
Abstract
Aims/hypothesis
With the increase in gestational diabetes mellitus (GDM), there is a growing need to understand the effects of intrauterine glucose exposure on the newborn at birth and later in life. The risk of developing impaired glucose tolerance (IGT) in individuals exposed to diabetes in utero has not been adequately investigated.
Methods
We studied 255 obese adolescents with normal glucose tolerance. All of them were investigated for in utero exposure to GDM and underwent an OGTT, which was repeated after approximately 2.8 years.
Results
210 (82.3%) participants were not exposed to GDM (NGDM group), and 45 (17.7%) were exposed to GDM (EGDM group). In the NGDM group, only 8.6% (n = 18) developed either IGT or type 2 diabetes compared with 31.1% (n = 14) of the EGDM group who developed either IGT or type 2 diabetes (p < 0.001). Exposure to GDM was the most significant predictor of developing IGT or type 2 diabetes (OR 5.75, 95% CI 2.19, 15.07, p < 0.001). At baseline and at follow-up, the EGDM group showed a reduction in beta cell function determined by the oral disposition index (p = 0.03 and p = 0.01, respectively), and, at follow-up, they also displayed a reduction in insulin sensitivity compared with the NGDM group (p = 0.05).
Conclusions/interpretation
Obese youth exposed in utero to GDM show early inability of the beta cell to compensate adequately in response to decreasing levels of insulin sensitivity.
Similar content being viewed by others
Introduction
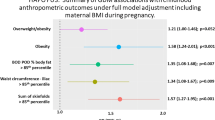
Over the past two decades, there has been a steady increase in the prevalence of type 2 diabetes [1] in parallel with the rising prevalence of obesity [2], which is the most important risk factor for paediatric development of type 2 diabetes [2, 3]. The SEARCH for Diabetes in Youth Study found that 3,600 youths were newly diagnosed annually. Type 2 diabetes was rare in children younger than 10 years, yet there was an increased prevalence in youths between 10 and 19 years of age [4]. One environmental factor that can drive this observation is intrauterine glucose exposure in the form of type 1 diabetes [5], type 2 diabetes [6] or gestational diabetes mellitus (GDM) [7]. Siblings born after exposure to diabetes in utero have a significantly greater BMI than those born to the same mothers before the diagnosis of maternal type 2 diabetes [8]. The HAPO Study examined neonatal outcomes of birthweight and cord C-peptide >90th percentile, primary Caesarean section and clinical hypoglycaemia. With the exception of hypoglycaemia, all other outcomes displayed an increasing linear relationship with maternal fasting glucose and 1 h and 2 h OGTT values [9].
Beyond perinatal effects, there are also long-term effects of intrauterine glucose exposure, which include an increase in obesity [10], cardiovascular risk factors [11] and glucose intolerance [7, 10]. At age 12 years, children born to mothers with pregestational or gestational diabetes have a 19.3% prevalence of impaired glucose tolerance (IGT), significantly greater than age- and sex-matched controls (2.5%) [7]. A relation has been shown between maternal glucose and offspring insulin sensitivity and beta cell response, independent of adiposity [12]. These observations suggest an increased risk of altered glucose metabolism in children exposed to hyperglycaemia in utero, yet the risks have not been quantified specifically for those exposed only to GDM.
The purpose of this study was to examine the risk in obese youths of developing IGT after exposure to GDM in utero. We hypothesised that prenatal exposure to GDM in obese children with normal glucose tolerance (NGT) would be associated with development of altered glucose metabolism over time, driven by an impairment of beta cell secretion relative to the insulin sensitivity.
Methods
All participants were recruited from the Yale Pathophysiology of Type 2 diabetes in Youth Study, a long-term, multiethnic study that aimed to investigate the early alternations in glucose metabolism in obese youth [13]. In this study, obese youth are followed longitudinally and OGTTs are repeated. The study was approved by the Human Investigations Committee of the Yale School of Medicine. Participants were eligible if they were healthy, between 4 and 20 years of age, and had a BMI that exceeded the 97th percentile for their age and sex [14]. An additional inclusion criterion was having NGT on the baseline OGTT. In addition to parental consent, complete medical histories and thorough physical examinations were obtained for each participant. Body composition was determined using the bioimpedance method (Tanita, TBF 300;Tanita Corp of America, Arlington Heights, IL, USA). All participants were negative at baseline for autoimmune markers of type 1 diabetes (insulin antibody, GAD65 and islet cell antibody 512).
