
Abstract
Purpose
There are only few studies that focused on Kienböck’s disease with non-negative ulnar variance, even though many surgical procedures have been introduced. A combined radial wedge and shortening osteotomy was carried out for Kienböck’s disease with non-negative ulnar variance. The purpose of this article is to report the results of this procedure by analyzing the clinical and radiological data.
Material and methods
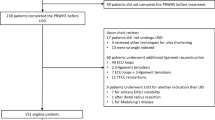
The data for patients with Kienböck’s disease who were treated by combined radial wedge and shortening osteotomy between 2007 and 2016 were retrospectively reviewed. A total of 18 patients (8 males, 10 females), average age 37 years, were included in this study and the mean follow-up period was 22.3 months. Radiological analysis included Lichtman stage, ulnar variance, radial inclination, carpal height ratio, radioscaphoid angle and Stahl’s index. Clinical analysis included range of motion (ROM), visual analog scale (VAS) score, grip power, modified Mayo wrist score (MMWS), and disabilities of arm, shoulder and hand (DASH) score.
Results
Preoperative radiological analysis showed 16 cases of Lichtman stage IIIA and 2 cases of stage IIIB. Preoperative ulnar variance was +0.51 mm, radial inclination was 27.7o, carpal height ratio was 0.49, radioscaphoid angle was 52.8o and Stahl’s index was 0.42. All patients had solid union at the osteotomy site. At the final follow-up the average ulnar variance was +1.9 mm, radial inclination was 16.5o, carpal height ratio was 0.48, radioscaphoid angle was 58.2o and Stahl’s index was 0.36. Clinical analysis showed that the average dorsiflexion of the wrist was increased by 8.4o and palmar flexion of the wrist was increased by 29.6o. Grip power was increased by an average of 9.9 kg. Average VAS at the final follow-up was 1.0, DASH score was 4.3, and modified Mayo wrist score was 78.1.
Conclusion
Radial wedge and shortening osteotomy can be recommended as an option for Kienböck’s disease with non-negative ulnar variance, based on acceptable results from this study.
Zusammenfassung
Zielsetzung
Bislang legen nur wenige Studien ihren Fokus auf die Lunatumnekrose mit Nichtminusvariante der Ulna, obwohl zahlreiche chirurgische Verfahren eingeführt wurden. Eine kombinierte radiale Keil- und Verkürzungsosteotomie wurde bei Lunatumnekrose mit Nichtminusvariante der Ulna durchgeführt. In der vorliegenden Arbeit sollen die Ergebnisse dieses Verfahrens vorgestellt werden. Dazu wurden klinische und radiologische Daten analysiert.
Material und Methoden
Retrospektiv wurden die Daten von Patienten mit Lunatumnekrose analysiert, bei denen zwischen 2007 und 2016 eine kombinierte radiale Keil- und Verkürzungsosteotomie durchgeführt worden war. Insgesamt 18 Patienten (8 männlich, 10 weiblich) in einem Durchschnittsalter von 37 Jahren wurden in die vorliegende Studie eingeschlossen. Die mittlere Follow-up-Dauer betrug 22,3 Monate. Für die radiologische Analyse wurden das Lichtman-Stadium, die Ulnarvarianz, die Radiusneigung, das karpale Höhenverhältnis („carpal height ratio“), der radioskaphoidale Winkel und der Stahl-Index berücksichtigt. Die klinische Analyse beinhaltete den Bewegungsumfang, eine visuelle Analogskala (VAS), die Griffkraft, den modifizierten Mayo-Wrist-Score (MMWS) und Funktionseinschränkungen von Arm, Schulter und Hand (Disability of Arm Shoulder and Hand [DASH]).
Ergebnisse
Die präoperative radiologische Untersuchung ergab 16 Fälle mit Lichtman-Stadium IIIA und 2 Fälle mit Stadium IIIB. Die präoperative Ulnarvarianz betrug +0,51 mm, die Radiusneigung 27,7°, das karpale Höhenverhältnis 0,49, der radioskaphoidale Winkel 52,8° und der Stahl-Index 0,42. Bei allen Patienten bestand eine feste Verbindung an der Osteotomiestelle. Im letzten Follow-up betrug die Ulnarvarianz durchschnittlich +1,9 mm, die Radiusneigung 16,5°, das karpale Höhenverhältnis 0,48, der radioskaphoidale Winkel 58,2° und der Stahl-Index 0,36. Die klinische Analyse ergab, dass die durchschnittliche Dorsalflexion des Handgelenks um 8,4° und die Palmarflexion des Handgelenks um 29,6° erhöht war. Die Griffkraft war um durchschnittlich 9,9 kg gesteigert. Der durchschnittliche VAS-Wert betrug beim letzten Follow-up 1,0, der DASH-Score 4,3 und der modifizierte Mayo-Wrist-Score 78,1.
Schlussfolgerung
Basierend auf den akzeptablen Ergebnissen der vorliegenden Studie kann die radiale Keil- und Verkürzungsosteotomie als Therapieoption bei Lunatumnekrose mit Nichtminusvariante der Ulna empfohlen werden.




