
Abstract
Background
Mental illness is a global concern and the leading cause of years lived with disability. Research on help-seeking behaviour has focused on individual factors, but there is still much unexplained variance. Suggesting complex interactions between determinants of human behaviour a new framework called Self-Milieux is proposed to represent a person’s sociocultural background. The article introduces a statistical approach to determine Self-Milieux and exemplarily examines its predictive validity for health-related research.
Methods
Self-Milieux are determined through a two-stage clustering method based on the determinants socioeconomic status and self-construal profile. Descriptive analyses are used to compare Self-Milieux characteristics. Hierarchical binary logistic regression models test the association between Self-Milieux and help-seeking behaviour, while controlling for socioeconomic status as an established predictor.
Results
The sample size was N = 1535 (Mage = 43.17 and 64.89% female participants). Average depression severity was M = 12.22, indicating mild to moderate symptoms. Six Self-Milieux were determined and named. Participants from privileged (aOR = 0.38) and self-sufficient (aOR = 0.37) milieux were less likely to seek help from a general practitioner than those from the entitled milieu. Participants from privileged (aOR = 0.30), collaborators (aOR = 0.50), disadvantaged (aOR = 0.33), and self-sufficient (aOR = 0.21) milieux were less likely to seek help from family members than those from the entitled and family-bound milieux.
Discussion
The study’s strengths and limitations, as well as the cluster methodology, are discussed. The comparative results for the six Self-Milieux are interpreted based on current research. For example, participants from some milieux follow a help-seeking process proposed in previous research, while participants from other milieux seem to show a different process, one that ends in informal help-seeking.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of mental illness is a global concern, even in modern countries with formalised mental health care systems [1, 2]. Despite the availability of professional help, people often do not seek it or only after significant delay [3]. In Germany, this issue of non-help-seeking remains even in regions with high health care density [4, 5]. Understanding the reasons for this issue is crucial because mental illness contributes significantly to the global burden of disease and has substantial individual-level consequences [6, 7]. For example, mental illness is the leading cause of years lived with disability among all disease groups and untreated mental illness has significant economic costs for societies [8].
To address help-seeking behaviour in individuals with mental illness, psychological research has focused on various individual factors such as age, gender, personal attitudes, and influences of stigma [9, 10, 11, 12, 13]. Despite these efforts, there is still considerable unexplained variance in help-seeking behaviour of individuals, suggesting that complex interactions between determinants of human behaviour on individual and socio-contextual levels remain unclear [14, 15]. Consequently, there is a need to adopt a more interdisciplinary approach in health-related research and examine the individual as an agent of their own life who is also socialised into certain social and cultural constraints [16,17,, 17, 18]. It has been suggested that a broader perspective on social and cultural determinants might help understand the help-seeking process beyond traditional health behaviour modelling approaches [18, 19].
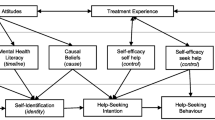
Therefore, a novel framework titled Self-Milieux is proposed that conceptualises and interprets human behaviour within a sociological framework, using the social milieu paradigm [20, 21]. This paradigm relates two orthogonal dimensions to each other, describing a person’s social status differentiated by subjective qualities along the horizontal dimension [21]. When social milieus are studied it is assumed that people within a milieu share ethical and aesthetic attitudes due to similar mentalities [21]. The novel framework is aligned with this paradigm, however, in comparison to the social milieu framework, the Self-Milieux incorporate the concept of self-construal, which was developed in cross-cultural comparative psychology [22,23,, 23, 24]. The Self-Construal Theory [22] proposes that individuals can have either an independent or interdependent self-construal, depending on cultural and social contexts [24]. Individuals with a more independent self-construal regard themselves as separate from their contexts [25] and consistent across situations [26], whereas, individuals with a more interdependent self-construal perceive themselves to be more role- and context-bound [27, 28]. This theory is relevant for understanding human emotion, motivation, and behaviour [23]. By incorporating the Self-Construal Theory within the social milieu paradigm, both the individual as well as the social level are recognised as relevant determinants within the Self-Milieux framework. Methodologically, the Self-Milieux are determined within a two-by-two coordinate system, similar to the social milieu concepts. The vertical dimension is defined by the socioeconomic status (SES) of the individual, and the horizontal dimension is defined by the self-construal profile (SCS) of the individual. This framework accounts for sociocultural factors that influence individual behaviour, which could provide a more comprehensive understanding of health-related help-seeking [19]. The Self-Milieux are visualised in Fig. 1. Individuals in the same milieu are assumed to have similar concepts of self, influenced by their respective socio-economic background and culturally related self-construal profile.

The Self-Milieux concept. The vertical dimension displays three socioeconomic status groups. The horizontal dimension displays a persons’ self-construal that ranges from highly interdependent to highly independent. The ovals represent arbitrarily placed milieux
The determinants to conceptualise Self-Milieux are chosen for two main reasons. Firstly, international research has considered both SES and self-construal concerning a multitude of psychological and sociological phenomena [e.g., 23, 24, 29, 30]. Secondly, in reciprocal processes of socialisation the regional SES and the culturally influenced understanding of the self has lasting effects on individuals influencing people across different personal and social domains of living [e.g., 17, 30, 31]. Furthermore, the Self-Milieux are proposed to be relevant in the context of health related research, because both SES and SCS have been associated with health-related behaviour and health inequality, which will be elaborated in the following sections [e.g., 32, 33, 34, 35, 36, 37].
The role of SES has been studied comprehensively in the context of health-related inequality [e.g., 34]. Phelan et al. [38] have even defined SES as a ‘fundamental cause’ of health-related inequality in mortality. The SES markers education, occupation, and income have been shown to have a significant impact on health-related opportunities, with individuals from lower SES backgrounds experiencing shorter and more health-burdened lives [39]. Additionally, regional SES has also been found to impact health outcomes [40]. Lower SES is associated with poorer health evaluation, symptom expression, and overall quality of life [41, 42]. The importance of SES in the context of health-related research is undeniable. However, it is necessary to allow for horizontal differentiation to account for inconsistencies within status groups [41]. Furthermore, the differentiation allows the influence of cultural factors to be explicitly addressed in empirical investigations.
