
Abstract
Summary
A reduced reimbursement for office-based dual-energy X-ray absorptiometry (DXA) is likely to exacerbate the burden of fractures in rural areas. Our cost-effective analysis suggests that, in areas where access to DXA is limited, treatment for women at high clinical risk for fractures could both improve health and save money.
Introduction
To evaluate the cost-effectiveness of various fracture prevention strategies for rural women with limited access to dual-energy X-ray absorptiometry (DXA).
Methods
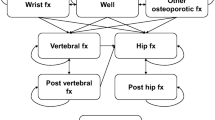
A Markov model was developed using data from the published literature and the Manitoba Bone Density Program. The participants were a simulated cohort of rural women aged 65 years with travel distance between 10 and 24 mi to the nearest DXA site. The evaluated strategies were (1) watchful waiting, (2) bone mineral density (BMD)-based strategy (i.e., DXA screening followed by pharmacotherapy based on BMD), and (3) clinical risk factor (CRF)-based strategy (i.e., pharmacotherapy for women at high risk for fractures by the World Health Organization Fracture Risk Assessment Tool [FRAX]). The outcome was an incremental cost-effectiveness ratio (ICER) measured by cost per quality-adjusted life-year (QALY) gained. The analysis was preformed from a societal perspective over a lifetime horizon.
Results
In the base-case analysis, the BMD-based strategy had an ICER of $6000 per QALY gained. For those with travel distance between 25 and 39 mi, the BMD-based strategy would have an ICER of $140,800 per QALY gained. For those with travel distance greater than 40 mi, the CRF-based strategy would be more effective and less costly than other strategies.
Conclusions
In areas where DXA is readily available, DXA screening followed by pharmacotherapy guided by BMD would be preferred. In areas with more limited access to DXA, pharmacotherapy for women at high clinical risk for fractures based on FRAX could both improve health and save money from the societal perspective.



Similar content being viewed by others


References
U.S. Preventive Services Tasks Force (2011) Screening for Osteoporosis: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med 154:356–364
National Osteoporosis Foundation (2013) Clinician's Guide to Prevention and Treatment of Osteoporosis. National Osteoporosis Foundation, Washington, http://nof.org/files/nof/public/content/file/950/upload/523.pdf. Accessed 31 Aug 31 2014
King AB, Fiorentino DM (2011) Medicare payment cuts for osteoporosis testing reduced use despite tests’ benefit in reducing fractures. Health Aff (Millwood) 30:2362–2370
American College of Rheumatology (2014) National Medicare Fee Schedule. https://www.rheumatology.org/Practice/Office/Medicare/Table_I__2014_National_Medicare_Fee_Schedule/. Accessed 31 Aug 2014
Hayes BL, Curtis JR, Laster A et al (2010) Osteoporosis care in the United States after declines in reimbursement for DXA. J Clin Densitom 13:352–360
O’Malley CD, Johnson SS, Lenhart G et al (2011) Trends in dual-energy x-ray absorptiometry in the United States, 2000-2009. J Clin Densitom 14:100–107
McAdam-Marx C, Unni S, Ye X et al (2012) Effect of Medicare reimbursement reduction for imaging services on osteoporosis screening rates. J Am Geriatr Soc 60:511–516
Yoo JW, Nakagawa S, Kim S (2012) Effect of reimbursement reductions on bone mineral density testing for female Medicate beneficiaries. J Women Health (Larchmt) 21:1144–1148
Zhang J, Delzell E, Zhao H et al (2012) Central DXA utilization shifts from office-based to hospital-based settings among Medicare beneficiaries in the wake of reimbursement changes. J Bone Miner Res 27:858–864
Curtis JR, Laster A, Becker DJ et al (2009) The geography availability and associated utilization of dual-energy x-ray absorptiometry (DXA) testing among older persons in the United States. Osteoporosis Int 20:1553–1561
Cadarette SM, Gignac MA, Jaglal SB et al (2007) Access to osteoporosis treatment is critically linked to access to dual-energy x-ray absorptiometry testing. Med Care 45:896–901
Kern LM, Powe NR, Levine MA et al (2005) Association between screening for osteoporosis and the incidence of hip fracture. Ann Intern Med 142:173–181
National Osteoporosis Guideline Group (2014) Guideline for diagnosis and management of osteoporosis in postmenopausal women and men from the 50 years in UK. http://www.shef.ac.uk/NOGG/NOGG_Pocket_Guide_for_Healthcare_Professionals.pdf. Accessed 31 Aug 2014
Kanis JA, McCloskey E, Johansson H et al (2012) FRAX (®) with and without bone mineral density. Calcif Tissue Int 90:1–13
Leslie WD, Majumdar SR, Lix LM et al (2012) High fracture probability with FRAX usually indicates densitometric osteoporosis: implications for clinical practice. Osteoporosis Int 23:391–397
Leslie WD, Morin S, Lix LM et al (2012) Fracture risk assessment without bone density measurement in routine clinical practice. Osteoporosis Int 23:75–85
Berry SD, Samelson EJ, Pencina MJ et al (2013) Repeat bone mineral density screening and prediction of hip and major osteoporotic fracture. JAMA 310:1256–1262
Ito K, Hollenberg JP, Charlson ME (2009) Using the osteoporosis self-assessment tool for referring older men for bone densitometry: a decision analysis. J Am Gerietr Soc 57:218–224
Ito K, Elkin EB, Girotra M et al (2010) Cost-effectiveness of fracture prevention in men who receive androgen deprivation therapy for localized prostate cancer. Ann Intern Med 152:621–629