For this study, data were analysed from 255 obese adolescents with a documented history of exposure/non-exposure to GDM in utero and NGT on the baseline OGTT. Exposure to GDM was based on the response to a validated questionnaire [15, 16], and the presence of GDM during the relevant offspring pregnancy was diagnosed by a glucose tolerance test. Women who responded ‘do not know’ were classified as negative for exposure.
The participants were separated into two groups on the basis of exposure history (NGDM, no exposure; EGDM, exposure). Participants were followed biannually as outpatients by the clinical staff and received nutritional guidance as well as recommendations for physical activity. Participants had an average follow-up period of 2.8 years between OGTTs.
OGTT
At 08:00 hours after a 10–12 h overnight fast, a standard OGTT (1.75 g/kg body weight, up to 75 g) was conducted to determine glucose tolerance [17]. Blood samples for determination of glucose, insulin and C-peptide were drawn at −15, 0, 30, 60, 90, 120 and 180 min. NGT was defined as a fasting glucose <5.55 mmol/l and a 2 h glucose <7.77 mmol/l. IGT was defined as a 2 h glucose of 7.77–11.05 mmol/l. Impaired fasting glucose (IFG) was defined as a fasting glucose of 5.55–6.88 mmol/l. Type 2 diabetes was defined as a fasting glucose >6.88 mmol/l or 2 h glucose >11.05 mmol/l [18].
Calculations derived from OGTT
The Matsuda index was used to calculate insulin sensitivity [19] (whole-body insulin sensitivity index [WBISI]). In addition, HOMA-IR [20] was calculated using the fasting sample as a surrogate of insulin resistance. The insulinogenic index (IGI) was defined by ∆ insulin (0–30, pmol/l)/∆ glucose (0–30, mmol/l), which is a surrogate measure of the acute insulin response [21]. We also calculated the oral disposition index (oDI) as the product of WBISI and IGI obtained during the OGTT [22]. The AUC for insulin and C-peptide was calculated using the trapezoidal rule.
Analytical methods
Plasma glucose was determined with a YSI 2700 Analyzer (Yellow Springs Instruments, Yellow Springs, OH, USA). Plasma insulin was measured with an RIA (Linco, St Charles, MO, USA), which has <1% cross-reactivity with C-peptide and proinsulin. Plasma C-peptide levels were measured using an RIA assay from Diagnostic Products (Los Angeles, CA, USA).
Statistical analysis
Data are presented as means ± SD. χ2 analysis was used to compare the dichotomous criteria of exposure to gestational diabetes and longitudinal glucose tolerance categories. Comparisons for continuous variables at baseline for both NGDM and EGDM participants were performed using a t test and ANCOVA with adjustment for age, sex, race, BMI z score and exposure to GDM. All delta values were calculated as the difference between follow-up and baseline continuous variables. Both delta (change) and baseline and longitudinal continuous variable comparisons for NGDM and EGDM were performed using a t test for related samples. Baseline and longitudinal WBISI, IGI and oDI were adjusted for sex, age, BMI z score and age at the time of evaluation by linear regression using the generalised linear model procedure [23]. A logistic regression analysis was performed to identify predictors of developing IGT/type 2 diabetes. The regression consisted of models comprising the independent variables of baseline age, sex, ethnicity, exposure to GDM, baseline BMI z score, baseline oDI, delta BMI z score and oDI percentage change. Statistical analyses were performed using SPSS (version 19.0 for Windows; SPSS, Chicago, IL, USA).
Results
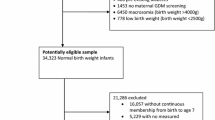
Of 255 participants, 82.3% (n = 210) were NGDM and 17.7% (n = 45) were EGDM. At baseline, all offspring in both groups had NGT as predefined. As shown in Fig. 1, within the NGDM group, 91.4% (n = 192) remained NGT at follow-up (non-progressors) and 8.6% (n = 18) developed either IGT or type 2 diabetes (progressors). In contrast, within the EGDM group, 68.9% (n = 31) remained NGT, while 31.1% (n = 14) developed either IGT or type 2 diabetes (p < 0.001; χ2 test). Of the NGDM group, 176 maintained normal fasting glucose, while 34 (16%) had IFG on follow-up. Of the EGDM group, 32 maintained normal fasting glucose and 13 (29%) developed IFG (p = 0.05; χ2 test). Importantly, 12 of the participants with IGT/type 2 diabetes on follow-up also had IFG.