To provide a comprehensive concept, the incorporation of self-construal as a subjective factor is proposed. It is argued that individuals are not only socialised within and into a certain SES [17, 43, 44] but, also, socialised within and into an understanding of self in relation to other [23, 24]. Self-construal is a socio-culturally influenced, overarching self-schemata that organises and regulates one’s experiences and actions, and influences intra- and inter-psychological functions, including cognitive processes, emotions, and intra-/inter-group relations [22, 23, 24, 26, 27, 28, 31, 45, 46]. More importantly for this study, a person’s self-construal has been shown to have relevant implications for health-related behaviour in different contexts, including the subjective experience of illness and protective factors against depression [e.g., 23, 47, 48, 49].
Considering the above, the primary aim of this article is two-fold. Firstly, to introduce a statistical approach to methodologically determine the concept of Self-Milieux, which represents a person’s sociocultural background instilled through socialisation. Secondly, to exemplarily show the predictive validity of the concept for health-related research, the Self-Milieux are examined regarding the help-seeking process of individuals with depressive symptoms. The help-seeking process involves self-identifying the complaints as symptoms of mental illness, forming an intention to seek help, and engaging in help-seeking behaviour [50], [51], [52].
Methods
The data for this study is taken from a project funded by the German Research Foundation (DFG), which looks at ways in which professional health care utilisation can be improved. The overall project has a study protocol [53] and was preregistered in the German Clinical Trial Register (https://drks.de/search/de/trial/DRKS00023557). The analyses done in this study are in addition to the research questions reported in the study protocol. Data was collected via an online panel between January and September 2021.
Sample
Participant recruitment was conducted with a German online-panel. Prospective participants (N = 10,348) were screened and included if they were currently not receiving health care treatment and had at least mild depressive symptoms [referring to a PHQ-9 sum score of 8 or higher; 54]. Altogether, a convenience sample of N = 1867 participants was included in the study. Before data analysis participants were excluded if they completed the survey within less than half the median study duration [55] or had apparent monotone answer profiles (n = 116), due to disparate gender data between the two study points (n = 15), and because they were of diverse gender (n = 9), leaving a sample size of N = 1727. After calculating the relevant SES indices (see further below), n = 192 were excluded from further analyses due to missing data concerning the variable “net household income”. Therefore, N = 1535 participants are included in the statistical analysis.
Measures
To measure the socioeconomic status, the SES-Index is determined using sociodemographic data, i.e., level of acquired schooling and education, type of vocation, and net household income level. The method for this is described in Lampert et al. [56]. A three-dimensional index is calculated on the basis of the meritocratic indices education, vocation, and income. The separate index values range from 1 = “low status” to 6 = “high status” and are summed up. The SES-Index values range from 3 = “low socioeconomic status” to 18 = “high socioeconomic status”. The wordings for the sociodemographic variables and exact calculations for the indices are reported in the supplementary material (Table S1).
To determine the participants status group, five quintiles are calculated for the summed SES-Index. The first quintile represents the “upper”-, the next three represent the “middle”-, and the fifth quintile represents the “lower”-status group. Two benefits arise from calculating the status in this way: first, “the distribution-based differentiation of the status groups underlines that the socioeconomic status is a measure of relative social inequality” and second, “it is ensured that there are no distortions in correlation-based analyses due to extreme cell occupations in the categories” [translated from 56]. The three meritocratic indices are separately used in the cluster analysis methodology to determine the Self-Milieux. When comparing the milieux the three status groups will be used.
To measure the participants self-construal, 24 items from four Self-Construal Scale dimensions are used, i.e., the dimensions representing the domains of personal and social functioning “making decisions”, “looking after oneself”, “communicating with others”, and “dealing with conflicting interests” [31]. Each dimension is assessed with six items, three reflecting a more independent and three a more interdependent self-construal, respectively. Response options are 1 = “does not describe me at all” to 5 = “describes me exactly”. In the supplementary material the independent vs. interdependent expressions of the dimensions as well as the items are reported (Table S2). Internal consistency across all items is very good (α = 0.82).
To calculate the separate dimension scores, first, the mean score is calculated across all items and then the acquiescence bias is corrected for by subtracting the mean score from the individual item [as suggested; 57]. The measure therefore reflects the individuals relative endorsement of each item in the context of the respective measurement occasion [31]. Second, the items measuring the interdependent self-construal are reversed. Third, the mean across the items within a dimension is calculated.
To determine the overall self-construal identification of the participants the mean across all four dimensions is calculated. Individuals with mean scores between − 1.5 and 0 will be classified as “mainly interdependent” and individuals with scores between 0 and + 1.5 will be classified as “mainly independent”. The four dimensions are separately used in the cluster analysis methodology to determine the Self-Milieux. When comparing the milieux the two classifications will be used.
Age and gender (“female” and “male”) were assessed together with the other sociodemographic variables used to determine the socioeconomic status.
Depression severity was assessed using the PHQ-9 questionnaire [58]. Participants reported how often they had complaints over the past two weeks (e.g., little interest or pleasure in doing things). Response options were 0 = “not at all”, 1 = “several days”, 2 = “more than half the days”, 3 = “nearly every day”. Sum scores (range = 0 to 27) are calculated and higher scores indicate greater severity of reported depressive symptoms. Internal consistency is acceptable (α = 0.70).
Self-identifying complaints as symptoms of mental illness was assessed using the SELF-I questionnaire [51]. Participants appraised their current problems (e.g., my present problems could be the first signs of a mental disorder) on a 5-point Likert scale from 1 = “don’t agree at all” to 5 = “agree completely”. Scores for the items 2, 4, and 5 are reversed before the mean score is calculated. Internal consistency is very good (α = 0.88).
Help-seeking intention was assessed using an adapted 15-item list [59]. Answers could be given on a 7-point Likert scale from 0 = “extremely unlikely” to 6 = “extremely likely”. We will conduct analyses for intention to seek help from a general practitioner (GP), a mental health professional (MHP; i.e., psychologist, psychotherapist, or psychiatrist), a social helper (i.e., social worker, counselling centre, teacher), a spiritual leader (i.e., priest or soothsayer), as well as informal instances, i.e., a friend or a family member. Maximum scores across the (grouped) items are taken to receive indicators for a participant’s intention to seek help. Other sources of help-seeking are not included in the analyses, e.g., police, colleague, or neurologist.