Similar content being viewed by others


Abbreviations
- DASH:
-
Disabilities of arm, shoulder and hand score
- MMWS:
-
Modified Mayo wrist score
- MRI:
-
Magnetic resonance imaging
- VA-LCP:
-
Variable angle locking compression plate
- VAS:
-
Visual analog scale
References
Alexander AH, Lichtman DM (1986) Kienböck’s disease. Orthop Clin North Am 17:461–472. https://doi.org/10.1302/0301-620X.90B2.20112
Pedro K (2009) Kienböck’s disease. J Hand Surg Am 2009(34A):167–175
Golay SK, Rust P, Ring D (2016) The radiological prevalence of incidental Kienböck disease. Arch Bone Jt Surg 4:220–223. https://doi.org/10.22038/abjs.2016.5817
Innes L, Strauch RJ (2010) Systematic review of the treatment of Kienböck’s disease in its early and late stages. J Hand Surg Am 35:713–717.e4. https://doi.org/10.1016/j.jhsa.2010.02.002
Watanabe K, Nakamura R, Horii E, Miura T (1993) Biomechanical analysis of radial wedge osteotomy for the treatment of Kienböck’s disease. J Hand Surg Am 18:686–690
Afshar A, Mehdizadeh M, Khalkhali H (2015) Short-term clinical outcomes of radial shortening osteotomy and capitates shortening osteotomy in Kienböck disease. Arch Bone Jt Surg 3:207–211
Koh S, Nakamura R, Horii E et al (2003) Surgical outcome of radial osteotomy for Kienböck’s disease-minimum 10 years of follow-up. J Hand Surg Am 28:910–916
Raven EEJ, Haverkamp D, Marti RK (2007) Outcome of Kienböck’s disease 22 years after distal radius shortening osteotomy. Clin Orthop Relat Res 460:137–141. https://doi.org/10.1097/BLO.0b013e318041d309
Tatebe M, Koh S, Hirata H (2016) Long-term outcomes of radial osteotomy for the treatment of Kienböck disease. J Wrist Surg 5:92–97. https://doi.org/10.1055/s-0036-1581099
de Vries J, Souer JS, Zurakowski D, Ring D (2010) Measurement of ulnar variance on uncalibrated digital radiographic images. Hand 5:267–272. https://doi.org/10.1007/s11552-009-9249-9
Irisarri C (2004) Aetiology of Kienböck’s disease. J Hand Surg Am 29 B:281–287. https://doi.org/10.1016/j.jhsb.2004.01.006
Kristensen SS, Thomassen E, Christensen F (1986) Kienböck’s disease—late results by non-surgical treatment. A follow-up study. J Hand Surg Br 11:422–425
Nakamura R, Nakao E, Nishizuka T et al (2011) Radial osteotomy for Kienböck disease. Tech Hand Up Extrem Surg 15:48–54. https://doi.org/10.1097/BTH.0b013e31820baa36
Salmon J, Stanley JK, Trail IA (2000) Kienböck’s disease: conservative management versus radial shortening. J Bone Joint Surg Br 82:820–823
Kam B, Topper SM, McLoughlin S, Liu Q (2002) Wedge osteotomies of the radius for Kienböck’s disease: a biomechanical analysis. J Hand Surg Am 27:37–42. https://doi.org/10.1053/jhsu.2002.29489
Tatebe M, Horii E, Majima M et al (2007) Radial osteotomy for Kienböck’s disease with displaced fracture of the lunate. J Hand Surg Am 32:1343–1347. https://doi.org/10.1016/j.jhsa.2007.08.013
Chevrollier J, Pomares G, Huguet S et al (2017) Intracarpal shortening osteotomy for Kienböck’s disease: a retrospective study of 28 cases. Orthop Traumatol Surg Res 103:191–198. https://doi.org/10.1016/j.otsr.2016.12.016
Tsunoda K, Nakamura R, Watanabe K et al (1993) Changes in carpal alignment following radial osteotomy for Kienböck’s disease. J Hand Surg Br 18:289–293. https://doi.org/10.1016/0266-7681(93)90043-F
Miura H, Uchida Y, Sugioka Y (1996) Radial closing wedge osteotomy for Kienböck’s disease. J Hand Surg Am 21:1029–1034. https://doi.org/10.1016/S0363-5023(96)80311-X
Shin YH, Kim J, Gong HS, Rhee SH (2017) Clinical outcome of lateral wedge osteotomy of the radius in advanced stages of Kienböck’s disease. Clin Orthop Surg 9(3):355–362
Nakamura R, Imaeda T, Miura T (1990) Radial shortening for Kienböck’s disease: factors affecting the operative result. J Hand Surg Am 15:40–45. https://doi.org/10.1016/0266-7681(90)90045-6
Illarramendi AA, Schulz C, De Carli P (2001) The surgical treatment of Kienböck’s disease by radius and ulna metaphyseal core decompression. J Hand Surg Am 26(2):252–260. https://doi.org/10.1053/jhsu.2001.22928
Blanco RH, Blanco FR (2012) Osteotomy of the radius without shortening for kienböck disease: a 10-year follow-up. J Hand Surg Am 37(11):2221–2225
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
I.-T. Hong, S. Lee, G.c Jang, G. Kim and S.-H. Han declare that they have no competing interests.
This article does not contain any studies with human participants or animals performed by any of the authors. Informed consent was obtained from subjects who might be identifiable from information or images shown in this article or their legal guardians.
Rights and permissions
About this article

Cite this article
Hong, IT., Lee, S., Jang, G.c. et al. Kienböck’s disease with non-negative ulnar variance. Orthopäde 48, 96–101 (2019). https://doi.org/10.1007/s00132-018-3641-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00132-018-3641-5