Outline of study participants and follow-up. Transition from NGT to IGT/type 2 diabetes (T2D) was 31.1% vs 8.6% for EGDM and NGDM, respectively (p < 0.001; χ2 test)
Anthropometric and metabolic phenotypes at baseline and follow-up
Baseline anthropometrics and metabolic phenotypes (Table 1)
At baseline the two groups were similar with respect to age, sex, ethnicity distribution, BMI and BMI z score. Sex and ethnicity distribution between the groups were comparable. Although the BMI and BMI z score for the NGDM and EGDM groups were comparable, the EGDM group had a significantly lower adjusted fat mass than the NGDM group (p = 0.024). Importantly, birthweights were comparable between the groups despite the exposure to GDM in the EGDM group.
The fasting and 2 h plasma glucose levels were similar in the two groups (Table 1). AUC-glucose 120 in the EGDM group was significantly elevated (p = 0.05, adjusted p = 0.04). AUC-insulin 120, AUC-C-peptide 120 and HbA1c were similar in the two groups. The surrogate markers of insulin resistance/sensitivity (HOMA-IR and WBISI) and insulin secretion (IGI) were similar in the two groups. Of note, at baseline the EGDM group had a significantly lower oDI, suggesting a reduced beta cell response relative to the ambient insulin sensitivity (p = 0.006, adjusted p = 0.035).
Dynamics of anthropometric and metabolic parameters (Table 2)
Over a mean of 2.8 years of follow-up, both groups demonstrated a substantial yet comparable weight gain (17.56 ± 17.23 kg vs 23.15 ± 22.17 kg for NGDM and EGDM, respectively; p = 0.11). Of note, as these were growing adolescents, the weight gain was accompanied by an increase in height, thus the change in the degree of obesity (BMI z score) was similar between the groups (−0.04 ± 0.27 vs −0.031 ± 0.41 for NGDM and EGDM, respectively; p = 0.81). Despite similar weight dynamics, the EGDM group tended to have an increase in fasting plasma glucose (0.19 ± 0.57 mmol/l vs 0.06 ± 0.54 mmol/l for EGDM and NGDM respectively, p = 0.16) and 2 h glucose levels (0.10 ± 1.31 mmol/l vs 0.53 ± 1.57 mmol/l for NGDM and EGDM, respectively; p = 0.08) and had a significant rise in AUC-glucose 120 (0.60 ± 1.34 mmol/l × min vs 0.094 ± 1.05 mmol/l × min for EGDM and NGDM, respectively; p = 0.02).Thus the EGDM participants had significantly greater follow-up values of fasting, 2 h and AUC glucose than the NGDM participants (p = 0.01, p = 0.005 and p = 0.001, respectively). Both NGDM and EGDM groups had a similar HbA1c change from baseline, yet the follow-up value for the EGDM group was higher than that for the NGDM group (p = 0.04). Of note, the change and the follow-up values of AUC of insulin and C-peptide were comparable between the groups.
As shown in Fig. 2, the adjusted (for age at evaluation, sex, ethnicity and BMI z score) insulin sensitivity at baseline was similar in the two groups, while follow-up levels were significantly lower in the EGDM group (p = 0.05). The adjusted IGI remained similar at baseline and follow-up in the two groups. The adjusted oDI in the EGDM group was significantly lower at baseline (p = 0.03) and at follow-up (p = 0.01). On modelling the follow-up 2 h glucose value and adjusting for age, sex, race, baseline 2 h glucose, baseline and change in BMI z score and baseline and change in the oDI, we found that the EDGM group had a significantly greater 2 h glucose (p = 0.007).

Adjusted insulin sensitivity (a), IGI (b) and oDI (c) at baseline and follow-up. Black bars, EGDM group; white bars, NGDM group. Variables adjusted for sex, age, BMI z score and age at time of the evaluation. *p = 0.05; † p = 0.03; **p = 0.01. WBISI (insulin sensitivity) and oDI are presented in arbitrary units. The calculations for WBISI and oDI were performed using conventional units (mg/dl for glucose and μU/ml for insulin)
Risk of dysglycaemia progression
In a logistic regression with race, sex, age, baseline degree of obesity (BMI z score) and time of follow up as independent variables, the risk of developing IGT or type 2 diabetes in obese children with NGT at baseline was significantly associated with exposure to GDM (OR 5.75, 95% CI 2.19, 15.07, p < 0.001). Adding baseline oDI and the change in the degree of obesity over time resulted in similar results for in utero exposure to GDM, while baseline oDI (p = 0.015) and delta BMI z score (p = 0.027) emerged as significant predictors of development of IGT/type 2 diabetes as well. Thus, in both models, exposure to GDM was not only a highly significant predictor of worsening glucose metabolism, but also remained with a similar effect size despite adjustment for multiple relevant covariates. Within these models, age, sex, ethnicity and baseline BMI z score were non-significant predictors of glucose metabolism deterioration over time.