Current help-seeking behaviour was assessed using the same list to assess intention. The participants could state whether they had sought help for their psychological complaints during the past six months using a binary format (0 = “no” and 1 = “yes”). The same groups as described above for assessing intention are used in these analyses.
Previous help-seeking experience was assessed by asking participants following question: “have you ever had treatment for mental illness in your life?” Answers could be given in a binary format for different treatment types. In this study responses concerning the answer categories “medical treatment”, “psychotherapy”, “art-, music- and/or sport-therapy”, “self-help groups”, and “coaching and counselling” are considered and collapsed into one variable (0 = “has no experience” and 1 = “has experience”).
Methodologically determining the Self-Milieux
In accordance with the findings of Stephens et al. [24], it is proposed that cultural factors influence self-construal. Furthermore, it is argued that the manner in which this self-construal is formed in the context of a specific sociocultural environment (i.e., social class) is relevant. To put it another way, a culture that encourages independence or interdependece will foster it in different ways depending on the social background of the individual. To determine the Self-Milieux representing the sociocultural background of an individual, a two-stage clustering analysis method is executed [60]. The SES indices education, vocation, and net household income, as well as the four self-construal dimensions developed by Vignoles et al. [31] are used as analysis input. Together, the seven dimensions map out different sociocultural backgrounds that go beyond the original constitutional variables in a Gestalt idea. In the first stage, all cluster solutions using a hierarchical method are determined and cluster centroids for the chosen solution are calculated. In the second stage, the hierarchically determined centroids are used as initial seed points in a non-hierarchical method. The advantage of the two-stage method is that this allows for correction of possibly improper cluster membership assignments due to the issue that hierarchical cluster analysis methods strictly nest the solutions, restricting cluster membership re-assignment. The partitioning method “unnests the hierarchy and allows for all data units to be assigned to the nearest cluster centroid” while still using the hierarchically found centroids as seed points [60].
The hierarchical method used is described by Ward [61]. The non-hierarchical method used is described by MacQueen [62]. The analyses are all done using the statistics software R version 4.1.0. [63]. To implement the hierarchical cluster method, the agnes {cluster} function [64] is conducted and doubled checked using the hclust {stats} function [63]. Dendrograms are used to choose a sufficient cluster solution. The centroids of the chosen cluster solution are calculated and used as the initial seed points in the function kmeans {stats}. These cluster memberships are then used to define the cluster membership, i.e., the Self-Milieux. Cohens Kappa [65] is calculated to compare the cluster solutions between the hierarchical and non-hierarchical solutions. The z-standardised variables for the three separate SES indices and the four SCS dimensions are used as analysis input variables. All R-code specifications to determine the Self-Milieux are supplied in the supplementary material (Table S3).
Concerning the a priori determined statistical power, Dalmaijer et al. [66] conclude that even relatively small samples (n = 20 per subgroup) are sufficient, and recommend n = 20 to 30 per expected subgroup.
Statistical and power analyses
Descriptive analyses to investigate the characteristics of the Self-Milieux are conducted with the demographic variables age and gender, with depression severity, as well as with the help-seeking variables self-identifying complaints as symptoms of mental illness, help-seeking intention and behaviour, and previous treatment experience. Univariate ANOVAs with Bonferroni-adjusted post hoc comparisons or Chi-square tests with adjusted residuals (AR) for each cell are used to compare the groups. AR bigger than 2 or smaller than -2 are considered to be significant [67].
Four hierarchical binary logistic regression models are performed to test for the associations of Self-Milieux and help-seeking behaviour (criteria: general practitioner, mental health professional, friends, family). It is controlled for age, gender, depression severity, and SES as a means to analyse incremental validity (model 1, respectively). Reference milieux will be chosen depending on the descriptive analyses, i.e., the milieu in which participants show the most help-seeking behaviour (model 2, respectively). This way the robustness of the descriptive results are checked. Nagelkerke’s Pseudo R2 is reported [68].
The necessary sample size was calculated a priori using G*Power [69]. For the ANOVAs, N = 324 is sufficient (medium effect size, α = 0.05, 1−β = 0.95, six groups). For the logistic regression analyses, N = 988 is sufficient (OR = 1.3, Pr(Y = 1) H0 = 0.2, α = 0.05, 1−β = 0.95).
Cluster analysis to determine the Self-Milieux is conducted using the statistics software R version 4.1.0 [63]. All other analyses are conducted using the statistics software IBM SPSS version 29. Significance levels are set to p < 0.05.
Results
The Self-Milieux determined through the two-stage cluster analysis method
The cluster solution with six clusters is chosen as appropriate, based on the dendrograms of both the cluster analyses with a cut-off at Hight 25, as well as conceptual consistency and explanatory plausibility [see: 62].The cluster allocation is the same irrespective of the algorithm. We considered it plausible that six clusters could be discerned and described within the current study sample, with minimal overlap between the clusters. However, the method itself is exploratory and therefore inherently decisionistic. The hclust {stats} dendrogram is reported in the supplementary material (Fig. S4). The cluster centroids for the six clusters chosen as the best cluster solution can be found in the supplementary material (Table S5). These centroids are then used as the initial seed points for the partitioning method. After running the kmeans {stats} algorithm with the centroids as seed points, the participants are allocated to the nearest cluster. In the supplementary material (Table S6) the cluster allocations are shown. Cohens Kappa is moderate with Κ = 0.57 (95% CI 0.54; 0.59) when comparing the hierarchical with the non-hierarchical cluster solution.
