
Abstract
Summary
It is of great importance to investigate any potential detrimental effect on bone health in young adults with 21-hydroxylase enzyme deficiency undergoing glucocorticoid replacement therapy. This study demonstrated normal bone health in well-controlled patients. Additionally, glucocorticoid dose may play an important role in the mineral density of femoral neck region.
Purpose
To compare regional bone mineral densities (BMDs) and bone statuses of young adults with congenital adrenal hyperplasia (CAH) due to 21-hydroxylase enzyme (21OHase) deficiency with a control group. The duration and dose of glucocorticoid therapy and relative skeletal muscle index (an indicator of sarcopenia) were also analyzed as parameters to predict bone health.
Methods
This case–control study included 23 patients (7 male and 16 female) and 20 controls (8 male and 12 female) matched by age range (18 to 31 years). Dual energy X-ray absorptiometry and phalangeal quantitative ultrasound (QUS) were used to estimate BMD and bone status, respectively.
Results
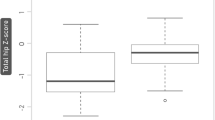
No difference was observed between patients and controls (of both sexes) in absolute values of BMD and Z-scores for the total body, lumbar spine, and femoral neck; or the bone status (estimated by phalangeal QUS). Multiple linear regression analysis demonstrated that relative skeletal muscle index independently correlated with BMD of the entire body (β: 0.67, P = 0.007), the lumbar spine (β: 0.73, P = 0.005), and the femoral neck (β: 0.67, P = 0.007). However, the dose of glucocorticoids (β: − 0.38, P = 0.028) independently correlated with BMD in the femoral neck region alone.
Conclusion
No signs of change in bone health were observed in patients with CAH when compared to the reference group. Additionally, a marker of sarcopenia was demonstrated to have a role in mineral density mechanisms in all analyzed bone sites. Only the femoral neck BMD seemed to be significantly dependent on glucocorticoid dose.

Similar content being viewed by others


References
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy (2001) Osteoporosis prevention, diagnosis, and therapy. JAMA 285:785–795. https://doi.org/10.1001/jama.285.6.785
Armas LAG, Recker RR (2012) Pathophysiology of osteoporosis: new mechanistic insights. Endocrinol Metab Clin North Am 41:475–486. https://doi.org/10.1016/j.ecl.2012.04.006
Jain RK, Vokes T (2017) Dual-energy X-ray absorptiometry. J Clin Densitom 20:291–303. https://doi.org/10.1016/j.jocd.2017.06.014
Gonnelli S, Cepollaro C (2002) The use of ultrasound in the assessment of bone status. J Endocrinol Invest 25:389–397. https://doi.org/10.1007/BF03344023
Claahsen-van der Grinten HL, Speiser PW, Ahmed SF et al (2021) Congenital adrenal hyperplasia—current insights in pathophysiology, diagnostics and management. Endocr Rev. https://doi.org/10.1210/endrev/bnab016
Speiser PW, Arlt W, Auchus RJ et al (2018) Congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 103:4043–4088. https://doi.org/10.1210/jc.2018-01865
Bachelot A, Chakhtoura Z, Samara-Boustani D et al (2010) Bone health should be an important concern in the care of patients affected by 21 hydroxylase deficiency. Int J Pediatr Endocrinol 2010. https://doi.org/10.1155/2010/326275
Ünal S, Alikaşifoğlu A, Özön A, et al (2020) Effect of long-term glucocorticoid therapy on bone mineral density of the patients with congenital adrenal hyperplasia. Turk J Pediatr 62:359–366. https://doi.org/10.24953/turkjped.2020.03.002
Delvecchio M, Soldano L, Lonero A et al (2015) Evaluation of impact of steroid replacement treatment on bone health in children with 21-hydroxylase deficiency. Endocrine 48:995–1000. https://doi.org/10.1007/s12020-014-0332-9
Metwalley KA, El-Saied A-RA-H (2014) Bone mineral status in Egyptian children with classic congenital adrenal hyperplasia. A single-center study from Upper Egypt. Indian J Endocrinol Metab 18:700–704. https://doi.org/10.4103/2230-8210.139236
Riehl G, Reisch N, Roehle R et al (2020) Bone mineral density and fractures in congenital adrenal hyperplasia: findings from the dsd-LIFE study. Clin Endocrinol 92:284–294. https://doi.org/10.1111/cen.14149