Discussion
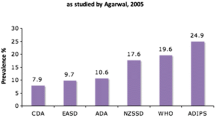
In this multiethnic cohort of obese adolescents, we found a 17.7% exposure rate to GDM, which is consistent with a contemporary rate of 18% reported by the International Association of Diabetes and Pregnancy Study Groups (IADPSG) [24, 25]. Alarmingly, 31.1% of obese children with NGT who were exposed to GDM in utero developed IGT/diabetes over a relatively short follow-up period of less than 3 years on average. Our results show that offspring of mothers who had gestational diabetes in pregnancy had at least a five times greater risk of developing IGT than those not exposed to gestational diabetes (OR >5 for all models tested). Although neither baseline insulin sensitivity nor baseline insulin secretion point to significant differences between the EGDM and NGDM groups, when we calculated the oDI, a difference between the groups emerged, indicating the presence of an inadequate compensation of beta cell response in the context of insulin resistance in offspring in the EGDM group.
Over time, EGDM participants showed a decrease in insulin sensitivity, irrespective of changes in adiposity. The significant decrease in insulin sensitivity without the ability to increase insulin secretion by the beta cells demonstrates this group’s inability to adequately compensate for a decrease in insulin sensitivity. The inability of EGDM offspring to increase insulin secretion over time is reflected in the significantly increased fasting glucose, 2 h glucose levels and 2 h AUC-glucose. A potential explanation for this deterioration in glycaemia over time in the EGDM offspring may be the reduced oDI, already present at baseline. The oDI has been shown to correlate reasonably well with a DI derived using ‘gold standard’ assessments of insulin sensitivity and secretion [26, 27]. In addition, this index has been shown to predict deterioration of glucose metabolism over time in adults and children [22, 28, 29]. It is thus not surprising that the baseline ~17% lower oDI in the EGDM group is associated with a greater deterioration in glucose metabolism over time. Our results are in agreement with those of Kelstrup et al [30] who followed non-obese offspring of mothers with GDM or type 1 diabetes mellitus into young adulthood and demonstrated a lower oDI in both populations compared with non-exposed controls. Our observations take this finding one step further and demonstrate the impact of such low oDI in children with additional risk factors (severe obesity) for diabetes development.
Numerous studies have found an increase in IGT in offspring exposed to GDM [7, 31]. While our findings are consistent with these studies, we provide novel functional defects that may explain the increased risk of developing IGT if exposed to GDM: a low oDI while glucose tolerance is normal, indicating the inability of the beta cell to compensate adequately in response to deterioration of ambient insulin sensitivity. We specifically chose to study obese children with baseline NGT and a comparable degree of glycaemia within the range of normal in order to eliminate baseline differences within the groups. A low baseline oDI is known to be predictive of development of diabetes over 10 years [32] in adults. Our results highlight a much faster progression towards IGT in EGDM obese offspring compared with that seen in adults.
The significantly elevated baseline AUC-glucose (p = 0.048) and the clinically relevant and nearly significant (p = 0.06) difference observed for the baseline 2 h glucose in the EGDM group (within the NGT range) may suggest defects in beta cell secretion, which have previously been observed in obese youths with high normal 2 h glucose [13]. As GDM is considered to be a prelude to later development of type 2 diabetes, it is possible that the genetic component of this risk is transmitted to the offspring independently of exposure to GDM in utero. Indeed, the heritability of the insulin secretion surrogates has been shown in non-diabetic relatives of patients with type 2 diabetes [33, 34]. The interaction of increasing 2 h glucose levels, within the normal range, with beta cell function and insulin sensitivity has also been examined, and it has been demonstrated that there is a significant decrease in insulin sensitivity and an absolute increase in insulin secretion as 2 h glucose increases [29]. This increase in insulin secretion is still not sufficient to normalise plasma glucose and reflects the inability of the beta cell to increase the early insulin response to blood glucose levels [29]. Thus, while slowly rising fasting and 2 h glucose levels seem to be a normal allostatic response to prevailing obesity-induced insulin resistance, the presence of exposure to GDM, along with additional type 2 diabetes-associated inherited genes, probably predisposes the beta cells of EGDM obese children to early failure [35].