Table 1 shows the different SES groups and SCS profile distributions in the six Self-Milieux. Additionally, the milieux are described according to the respective determinants with a creative label (see Table S5 in the supplementary material for the exact expressions along the seven dimensions). Milieu 1, “the privileged”, includes people from mainly upper SES, especially with high income, and mainly independent self-construal showing high levels of self-interest when dealing with conflicting interests. Milieu 2, “the collaborators”, includes people from mainly middle SES, especially higher vocational status, and high interdependent self-construal. Milieu 3, “the entitled”, includes people from mainly middle SES and mainly independent self-construal, except for showing a tendency to depend on others when looking after oneself. Milieu 4, “the family bound”, includes people from both middle and lower SES and higher interdependent self-construal. Milieu 5, “the disadvantaged”, includes people from both middle and lower SES and mainly independent self-construal. Milieu 6, “the self-sufficient”, includes people from mainly middle SES and more independent self-construal, except for showing a tendency to desire harmony when communicating with others.
Sample characteristics & descriptive analyses
The final sample size consisted of N = 1535 at baseline and N = 1125 three to six months later. The sample mean age is 43.17 (SD = 15.42) years old with 64.89% of the participants identifying as female and an average depression severity of 12.22 (SD = 4.14). This indicates that participants mainly report mild to moderate symptoms of depression [54]. Most participants had the German equivalent of the “international baccalaureate” (51.7%), followed by an “average ten years of schooling” (34.7%) and “nine or less years of schooling” (12.9%). Concerning net household income, most participants reported “1000–2000€ net income” (36.1%), followed by “less than 1000€” (28.6%), “2000–3000€” (20.1%), and “more than 3000€” (9.8%). In Table 2 the sample characteristics including the results of the descriptive comparative analysis, both ANOVA/ANCOVA as well as Chi-square tests, are shown in which the Self-Milieux are compared with each other.
Comparing the milieux to each other, there are significant differences. On average, participants from the family bound milieu are younger and participants from the self-sufficient milieu are older than in the other milieux. Compared with the overall gender distribution, there are more male participants in the privileged and entitled milieux than is to be expected. Correspondingly, there are more female participants in the family bound milieu than is to be expected. Depression severity is less pronounced in the privileged and entitled milieux than in the collaborator and family bound milieux.
Concerning the help-seeking process there are significant differences between the milieux. Self-identifying the experienced complaints as symptoms of mental illness is most pronounced in the collaborator milieu, especially compared with the privileged, entitled, and self-sufficient milieux. Irrespective of help-seeking source, intention to seek help is most expressed in the entitled milieu. Overall intention to seek help is most strongly expressed concerning friends, then family and then from a general practitioner. Help-seeking intention is least expressed concerning a spiritual leader. Corresponding with the higher intention to seek help from a general practitioner, participants in the entitled milieu show more than expected help-seeking behaviour. Also, based on the overall help-seeking behaviour frequencies, the entitled and family bound milieux show more than expected help-seeking behaviour from family members, whilst participants from the self-sufficient milieu show less than expected help-seeking behaviour from family members. Concerning previous treatment experience, participants from the privileged milieu reported the least experience and participants from the disadvantaged milieu reported the most treatment experience.
Logistic regressions for help-seeking behaviour
The results for the multiple logistic regressions, with the outcome variables help-seeking behaviour from a general practitioner, a mental health professional, a friend, and a family member, are reported in Table 3. SES was introduced as a control variable in the respective model 1 of the regression analyses to test the added value of the Self-Milieux against already established measures in health-related research. Overall, SES was a positive predictor for help-seeking behaviour.
Due to the non-significance of the overall statistical test concerning help-seeking from a mental health professional these results cannot be interpreted but are reported in Table 3. The other regressions were significant and are interpretable.
Concerning help-seeking from a GP, participants from the privileged and self-sufficient milieux are less likely to seek help than participants from the entitled milieu.
Concerning help-seeking from a friend, participants from the entitled, family bound, and disadvantaged milieux are more likely to seek help than participants from the self-sufficient milieu.
Concerning help-seeking from a family member, participants from the privileged, collaborators, disadvantaged, and self-sufficient milieux are less likely to seek help than participants from the family bound milieu.
Discussion
The aim of the present study was to present and test the novel framework, Self-Milieux, that represent individuals sociocultural background in an economic way for empirical research. To show the predictive validity the Self-Milieux framework was exemplarily tested in the context of the help-seeking process for mental health issues [50].
It is argued that both the social as well as the cultural background are relevant for the development of self-construal, synergistically coming together and representable as Self-Milieux. People within the same milieu have similar self-understanding and construal but do not represent actual social groups, as is the aim of social milieu concepts [21]. Furthermore, it is argued that the understanding of self will have an impact on help-seeking and non-help-seeking behaviour. This study answers the call to regard and recognise individual health-related behaviour on a psychological as well as sociocultural level [16,17,18,19].
As a means of introducing a conceptually consistent methodology to determine the Self-Milieux a two-stage clustering analysis method was used [60]. It is a method allowing for re-allocation of cluster membership. Cohens Kappa was moderate, indicating that a sufficient number of participants were allocated to the same cluster in both stages but that some necessary miss-allocations were rectified and individuals reassigned to the nearest cluster centroid. Six clusters were chosen to represent different milieux based on the hierarchical cluster dendrograms and explanatory plausibility [62]. The clusters are distributed equally across the three SES status groups which is due to the chosen methodology representing relative status groups [56]. Two of the clusters are mainly interdependent, whereas four are mainly independent with significant differences concerning the self-construal dimensions. It is important to note that on a conceptual level the horizontal dimension ranges from highly interdependent to highly independent. The empirical model however shows less extreme self-construal profiles. This is likely due to a study sample bias and the limitation that only people registered at the online panel could participate (see Sect. “Strengths and limitations”).
Also, there is some criticism concerning the method itself. First, the cluster analysis process is inherently conditional and decisionistic, meaning that other cluster solutions would have been possible. Second, it is criticised that there is a lack of standardised reporting guidelines making it difficult to compare and replicate studies [70]. However, because this is an introduction of a novel framework the methodology is considered sufficient and in the supplementary material the R-code was provided so that replication is possible.