Auer MK, Paizoni L, Hofbauer LC et al (2020) Effects of androgen excess and glucocorticoid exposure on bone health in adult patients with 21-hydroxylase deficiency. J Steroid Biochem Mol Biol 204:105734. https://doi.org/10.1016/j.jsbmb.2020.105734
de Araujo M, Sanches MR, Suzuki LA et al (1996) Molecular analysis of CYP21 and C4 genes in Brazilian families with the classical form of steroid 21-hydroxylase deficiency. Braz J Med Biol Res 29:1–13
Lau IF, Soardi FC, Lemos-Marini SH et al (2001) H28+C insertion in the CYP21 gene: a novel frameshift mutation in a Brazilian patient with the classical form of 21-hydroxylase deficiency. J Clin Endocrinol Metab 86:5877–5880. https://doi.org/10.1210/jcem.86.12.8113
Paulino LC, Araujo M, Guerra G et al (1999) Mutation distribution and CYP21/C4 locus variability in Brazilian families with the classical form of the 21-hydroxylase deficiency. Acta Paediatr 88:275–283. https://doi.org/10.1080/08035259950170024
Soardi FC, Barbaro M, Lau IF et al (2008) Inhibition of CYP21A2 enzyme activity caused by novel missense mutations identified in Brazilian and Scandinavian patients. J Clin Endocrinol Metab 93:2416–2420. https://doi.org/10.1210/jc.2007-2594
Liu D, Ahmet A, Ward L et al (2013) A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol 9:30. https://doi.org/10.1186/1710-1492-9-30
Du Bois D, Du Bois EF (1989) A formula to estimate the approximate surface area if height and weight be known. 1916. Nutrition 5:303–311; discussion 312–313
Katzman DK, Bachrach LK, Carter DR, Marcus R (1991) Clinical and anthropometric correlates of bone mineral acquisition in healthy adolescent girls. J Clin Endocrinol Metab 73:1332–1339. https://doi.org/10.1210/jcem-73-6-1332
Carter DR, Bouxsein ML, Marcus R (1992) New approaches for interpreting projected bone densitometry data. J Bone Miner Res 7:137–145. https://doi.org/10.1002/jbmr.5650070204
Walsh MC, Hunter GR, Livingstone MB (2006) Sarcopenia in premenopausal and postmenopausal women with osteopenia, osteoporosis and normal bone mineral density. Osteoporos Int 17:61–67. https://doi.org/10.1007/s00198-005-1900-x
Gonçalves EM, Sewaybricker LE, Baptista F et al (2014) Performance of phalangeal quantitative ultrasound parameters in the evaluation of reduced bone mineral density assessed by DX in patients with 21 hydroxylase deficiency. Ultrasound Med Biol 40:1414–1419. https://doi.org/10.1016/j.ultrasmedbio.2013.12.027
Ainsworth BE, Haskell WL, Herrmann SD et al (2011) 2011 Compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc 43:1575–1581. https://doi.org/10.1249/MSS.0b013e31821ece12
Borges JH, de Oliveira DM, de Lemos-Marini SHV et al (2021) Fat distribution and lipid profile of young adults with congenital adrenal hyperplasia due to 21-hydroxylase enzyme deficiency. Lipids 56:101–110. https://doi.org/10.1002/lipd.12280
Matthews DR, Hosker JP, Rudenski AS et al (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419. https://doi.org/10.1007/BF00280883
Muthusamy K, Elamin MB, Smushkin G et al (2010) Clinical review: adult height in patients with congenital adrenal hyperplasia: a systematic review and metaanalysis. J Clin Endocrinol Metab 95:4161–4172. https://doi.org/10.1210/jc.2009-2616
Mora S, Saggion F, Russo G et al (1996) Bone density in young patients with congenital adrenal hyperplasia. Bone 18:337–340. https://doi.org/10.1016/8756-3282(96)00003-8
Stikkelbroeck NMML, Oyen WJG, van der Wilt G-J et al (2003) Normal bone mineral density and lean body mass, but increased fat mass, in young adult patients with congenital adrenal hyperplasia. J Clin Endocrinol Metab 88:1036–1042. https://doi.org/10.1210/jc.2002-021074
Girgis R, Winter JS (1997) The effects of glucocorticoid replacement therapy on growth, bone mineral density, and bone turnover markers in children with congenital adrenal hyperplasia. J Clin Endocrinol Metab 82:3926–3929. https://doi.org/10.1210/jcem.82.12.4320
Christiansen P, Mølgaard C, Müller J (2004) Normal bone mineral content in young adults with congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Horm Res 61:133–136. https://doi.org/10.1159/000075588
Wüster C, Albanese C, De Aloysio D et al (2000) Phalangeal osteosonogrammetry study: age-related changes, diagnostic sensitivity, and discrimination power. The Phalangeal Osteosonogrammetry Study Group. J Bone Miner Res 15:1603–1614. https://doi.org/10.1359/jbmr.2000.15.8.1603