Unlike the IADPSG study which showed an increase in birthweight due to exposure to GDM, our NGDM and EGDM cohorts had seemingly similar birthweights. This is probably because this study deals with severely obese children and adolescents with a high prevalence of obese parents. The familial obesity phenotype probably has an adverse synergistic effect on the metabolic markers we have shown in this study (such as reduced beta cell function), yet may mask the effects of isolated exposure to hyperglycaemia in utero on birthweight. Previous studies have shown increases in fat mass present in infants exposed to GDM, regardless of their weight for gestational age [36]. The fact that we demonstrate a lower amount of body fat mass in EGDM children who are severely obese already suggests that the impact of in utero hyperglycaemia on body composition may not only manifest at birth but also track into late childhood. As the presence of greater absolute obesity has been shown in offspring of GDM mothers [8, 37], it is reasonable to assume that the effect of exposure is manifested in body mass as well as body composition. As we have previously shown, lower body fat in the subcutaneous compartment may favour excessive lipid storage in insulin-responsive tissues, such as liver and muscle, and predispose to an adverse metabolic phenotype [38].
Potential limitations in our study include the self-reported history of maternal GDM data; however, the questionnaire used in this study has been validated and shown to have high sensitivity and specificity. The unknown time between maternal GDM diagnosis and birth does not allow us to factor in estimated exposure time, which could potentially reduce some of the adverse effects of increased glucose exposure. There are also no data on treatment after GDM diagnosis during pregnancy or the degree of metabolic control. One can speculate that exposure to poor metabolic control during pregnancy may have a stronger impact on indices of beta cell function in the offspring than exposure to strict glycaemic control. Furthermore, pre- or post-pregnancy BMI data for the mothers were not reliably recorded. This may serve as a surrogate of exposure to an additional obesity/diabetes genotype that was not accounted for in this analysis.
Strengths of the study are the repeated OGTT, along with body composition assessment and measures of insulin secretion and sensitivity, allowing a thorough evaluation of beta cell function in the context of the prevailing insulin sensitivity.
Implications
We demonstrate that obese NGT offspring of GDM mothers have pre-existing defects in beta cell function, as evidenced by a low oDI. The apparent low oDI is a strong risk factor for imminent progression towards IGT. The ever growing number of women with gestational diabetes (18%) suggests that the future will be filled with children with early diabetes at a rate that far exceeds the current prevalence. IADPSG criteria for diagnosing GDM [24] identify more cases of diabetes during pregnancy than the criteria used 10–15 years ago, yet quantification and characterisation of the metabolic risk of offspring based on the newly described criteria remain to be studied. Offspring of GDM mothers ought to be screened for IGT and/or IFG, and preventive and therapeutic strategies should be considered before the development of full clinical manifestation of diabetes. While we cannot use this analysis for development of definitive screening guidelines, we strongly suggest that, among obese children and adolescents exposed to GDM, specifically if additional risk factors are present (such as severe obesity, acanthosis nigricans, ethnic minorities, etc), OGTTs should be performed at baseline (specifically in mid-pubertal adolescents) and potentially repeated based on clinical judgement. Furthermore, the need for studies aimed at unravelling the role of genetic or epigenetic factors and environmental postnatal factors that might be causing functional defects in the beta cell has never been more urgent.