To show the predictive validity, the Self-Milieux are exemplarily examined regarding variables of the help-seeking process [50]. The main finding is that participants from different milieux show significant differences when it comes to the separate parts of this help-seeking process and how these are associated with each other. Importantly, the resulting differences could be shown with the socioeconomic status introduced in the models as a control variable due to its established role in health related behaviour [e.g., 34, 38]. Therefore, it is concluded that introducing the Self-Construal Theory [45] in such a milieux framework has added value for understanding help-seeking behaviour in a health related context. The impact of the milieux on the help-seeking process for the milieu members themselves is discussed as a tendency. Due to the limitations of the study and the constraints of the concept itself, a causal argumentation is not supported.
Participants from the privileged milieu generally self-identify complaints as symptoms of mental illness less often, show less intention to seek help and have less than expected treatment experience. They are also less likely to seek help from a general practitioner or a family member. This is in line with research showing that previous steps of the help-seeking process are important for subsequent steps [13, 50, 71, 72]. Participants of this privileged milieu are people with mainly independent self-construal and even though they are well educated and belong to an upper income status group they do not seek help for their complaints. Two milieu-characteristics seem to be important here. First, the male proportion is higher than expected, which could explain the reduced help-seeking intention and behaviour [10]. Second, depression severity is lower than in the other milieux, which on the one hand could be because they are from higher SES groups and on the other hand more independently construed. Independent self-construal has been shown to buffer depression, mediated by higher self-efficacy [49]. The self-efficacy buffer hypothesis seems to be likely, seeing as the results indicated that participants from the more independent milieux are in general less depressed than the more interdependent milieux. However, when comparing the privileged milieu and the entitled milieu, participants from the entitled milieu show significantly more intention and help-seeking behaviour than participants from the privileged milieu, despite their similar SES and SCS profiles and demographic characteristic. One explanation is found when regarding the self-construal profiles more carefully (Table S5). There is a clear difference between the two milieux in the SCS dimensions “making decisions”, “communicating with others”, and “dealing with conflicting interests” in which the entitled milieu is more independent than the privileged milieu. Therefore, it is suggested that these SCS dimensions could be especially relevant when it comes to help-seeking intention and behaviour; an independent expression benefitting help-seeking. The actual behaviour and antecedent decision to seek help must come from the individual themselves, even if “others might not approve” or their behaviour is contrary to “other’s expectations” (wordings taken verbatim from the SCS items 3 and 41, Table S2).
An interesting finding is that participants from the more independent milieux, irrespective of SES, are less likely to self-identify their complaints as symptoms of a mental illness, which is most pronounced in the interdependent milieux. Possibly, this could be traced back to the interdependent construal of closely sharing self-related aspects within a familial setting whereby family members could reflect the complaints together with the individual and identify the complaints as symptoms of a mental illness. This seem to be especially pronounced in the collaborators milieu, in which participants are mainly interdependently construed and from middle and upper SES compared to the family bound milieu where the tendency is also more pronounced than in the mainly independent milieux but in which participants are from lower to middle SES than the collaborators. This interpretation holds when comparing help-seeking behaviour from a family member. Here, the more interdependent milieux are more likely to seek help than the more independent milieux. Even when comparing the milieux with similar SES profiles yet clearly contrary self-construal profiles, participants from the mainly interdependent milieux are more likely to seek help from family members. This is a good example for the necessity to not only regard SES as an explanans for differences in health-related behaviour, but also regard the self-construal of the person [41].
However, inconsistent with previous research regarding the help-seeking process [50, 52] the higher self-identifying tendency in the interdependent milieux does not support a higher intention to seek help or actual help seeking from a general practitioner. An obvious interpretation is that for participants from the mainly interdependent milieux further variables impact the help-seeking process in a stronger way than in the other milieux. This discrepancy is especially pronounced when comparing the collaborators and family bound milieux with the entitled milieu, in which participants show less severe depressive symptoms, lower self-identifying tendency and yet higher help-seeking intention and behaviour. This is one definite indicator that it is expedient to regard help-seekers differentially depending on their sociocultural background. For example, individuals from more independent milieux are supported more, when they are helped to identify their complaints as symptoms of mental illness, e.g., through mental health campaigns. On the other hand, individuals from more interdependent milieux, are more likely to find support when the peers and family members are shown the necessity and possibility to seek help from an out-group source, e.g., a general practitioner.
Strengths and limitations
There are some important strengths and limitations. A strength is the adaptability of the cluster methodology and the SES indexing procedure [56], meaning that the proposed methods could be easily used in different social and cultural environments. The novel framework also explains variances in help-seeking behaviour and could be used to develop intervention material aimed specifically for target groups who are less likely to seek professional help despite acknowledging their complaints as symptoms of a mental illness, i.e., more interdependently self-construed individuals. The sample was fitting to exemplarily test the Self-Milieux in empirical research, because participants reported symptoms of depression but were not in treatment at the beginning of the study. Due to the longitudinal design, actual help-seeking behaviour in the six-month period could be analysed.
Nevertheless, there are some important limitations. First and foremost, the data is based on self-reports which is inherently biased and does not represent actual help-seeking behaviour. Second, the sample was acquired using an online panel and has to be considered a convenience sample. Although the panel aims to be representative, there is likely a participation-selection bias, e.g., participants with high motivation to participate in online studies, participants with higher levels of education and income (as seen in this sample). Furthermore, it is unlikely that many individuals participated who are from very low SES backgrounds or ethnic minority groups. Therefore, a replication of the study would be interesting with data from a broader and more representative (German) sample as well as amongst hard to reach minority groups. Additionally, the differences between the six milieux might be impacted by the sample composition. Third, the impact of the milieux on the help-seeking process might primarily be attributed to self-construal profiles, as SES was introduced as a control variable in the regression analyses. This was done because SES is an established measure. Nevertheless, a novel framework must demonstrate the ability to add explanatory value to established concepts in order to be accepted. The findings provide support for the idea that the milieux go beyond the original constitutional variables in a Gestalt manner. Fourth, the study was conducted online during the COVID-19 pandemic, from January to September 2021, and even though research shows that online assessment doesn’t reduce attention levels [73] the online assessment will have had an impact on the external validity of the results. However, to counteract this issue, strict data control exclusion criteria were used before data analysis. Lastly, the self-construal items are usually not meant to be averaged into one score [31] which was done here to simplify visualisation (Fig. 1). However, internal consistency across all items is very good and because cluster centroids are reported, interpretation on a dimensional level was still possible.