Ito K, Blinder VS, Elkin EB (2012) Cost effectiveness of fracture prevention in postmenopausal women who receive aromatase inhibitors for early breast cancer. J Clin Oncol 30:1468–1475
Gold MR, Siegel JE, Russel LB et al (1996) Cost-Effectiveness in Health and Medicine. Oxford University Press, New York
Johnell O, Kanis JA, Oden A et al (2005) Predictive value of BMD for hip and other fractures. J Bone Miner Res 20:1185–1194
Kanis JA, Johnell O, De Laet C et al (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35:375–382
Wells GA, Cranney A, Peterson J et al (2008) Alendronate for the primary and secondary prevention of osteoporotic fractures in postmenopausal women. Cochrane Database Syst Rev (1):CD001155
Haentjens P, Magaziner J, Colón-Emeric CS et al (2010) Meta-analysis: excess mortality after hip fracture among older women and men. Ann Intern Med 152:380–390
Agency for Healthcare Research and Quality (2008) National Healthcare Quality & Disparity Reports. Female Medicare beneficiaries age 65 and over who reported ever being screened for osteoporosis with a bone mass or bone density measurement. http://nhqrnet.ahrq.gov/nhqrdr/jsp/nhqrdrst.jsp?catId=0&searchkey=osteoporosis&CatLevelCB=0&resetFlg=N&submit_button=Search#snhere#snhere. Accessed 31 Aug 2014
Kothawala P, Badamgarav E, Ryu S et al (2007) Systematic review and meta-analysis of real-world adherence to drug therapy for osteoporosis. Mayo Clin Proc 82:1493–1501
Hanmer J, Lawrence WF, Anderson JP et al (2006) Report of nationally representative values for the noninstitutionalizedUS adult population for 7 health-related quality-of-life scores. Med Decis Making 26:391–400
Kanis JA, Johnell O, Oden A et al (2004) The risk and burden of vertebral fractures in Sweden. Osteoporosis Int 15:20–26
US Department of Labor (2014) Usual weekly earnings of wage and salary workers first quarter 2014. http://www.bls.gov/news.release/pdf/wkyeng.pdf. Accessed 31 Aug 2014
Probst JC, Laditka SB, Wang JY et al (2007) Effect of residence and race on burden of travel for care: cross-sectional analysis of the 2001 US National Household Travel Survey. BMC Health Serv Res 7:40
Drugstore.com http://www.drugstore.com/. Accessed 31 Aug 2014
Gabriel SE, Tosteson AN, Leibson CL et al (2002) Direct medical costs attributable to osteoporotic fractures. Osteoporos Int 13:323–330
US Department of Labor. US Consumer price index for medical care for all urban consumers. http://data.bls.gov/cpi. Accessed 31 Aug 2014
Burge R, Dowson-Hughs B, Solomon DH et al (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2002-2025.J Bone Miner Res 22:465–475
Zethraeus N, Borgström F, Ström O et al (2007) Cost-effectiveness of the treatment and prevention of osteoporosis–a review of the literature and a reference model. Osteoporosis Int 18:9–23
Arias E (2012) United Stated Life Tables, 2008. http://www.cdc.gov/nchs/data/nvsr/nvsr61/nvsr61_03.pdf. Accessed 31 Aug 2014
Nayak S, Roberts MS, Greenspan SL (2011) Cost-effectiveness of different screening strategies for osteoporosis in postmenopausal women. Ann Intern Med 155:751–761
Dawson-Hughes B, Looker AC, Tosteson AN et al (2010) The potential impact of new National Osteoporosis Foundation guideline on treatment patterns. Osteoporosis Int 21:41–52
Berry SD, Kiel DP, Donaldson MG et al (2010) Application of the new National Osteoporosis Foundation Guideline to postmenopausal women and men: the Framingham Osteoporosis Study. Osteoporosis Int 21:53–60
Kastner M, Straus SE (2008) Clinical decision support tools for osteoporosis disease management: a systematic review of randomized controlled trials. J Gen Intern Med 23:2095–2105
Elias MN, Burden AM, Cadarette SM (2011) The impact of pharmacist interventions on osteoporosis management: a systematic review. Osteoporosis Int 22:1661–1667
Reuben DB, Bassett LW, Hirsch SH et al (2002) A randomized clinical trial to assess the benefit of offering on-site mobilemammography in addition to health education for older women. AJR Am J Roentgenol 179:1509–1514
Naeim A, Keeler E, Bassett LW et al (2009) Cost-effectiveness of increasing access to mammography through mobilemammography for older women. J Am Geriatr Soc 57:285–290
Newman ED, Olenginski TP, Perruquet JL et al (2004) Using mobileDXA to improve access to osteoporosis care: unit design, program development, implementation, and outcomes. J Clin Densitom 7:71–76
Acknowledgments
The authors acknowledge the Manitoba Centre for Health Policy (MCHP) for use of data contained in the Population Health Research Data Repository (HIPC project number 2012/2013-5). The results and conclusions are those of the authors, and no official endorsement by the MCHP, Manitoba Health, or other data providers is intended or should be inferred. This article has been reviewed and approved by the members of the Manitoba Bone Density Program Committee.
Conflicts of interest
Kouta Ito declares that he has no conflict of interest. William Leslie received speaker bureau (paid to facility) from Amgen, Eli Lilly, and Novartis and research grants (paid to facility) from Amgen and Genzyme.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ito, K., Leslie, W.D. Cost-effectiveness of fracture prevention in rural women with limited access to dual-energy X-ray absorptiometry. Osteoporos Int 26, 2111–2119 (2015). https://doi.org/10.1007/s00198-015-3107-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-015-3107-0