Koetz KR, Ventz M, Diederich S, Quinkler M (2012) Bone mineral density is not significantly reduced in adult patients on low-dose glucocorticoid replacement therapy. J Clin Endocrinol Metab 97:85–92. https://doi.org/10.1210/jc.2011-2036
Falhammar H, Filipsson Nyström H, Wedell A et al (2013) Bone mineral density, bone markers, and fractures in adult males with congenital adrenal hyperplasia. Eur J Endocrinol 168:331–341. https://doi.org/10.1530/EJE-12-0865
Schulz J, Frey KR, Cooper MS et al (2016) Reduction in daily hydrocortisone dose improves bone health in primary adrenal insufficiency. Eur J Endocrinol 174:531–538. https://doi.org/10.1530/EJE-15-1096
Rangaswamaiah S, Gangathimmaiah V, Nordenstrom A, Falhammar H (2020) Bone mineral density in adults with congenital adrenal hyperplasia: a systematic review and meta-analysis. Front Endocrinol 11:493. https://doi.org/10.3389/fendo.2020.00493
Kraan GP, Dullaart RP, Pratt JJ et al (1998) The daily cortisol production reinvestigated in healthy men. The serum and urinary cortisol production rates are not significantly different. J Clin Endocrinol Metab 83:1247–1252. https://doi.org/10.1210/jcem.83.4.4694
Iervolino LL, Ferraz-de-Souza B, Martin RM et al (2020) Real-world impact of glucocorticoid replacement therapy on bone mineral density: retrospective experience of a large single-center CAH cohort spanning 24 years. Osteoporos Int 31:905–912. https://doi.org/10.1007/s00198-019-05268-0
Canalis E, Mazziotti G, Giustina A, Bilezikian JP (2007) Glucocorticoid-induced osteoporosis: pathophysiology and therapy. Osteoporos Int 18:1319–1328. https://doi.org/10.1007/s00198-007-0394-0
Whittier X, Saag KG (2016) Glucocorticoid-induced osteoporosis. Rheum Dis Clin North Am 42(177–189):x. https://doi.org/10.1016/j.rdc.2015.08.005
Falhammar H, Filipsson H, Holmdahl G et al (2007) Fractures and bone mineral density in adult women with 21-hydroxylase deficiency. J Clin Endocrinol Metab 92:4643–4649. https://doi.org/10.1210/jc.2007-0744
Cummings SR, Black DM, Nevitt MC et al (1993) Bone density at various sites for prediction of hip fractures. The Study of Osteoporotic Fractures Research Group. Lancet 341:72–75. https://doi.org/10.1016/0140-6736(93)92555-8
Benedetti MG, Furlini G, Zati A, Letizia Mauro G (2018) The effectiveness of physical exercise on bone density in osteoporotic patients. BioMed Res Int 2018:4840531. https://doi.org/10.1155/2018/4840531
Bakker I, Twisk JWR, Van Mechelen W, Kemper HCG (2003) Fat-free body mass is the most important body composition determinant of 10-yr longitudinal development of lumbar bone in adult men and women. J Clin Endocrinol Metab 88:2607–2613. https://doi.org/10.1210/jc.2002-021538
Acknowledgements
The authors thank the participants who gave their time and effort to participate in the study.
Funding
This work was supported by the São Paulo Research Foundation (FAPESP-2011/23460–1 and 2012/16778–8) and the Brazilian Federal Agency for Support and Evaluation of Graduate Education (CAPES/PNPD — 88887.360763/2019–00).
Author information
Authors and Affiliations
Contributions
JHB, GG, and EMG conceived and designed the analysis. DMO, SHVL, and EMG collected the data. All authors contributed to data analysis and interpretation. JHB, GG, and EMG drafted the manuscript, and all authors provided critical revisions. All authors gave final approval of the version of the manuscript submitted for publication.
Corresponding author
Ethics declarations
Ethics approval
The Research Ethics Committee of the State University of Campinas (UNICAMP) (number 768/2007) approved the procedures according to the Declaration of Helsinki for studies involving humans.
Consent to participate
All subjects provided informed consent.
Conflicts of interest
None.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Borges, J.H., de Oliveira, D.M., de Lemos-Marini, S.H.V. et al. Normal bone health in young adults with 21-hydroxylase enzyme deficiency undergoing glucocorticoid replacement therapy. Osteoporos Int 33, 283–291 (2022). https://doi.org/10.1007/s00198-021-06097-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-021-06097-w