Conclusions
This study attempts to combine findings from relative disparate research traditions and combine them into a novel Self-Milieux framework that goes beyond the separate determinants to explain health related help-seeking behaviour, both of a formal and an informal source. Participants from some milieux show a help-seeking process that has been proposed in previous research [13, 50] while other participants from more interdependent milieux show a different process, one that ends in informal help-seeking and is less influenced by self-identifying complaints as symptoms of a mental illness. Furthermore, these findings confirm the necessity to differentiate between similar SES groups when researching health related behaviour [41]. It is our conclusion, therefore, that understanding help-seeking in a milieux framework has practical relevance, because it should be useful in developing milieux-sensitive strategies to support individuals seeking (mental) health care. Possibly, such a campaign diversifying help-seeking strategies could counteract some troubling societal tendencies in which health related inequalities are becoming more and more prominent despite political and scientific efforts to counteract this inequality.
Data availability
The datasets generated during the current study is available from the corresponding author on reasonable request.
References
Lasalvia A, Zoppei S, van Bortel T et al (2013) Global pattern of experienced and anticipated discrimination reported by people with major depressive disorder: a cross-sectional survey. Lancet 381:55–62. https://doi.org/10.1016/S0140-6736(12)61379-8
Steel Z, Marnane C, Iranpour C et al (2014) The global prevalence of common mental disorders: a systematic review and meta-analysis 1980–2013. Int J Epidemiol 43:476–493. https://doi.org/10.1093/ije/dyu038
Wang PS, Aguilar-Gaxiola S, Alonso J et al (2007) Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet 370:841–850. https://doi.org/10.1016/s0140-6736(07)61414-7
Nübel J, Müllender S, Hapke U et al (2019) Epidemie der Depression?: Prävalenzentwicklung und Inanspruchnahme von Hilfs- und Versorgungsangeboten (Epidemic of depression?: Development of prevalence and help-seeking behaviour). Nervenarzt 90:1177–1186. https://doi.org/10.1007/s00115-019-0681-y
Robert Koch-Institut (2019) Inanspruchnahme psychiatrischer und psychotherapeutischer Leistungen—Individuelle Determinanten und regionale Unterschiede. RKI-Bib1 (Robert Koch-Institut)
Lopez AD, Murray CC (1998) The global burden of disease, 1990–2020. Nat Med 4:1241–1243. https://doi.org/10.1038/3218
Saxena S, Thornicroft G, Knapp M et al (2007) Resources for mental health: scarcity, inequity, and inefficiency. Lancet 370:878–889. https://doi.org/10.1016/S0140-6736(07)61239-2
Trautmann S, Rehm J, Wittchen H-U (2016) The economic costs of mental disorders: do our societies react appropriately to the burden of mental disorders? EMBO Rep 17:1245–1249. https://doi.org/10.15252/embr.201642951
Corrigan PW, Watson AC (2002) The paradox of self-stigma and mental illness. Clin Psychol Sci Pract 9:35–53. https://doi.org/10.1093/clipsy.9.1.35
von Eitzen L, Valerius K, van den Berg N et al (2021) Soziodemografische und störungsbezogene Determinanten zur Inanspruchnahme von ärztlicher oder psychologischer Hilfe bei depressiven Episoden in einem strukturschwachen Flächenland—die besondere Rolle des Lebensalters (Sociodemographic and Disorder-Specific Determinants for Professional Help-Seeking due to Depression in a Structurally Weak Region—The Important Role of Age). Psychiatr Prax 48:404–411. https://doi.org/10.1055/a-1468-3860
Jorm AF (2000) Mental health literacy. Public knowledge and beliefs about mental disorders. Br J Psychiatry 177:396–401. https://doi.org/10.1192/bjp.177.5.396
Pattyn E, Verhaeghe M, Sercu C et al (2014) Public stigma and self-stigma: differential association with attitudes toward formal and informal help seeking. Psychiatr Serv 65:232–238. https://doi.org/10.1176/appi.ps.201200561
Tomczyk S, Schmidt S, Muehlan H et al (2020) A prospective study on structural and attitudinal barriers to professional help-seeking for currently untreated mental health problems in the community. J Behav Health Serv Res 47:54–69. https://doi.org/10.1007/s11414-019-09662-8
Sallis J, Owen N, Fisher E (2008) Ecological models of health behavior. In: Glanz K (ed) Health behavior and health education: theory, research, and practice, 4th edn. Jossey-Bass, San Francisco, pp 465–485
Scott SE, Walter FM, Webster A et al (2013) The model of pathways to treatment: conceptualization and integration with existing theory. Br J Health Psychol 18:45–65. https://doi.org/10.1111/j.2044-8287.2012.02077.x
Lindbladh E, Lyttkens CH (2002) Habit versus choice: the process of decision-making in health-related behaviour. Soc Sci Med. https://doi.org/10.1016/S0277-9536(01)00180-0
Lindbladh E, Lyttkens CH, Hanson BS et al (1996) An economic and sociological interpretation of social differences in health-related behaviour: an encounter as a guide to social epidemiology. Soc Sci Med. https://doi.org/10.1016/S0277-9536(96)00087-1
Sewell WH (1992) A theory of structure: duality, agency, and transformation. Am J Sociol 98:1–29
Speerforck S, Schomerus G (2020) Soziale Milieus: Ein relevantes Konzept für ein besseres Verständnis von Stigma und psychiatrischer Unterversorgung? (Social milieu: a relevant concept for a better understanding of stigma and help-seeking?). Nervenarzt 91:785–791. https://doi.org/10.1007/s00115-020-00927-8
Diaz-Bone R (2003) Milieumodelle und Milieuinstrumente in der Marktforschung, Mannheim
Hradil S (2006) Soziale Milieus—eine praxisorientierte Forschungsperspektive. Aus Politik und Zeitgeschichte : APuZ 56:3–10
Markus HR, Kitayama S (1991) Culture and the self: implications for cognition, emotion, and motivation. Psychol Rev 98:224–253. https://doi.org/10.1037/0033-295X.98.2.224
