
Abstract
Summary
Heart failure is associated with increased risk of osteoporosis. We evaluated the prevalence and predictors of osteoporosis in hospitalized patients with ADHF using quantitative computed tomography. Osteoporosis and vertebral fracture are prevalent in patients with ADHF and exercise capacity independently predicts bone mass and femoral bone geometry.
Introduction
Heart failure is associated with reduced bone mass and increased risk of osteoporotic fractures. However, the prevalence and predictors of osteoporosis in hospitalized patients with acute decompensated heart failure (ADHF) are not well understood.
Methods
Sixty-five patients (15 postmenopausal females and 50 males) with ADHF were prospectively and consecutively enrolled. After stabilization of heart failure symptoms, quantitative computed tomography for bone mineral density (BMD) and femoral geometry as well as biochemical, echocardiographic, and cardiopulmonary exercise tests were performed.
Results
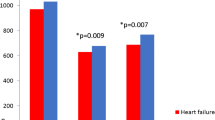
Fifteen postmenopausal female showed a high prevalence of osteoporosis (40 %) and vertebral fracture (53 %). Among 50 male patients, 12 % had osteoporosis and 32 % had osteopenia, while vertebral fracture was found in 12 %. Lumbar volumetric BMD (vBMD) was significantly lower in ischemic patients than non-ischemic patients (107.9 ± 47.5 vs. 145.4 ± 40.9 mg/cm3, p = 0.005) in male. Exercise capacity, indicated by peak oxygen consumption (VO2), was significantly associated with lumbar vBMD (r = 0.576, p < 0.001) and total hip areal BMD (aBMD) (r = 0.512, p = 0.001) and cortical thickness of the femur neck (r = 0.544, p = 0.001). When controlled for age, body mass index, N-terminal proBrain natriuretic protein (NT-proBNP), etiology of heart failure, hemoglobin, and thigh circumference, multivariate regression analysis revealed peak VO2 independently predicted lumbar vBMD (β = 0.448, p = 0.031), total hip aBMD (β = 0.547, p = 0.021), and cortical thickness of the femur neck (β = 0.590, p = 0.011).
Conclusion
In male patients with ADHF, osteoporosis and vertebral fracture are prevalent, and exercise capacity independently predicts bone mass and geometry. Given that heart failure patients with reduced exercise capacity carry a substantial increased risk of fracture, proper osteoporosis evaluation is important in these patients.

Similar content being viewed by others

References
van Diepen S, Majumdar SR, Bakal JA, McAlister FA, Ezekowitz JA (2008) Heart failure is a risk factor for orthopedic fracture: a population-based analysis of 16,294 patients. Circulation 118:1946–1952
Carbone L, Buzkova P, Fink HA, Lee JS, Chen Z, Ahmed A et al (2010) Hip fractures and heart failure: findings from the Cardiovascular Health Study. Eur Heart J 31:77–84
Majumdar SR, Ezekowitz JA, Lix LM, Leslie WD (2012) Heart failure is a clinically and densitometrically independent risk factor for osteoporotic fractures: population-based cohort study of 45,509 subjects. J Clin Endocrinol Metab 97:1179–1186
Jankowska EA, Jakubaszko J, Cwynar A, Majda J, Ponikowska B, Kustrzycka-Kratochwil D et al (2009) Bone mineral status and bone loss over time in men with chronic systolic heart failure and their clinical and hormonal determinants. Eur J Heart Fail 11:28–38
Lyons KJ, Majumdar SR, Ezekowitz JA (2011) The unrecognized burden of osteoporosis-related vertebral fractures in patients with heart failure. Circ Heart Fail 4:419–424
Terrovitis J, Zotos P, Kaldara E, Diakos N, Tseliou E, Vakrou S et al (2012) Bone mass loss in chronic heart failure is associated with secondary hyperparathyroidism and has prognostic significance. Eur J Heart Fail 14:326–332
McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K et al (2012) ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European society of cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J 33:1787–1847
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH et al (2013) 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 128:1810–1852
Tejero Garcia S, Giraldez Sanchez MA, Cejudo P, Quintana Gallego E, Dapena J, Garcia Jimenez R et al (2011) Bone health, daily physical activity, and exercise tolerance in patients with cystic fibrosis. Chest 140:475–481
Vaquero-Barrios JM, Arenas-de Larriva MS, Redel-Montero J, Bujalance-Cabrera C, Santos-Luna F, Moreno-Casado P et al (2010) Bone mineral density in patients with chronic obstructive pulmonary disease who are candidates for lung transplant. Transplant Proc 42:3020–3022
Vosse D, de Vlam K (2009) Osteoporosis in rheumatoid arthritis and ankylosing spondylitis. Clin Exp Rheumatol 27:S62–S67
Jarfelt M, Fors H, Lannering B, Bjarnason R (2006) Bone mineral density and bone turnover in young adult survivors of childhood acute lymphoblastic leukaemia. Eur J Endocrinol 154:303–309
Quinones MA, Waggoner AD, Reduto L, Nelson J, Young J, Winters W et al (1981) A new, simplified and accurate method for determining ejection fraction with two-dimensional echocardiography. Circulation 64:744–753
Folland E, Parisi A, Moynihan P, Jones DR, Feldman CL, Tow D (1979) Assessment of left ventricular ejection fraction and volumes by real-time, two-dimensional echocardiography. A comparison of cineangiographic and radionuclide techniques. Circulation 60:760–766
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137–1148
Arnett TR (2010) Acidosis, hypoxia and bone. Arch Biochem Biophys 503:103–109
Chhokar VS, Sun Y, Bhattacharya SK, Ahokas RA, Myers LK, Xing Z et al (2004) Loss of bone minerals and strength in rats with aldosteronism. Am J Physiol Heart Circ Physiol 287:H2023–H2026
Carbone LD, Cross JD, Raza SH, Bush AJ, Sepanski RJ, Dhawan S et al (2008) Fracture risk in men with congestive heart failure risk reduction with spironolactone. J Am Coll Cardiol 52:135–138
Leistner DM, Seeger FH, Fischer A, Roxe T, Klotsche J, Iekushi K et al (2012) Elevated levels of the mediator of catabolic bone remodeling RANKL in the bone marrow environment link chronic heart failure with osteoporosis. Circ Heart Fail 5:769–777
Bikle DD, Halloran BP (1999) The response of bone to unloading. J Bone Miner Metab 17:233–244
Trebacz H (2001) Disuse-induced deterioration of bone strength is not stopped after free remobilization in young adult rats. J Biomech 34:1631–1636
Baxter-Jones AD, Kontulainen SA, Faulkner RA, Bailey DA (2008) A longitudinal study of the relationship of physical activity to bone mineral accrual from adolescence to young adulthood. Bone 43:1101–1107
Michalopoulou M, Kambas A, Leontsini D, Chatzinikolaou A, Draganidis D, Avloniti A et al (2013) Physical activity is associated with bone geometry of premenarcheal girls in a dose-dependent manner. Metabolism 62:1811–1818
Gregory JS, Aspden RM (2008) Femoral geometry as a risk factor for osteoporotic hip fracture in men and women. Med Eng Phys 30:1275–1286
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Youn, JC., Lee, S.J., Lee, H.S. et al. Exercise capacity independently predicts bone mineral density and proximal femoral geometry in patients with acute decompensated heart failure. Osteoporos Int 26, 2121–2129 (2015). https://doi.org/10.1007/s00198-015-3112-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-015-3112-3