osteomalacia in China: Report of 39 cases and review of the literature. J Bone Miner Res 27:1967–1975. https://doi.org/10.1002/jbmr.1642
Flourish Flourish Data Visualization & Storytelling. https://www.flourish.studio/ Accessed 11 Jan 2022
Sayre JW, Toklu HZ, Ye F, Mazza J, Yale S (2017) Case reports, case series - from clinical practice to evidence-based medicine in graduate medical education. Cureus 9:e1546. https://doi.org/10.7759/cureus.1546
Murad MH, Sultan S, Haffar S, Bazerbachi F (2018) Methodological quality and synthesis of case series and case reports. BMJ Evid Based Med 23:60–63. https://doi.org/10.1136/bmjebm-2017-110853.17
Feng J, Jiang Y, Wang O, Li M, Xing X, Huo L, Li F, Yu W, Zhong D-r, Jin J (2017) The diagnostic dilemma of tumor induced osteomalacia: a retrospective analysis of 144 cases. Endocrine J EJ16–0587. https://doi.org/10.1507/endocrj.EJ16-0587
Zuo Q-y, Wang H, Li W, Niu X-h, Huang Y-h, Chen J, You Y-h, Liu B-y, Cui A-m, Deng W (2017) Treatment and outcomes of tumor-induced osteomalacia associated with phosphaturic mesenchymal tumors: retrospective review of 12 patients. BMC Musculoskeletal Disord 18:1–9. https://doi.org/10.1186/s12891-017-1756-1
Mueller M, D’Addario M, Egger M, Cevallos M, Dekkers O, Mugglin C, Scott P (2018) Methods to systematically review and meta-analyse observational studies: a systematic scoping review of recommendations. BMC Med Res Methodol 18:1–18. https://doi.org/10.1186/s12874-018-0495-9
Nakamura T, Igarashi H, Ito T, Jensen RT (2014) Important [sic] of case-reports/series, in rare diseases: using neuroendocrine tumors as an example. World J Clin Cases 2:608–613. https://doi.org/10.12998/wjcc.v2.i11.608
Sampayo-Cordero M, Miguel-Huguet B, Malfettone A, Perez-Garcia JM, Llombart-Cussac A, Cortes J, Pardo A, Perez-Lopez J (2020) The value of case reports in systematic reviews from rare diseases. The example of enzyme replacement therapy (ERT) in patients with mucopolysaccharidosis type II (MPS-II). Int J Environ Res Public Health 17:(18):E6590. https://doi.org/10.3390/ijerph17186590.
Dueñas M, Ojeda B, Salazar A, Mico JA, Failde I (2016) A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res 9:457–467. https://doi.org/10.2147/JPR.S105892
Hadi MA, McHugh GA, Closs SJ (2019) Impact of chronic pain on patients’ quality of life: a comparative mixed-methods study. J Patient Exp 6:133–141. https://doi.org/10.1177/2374373518786013
Fishbain DA, Cutler R, Rosomoff HL, Rosomoff RS (1997) Chronic pain-associated depression: antecedent or consequence of chronic pain? A review. Clin J Pain 13:116–137. https://doi.org/10.1097/00002508-199706000-00006
IsHak WW, Wen RY, Naghdechi L et al (2018) Pain and depression: a systematic review. Harv Rev Psychiatry 26:352–363. https://doi.org/10.1097/HRP.0000000000000198
Seemann L, Padala SA, Mohammed A, Belayneh N (2019) Tumor-induced osteomalacia and the importance of plasma fibroblast growth factor 23 as an indicator: diagnostic delay leads to a suicide attempt. J Investig Med High Impact Case Rep 7:2324709619895162. https://doi.org/10.1177/2324709619895162
Day AL, Gutiérrez OM, Guthrie BL, Saag KG (2020) Burosumab in tumor-induced osteomalacia: a case report. Joint Bone Spine 87:81–83. https://doi.org/10.1016/j.jbspin.2019.07.012
The Symposium on Hypophosphatemia: Past P, and Future, (2019) XLH Network; (Voice of the Patient Report)
Lo SH, Lachmann R, Williams A, Piglowska N, Lloyd AJ (2020) Exploring the burden of X-linked hypophosphatemia: a European multi-country qualitative study. Qual Life Res 29:1883–1893. https://doi.org/10.1007/s11136-020-02465-x
Linglart A, Dvorek-Ewell M, Marshall A, Martin JS, Skrinar A (2015) Impaired mobility and pain significantly impact the quality of life of children with X-linked hypophosphatemia. Bone Abstracts. Bioscientifica]. http://www.bone-abstracts.org/ba/0004/ba0004p198. Accessed 11 Jan 2022
Boulanger V, Schlemmer M, Rossov S, Seebald A, Gavin P (2020) Establishing patient registries for rare diseases: rationale and challenges. Pharmaceut Med 34:185–190. https://doi.org/10.1007/s40290-020-00332-1
Seefried L, Smyth M, Keen R, Harvengt P (2021) Burden of disease associated with X-linked hypophosphataemia in adults: a systematic literature review. Osteoporos Int 32:7–22. https://doi.org/10.1007/s00198-020-05548-0
Funding
The study was funded by Kyowa Kirin International.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
SM works for Sapienza University of Rome. He served as a speaker for Amgen, Bruno Farmaceutici, Diasorin, Eli Lilly, Sandoz, Takeda and Kyowa Kirin and was on the advisory board of Abiogen, Kyowa Kirin, Pfizer and UCB. AB and SAV work for OPEN Health. SW and AW work for Kyowa Kirin International.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Table 3
Table 4
Table 5
Table 6
Table 7
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Minisola, S., Barlassina, A., Vincent, SA. et al. A literature review to understand the burden of disease in people living with tumour-induced osteomalacia. Osteoporos Int 33, 1845–1857 (2022). https://doi.org/10.1007/s00198-022-06432-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-022-06432-9