Markus HR, Kitayama S (2010) Cultures and selves: a cycle of mutual constitution. Perspect Psychol Sci 5:420–430. https://doi.org/10.1177/1745691610375557
Stephens NM, Markus HR, Phillips LT (2014) Social class culture cycles: how three gateway contexts shape selves and fuel inequality. Annu Rev Psychol 65:611–634. https://doi.org/10.1146/annurev-psych-010213-115143
Masuda T, Ellsworth PC, Mesquita B et al (2008) Placing the face in context: cultural differences in the perception of facial emotion. J Pers Soc Psychol 94:365–381. https://doi.org/10.1037/0022-3514.94.3.365
Suh EM (2002) Culture, identity consistency, and subjective well-being. J Pers Soc Psychol 83:1378–1391. https://doi.org/10.1037/0022-3514.83.6.1378
Mesquita B (2001) Emotions in collectivist and individualist contexts. J Pers Soc Psychol 80:68–74. https://doi.org/10.1037/0022-3514.80.1.68
Tsai JL, Miao FF, Seppala E (2007) Good feelings in Christianity and Buddhism: religious differences in ideal affect. Pers Soc Psychol Bull 33:409–421. https://doi.org/10.1177/0146167206296107
Cross SE, Hardin EE, Gercek-Swing B (2011) The what, how, why, and where of self-construal. Pers Soc Psychol Rev 15:142–179. https://doi.org/10.1177/1088868310373752
Manstead ASR (2018) The psychology of social class: How socioeconomic status impacts thought, feelings, and behaviour. Br J Soc Psychol 57:267–291. https://doi.org/10.1111/bjso.12251
Vignoles VL, Owe E, Becker M et al (2016) Beyond the ‘east-west’ dichotomy: global variation in cultural models of selfhood. J Exp Psychol Gen. https://doi.org/10.1037/xge0000175
Feinstein JS (1993) The relationship between socioeconomic status and health: a review of the literature. Milbank Q 71:279. https://doi.org/10.2307/3350401
Galang CM, Johnson D, Obhi SS (2021) Exploring the relationship between empathy, self-construal style, and self-reported social distancing tendencies during the COVID-19 pandemic. Front Psychol 12:588934. https://doi.org/10.3389/fpsyg.2021.588934
Herd P, Goesling B, House JS (2007) Socioeconomic position and health: the differential effects of education versus income on the onset versus progression of health problems. J Health Soc Behav 48:223–238. https://doi.org/10.1177/002214650704800302
Huurre T, Eerola M, Rahkonen O et al (2007) Does social support affect the relationship between socioeconomic status and depression? A longitudinal study from adolescence to adulthood. J Affect Disord 100:55–64. https://doi.org/10.1016/j.jad.2006.09.019
Liu FF, Goto SG (2007) Self-construal, mental distress, and family relations: a mediated moderation analysis with Asian American adolescents. Cultur Divers Ethnic Minor Psychol 13:134–142. https://doi.org/10.1037/1099-9809.13.2.134
Marmot M, Ryff CD, Bumpass LL et al (1997) Social inequalities in health: next questions and converging evidence. Soc Sci Med 44:901–910. https://doi.org/10.1016/s0277-9536(96)00194-3
Phelan JC, Link BG, Diez-Roux A et al (2004) “Fundamental causes” of social inequalities in mortality: a test of the theory. J Health Soc Behav 45:265–285. https://doi.org/10.1177/002214650404500303
Steinkamp G (1999) Soziale Ungleichheit in Morbidität und Mortalität. Oder. Warum einige Menschen gesünder sind und länger leben als andere. In: Schlicht W DH-H (ed) Gesundheit für alle—Fiktion oder Realität. Schorndorf: Hofmann, pp 101–154
Jungbauer-Gans M, Gross C (2009) Erklärungsansätze sozial differenzierter Gesundheitschancen. In: Gesundheitliche Ungleichheit. VS, Verl. für Sozialwissenschaften, 2009, Wiesbaden, pp 77–98
Hradil S (2009) Was prägt das Krankheitsrisiko: Schicht, Lage, Lebensstil? In: Gesundheitliche Ungleichheit. VS, Verl. für Sozialwissenschaften, 2009, Wiesbaden, pp 35–54
Ostrove JM, Adler NE, Kuppermann M et al (2000) Objective and subjective assessments of socioeconomic status and their relationship to self-rated health in an ethnically diverse sample of pregnant women. Health Psychol 19:613–618. https://doi.org/10.1037/0278-6133.19.6.613
Baker EH (2014) Socioeconomic status, definition. In: Cockerham WC, Dingwall R, Quah S (eds) The Wiley Blackwell encyclopedia of health, illness, behavior, and society. Wiley, Chichester, pp 2210–2214
Singh-Manoux A, Marmot M (2005) Role of socialization in explaining social inequalities in health. Soc Sci Med 60:2129–2133. https://doi.org/10.1016/j.socscimed.2004.08.070
Kitayama S, Markus HR, Matsumoto H et al (1997) Individual and collective processes in the construction of the self: self-enhancement in the United States and self-criticism in Japan. J Pers Soc Psychol 72:1245–1267. https://doi.org/10.1037/0022-3514.72.6.1245
Markus HR, Wurf E (1987) The dynamic self-concept: a social psychological perspective. Annu Rev Psychol 38:299–337. https://doi.org/10.1146/annurev.ps.38.020187.001503
Angel RJ, Williams K (2013) Cultural Models of Health and Illness. Handbook of Multicultural Mental Health. Elsevier, Cham, pp 49–68
Shim G, Freund H, Stopsack M et al (2014) Acculturation, self-construal, mental and physical health: an explorative study of East Asian students in Germany. Int J Psychol 49:295–303. https://doi.org/10.1002/ijop.12008
Smith PB, Ahmad AH, Owe E et al (2016) Nation-level moderators of the extent to which self-efficacy and relationship harmony predict students’ depression and life satisfaction. J Cross Cult Psychol 47:818–834. https://doi.org/10.1177/0022022116648210
McLaren T, Peter L-J, Tomczyk S et al (2023) The seeking mental health care model: prediction of help-seeking for depressive symptoms by stigma and mental illness representations. BMC Public Health 23:69. https://doi.org/10.1186/s12889-022-14937-5
Schomerus G, Muehlan H, Auer C et al (2019) Validity and psychometric properties of the self-identification as having a mental illness scale (SELF-I) among currently untreated persons with mental health problems. Psychiatry Res 273:303–308. https://doi.org/10.1016/j.psychres.2019.01.054
Tomczyk S, Schomerus G, Stolzenburg S et al (2020) Ready, willing and able? An investigation of the theory of planned behaviour in help-seeking for a community sample with current untreated depressive symptoms. Prev Sci 21:749–760. https://doi.org/10.1007/s11121-020-01099-2
McLaren T, Peter LJ, Tomczyk S et al (2021) How can the utilisation of help for mental disorders be improved? A quasiexperimental online study on the changeability of stigmatising attitudes and intermediate variables in the process of utilisation. BMC Public Health 21:2124. https://doi.org/10.1186/s12889-021-12125-5
Kroenke K, Spitzer RL, Williams JB (2001) The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 16:606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Rössler P (2017) Kumulierte Evidenzen: Replikationsstudien in der empirischen Kommunikationsforschung. Springer Fachmedien Wiesbaden, Wiesbaden
Lampert T, Kroll LE, Müters S et al (2013) Messung des sozioökonomischen Status in der Studie “Gesundheit in Deutschland aktuell” (GEDA) (Measurement of the socioeconomic status within the German Health Update 2009 (GEDA)). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 56:131–143. https://doi.org/10.1007/s00103-012-1583-3
Schwartz S (2007) Value orientations: measurement, antecedents and consequences across nations. In: Jowell R (ed) Measuring attitudes cross-nationally: lessons from the European Social Survey, Reprinted. Sage, London, pp 161–193
Kroenke K, Spitzer RL, Williams JBW et al (2010) The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry 32:345–359. https://doi.org/10.1016/j.genhosppsych.2010.03.006
Pescosolido BA, Boyer CA (2010) Understanding the context and dynamic social processes of mental health treatment. In: Scheid TL, Brown TN (eds) A handbook for the study of mental health: social contexts, theories, and systems, 2nd edn. Cambridge University Press, Cambridge, pp 420–438
Milligan GW, Sokol LM (1980) A two-stage clustering algorithm with robust recovery characteristics. Educ Psychol Meas 40:755–759
Ward JH (1963) Hierarchical grouping to optimize an objective function. J Am Stat Assoc 58:236–244. https://doi.org/10.1080/01621459.1963.10500845
MacQueen J (1967) Some methods for classification and analysis of multivariate observations. In: Lecam L, Neyman J (eds) Proceedings of the fifth Berkeley symposium on mathematical statistics and probability, vol 1. University of California Press, Berkely, pp 281–297
R Core Team (2021) R: a language and environment for statistical, R Foundation for Statistical Computing, Vienna, Austria
Maechler M, Rousseeuw P, Struyf A et al. (2022) cluster: cluster analysis basics and extensions
Cohen J (1960) A coefficient of agreement for nominal scales. Educ Psychol Measur 20:37–46. https://doi.org/10.1177/001316446002000104
Dalmaijer ES, Nord CL, Astle DE (2022) Statistical power for cluster analysis. BMC Bioinform 23:205. https://doi.org/10.1186/s12859-022-04675-1
Sharpe D (2015) Chi-square test is statistically significant: now what? University of Massachusetts Amherst
Nagelkerke NJD (1991) A note on a general definition of the coefficient of determination. Biometrika 78:691. https://doi.org/10.2307/2337038
Faul F, Erdfelder E, Buchner A et al (2009) Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods 41:1149–1160. https://doi.org/10.3758/BRM.41.4.1149
Clatworthy J, Buick D, Hankins M et al (2005) The use and reporting of cluster analysis in health psychology: a review. Br J Health Psychol 10:329–358. https://doi.org/10.1348/135910705X25697
Schomerus G, Matschinger H, Angermeyer MC (2009) Attitudes that determine willingness to seek psychiatric help for depression: a representative population survey applying the Theory of Planned Behaviour. Psychol Med 39:1855–1865. https://doi.org/10.1017/S0033291709005832
Schomerus G, Auer C, Rhode D et al (2012) Personal stigma, problem appraisal and perceived need for professional help in currently untreated depressed persons. J Affect Disord 139:94–97. https://doi.org/10.1016/j.jad.2012.02.022
Clifford S, Jerit J (2014) Is there a cost to convenience? An experimental comparison of data quality in laboratory and online studies. J Exp Polit Sci 1:120–131. https://doi.org/10.1017/xps.2014.5
Acknowledgements
We would like to acknowledge our scientific assistant Jonathan Stellmacher, who aided substantially in the socioeconomic indexing procedure.
Funding
Open Access funding enabled and organized by Projekt DEAL. The data was acquired in a project funded by the DFG (German Research Foundation, www.dfg.de: SCHO 1337/4-2 and SCHM 2683/4-2). The DFG was not involved in the design of the study, the preparation, collection, analysis, and interpretation of data, or the writing of this article and deciding to submit it for publication. The project design was approved by external consultants of the DFG.
Author information
Authors and Affiliations
Contributions
TM and LJP contributed equally to the overall study design and the acquisition of the data. ST and HoM contributed to the conception of the work. GS and SiS manage the DFG funded project. The data was analysed and interpreted by TM. The manuscript was developed and drafted by TM. HoM, ST, LJP, GS, and SiS revised the draft. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
The study procedure was developed in accordance with the Declaration of Helsinki and has been approved by the Ethics Commission of the University Medicine Greifswald (BB 061/18) and Leipzig (514/19-lk).
Consent to participate
Participants included in the study gave electronic informed consent following comprehensive written information about the study. Participants gave electronic informed consent that results could be published anonymously.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
McLaren, T., Peter, LJ., Tomczyk, S. et al. A “Self-Milieux” perspective on help-seeking: examining the impact of a person’s sociocultural background on help-seeking in people with untreated depressive symptoms. Soc Psychiatry Psychiatr Epidemiol (2024). https://doi.org/10.1007/s00127-024-02720-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00127-024-02720-3