Abbreviations
- EGDM:
-
Exposed to gestational diabetes mellitus
- GDM:
-
Gestational diabetes mellitus
- IADPSG:
-
International Association of Diabetes and Pregnancy Study Groups
- IFG:
-
Impaired fasting glucose
- IGI:
-
Insulogenic index
- IGT:
-
Impaired glucose tolerance
- NGDM:
-
Not exposed to gestational diabetes mellitus
- NGT:
-
Normal glucose tolerance
- oDI:
-
Oral disposition index
- WBISI:
-
Whole-body insulin sensitivity index
References
Zimmet P, Alberti KG, Shaw J (2001) Global and societal implications of the diabetes epidemic. Nature 414:782–787
Arslanian S (2002) Type 2 diabetes in children: clinical aspects and risk factors. Horm Res 57(Suppl 1):19–28
Fagot-Campagna A, Pettitt DJ, Engelgau MM et al (2000) Type 2 diabetes among North American children and adolescents: an epidemiologic review and a public health perspective. J Pediatr 136:664–672
Dabelea D, Mayer-Davis EJ, Saydah S et al (2014) Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. JAMA 311:1778–1786
Sobngwi E, Boudou P, Mauvais-Jarvis F et al (2003) Effect of a diabetic environment in utero on predisposition to type 2 diabetes. Lancet 361:1861–1865
Pettitt DJ, Aleck KA, Baird HR, Carraher MJ, Bennett PH, Knowler WC (1988) Congenital susceptibility to NIDDM. Role of intrauterine environment. Diabetes 37:622–628
Silverman BL, Metzger BE, Cho NH, Loeb CA (1995) Impaired glucose tolerance in adolescent offspring of diabetic mothers. Relationship to fetal hyperinsulinism. Diabetes Care 18:611–617
Dabelea D, Hanson RL, Lindsay RS et al (2000) Intrauterine exposure to diabetes conveys risks for type 2 diabetes and obesity: a study of discordant sibships. Diabetes 49:2208–2211
HAPO Study Cooperative Research Group, Metzger BE, Lowe LP et al (2008) Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 358:1991–2002
Petitt DJ, Bennett PH, Knowler WC, Baird HR, Aleck KA (1985) Gestational diabetes mellitus and impaired glucose tolerance during pregnancy. Long-term effects on obesity and glucose tolerance in the offspring. Diabetes 34(Suppl 2):119–122
Tam WH, Ma RC, Yang X et al (2008) Glucose intolerance and cardiometabolic risk in children exposed to maternal gestational diabetes mellitus in utero. Pediatrics 122:1229–1234
Bush NC, Chandler-Laney PC, Rouse DJ, Granger WM, Oster RA, Gower BA (2011) Higher maternal gestational glucose concentration is associated with lower offspring insulin sensitivity and altered beta-cell function. J Clin Endocrinol Metab 96:E803–E809
Yeckel CW, Taksali SE, Dziura J et al (2005) The normal glucose tolerance continuum in obese youth: evidence for impairment in beta-cell function independent of insulin resistance. J Clin Endocrinol Metab 90:747–754
Kuczmarski RJ, Ogden CL, Grummer-Strawn LM et al (2000) CDC growth charts: United States. Adv Data 314:1–27
Gunderson EP, Lewis CE, Tsai AL et al (2007) A 20-year prospective study of childbearing and incidence of diabetes in young women, controlling for glycemia before conception: the Coronary Artery Risk Development in Young Adults (CARDIA) Study. Diabetes 56:2990–2996
Zeitler P, Hirst K, Pyle L et al (2012) A clinical trial to maintain glycemic control in youth with type 2 diabetes. N Engl J Med 366:2247–2256
Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (2003) Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 26(Suppl 1):S5–S20
American Diabetes Association (2004) Diagnosis and classification of diabetes mellitus. Diabetes Care 27(Suppl 1):S5–S10
Matsuda M, DeFronzo RA (1999) Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care 22:1462–1470
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419
Phillips DI, Clark PM, Hales CN, Osmond C (1994) Understanding oral glucose tolerance: comparison of glucose or insulin measurements during the oral glucose tolerance test with specific measurements of insulin resistance and insulin secretion. Diabet Med J 11:286–292
Weiss R, Cali AM, Dziura J, Burgert TS, Tamborlane WV, Caprio S (2007) Degree of obesity and glucose allostasis are major effectors of glucose tolerance dynamics in obese youth. Diabetes Care 30:1845–1850
Nelder JA, Wedderburn RWM (1972) Generalized linear models. JR Statist Soc A 135:370–384
Metzger BE, Gabbe SG, Persson B et al (2010) International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 33:676–682
International Association of Diabetes and Pregnancy Study Groups Consensus Panel, Metzger BE, Gabbe SG et al (2010) International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 33:676–682
Retnakaran R, Qi Y, Goran MI, Hamilton JK (2009) Evaluation of proposed oral disposition index measures in relation to the actual disposition index. Diabet Med 26:1198–1203
Sjaarda LG, Bacha F, Lee S, Tfayli H, Andreatta E, Arslanian S (2012) Oral disposition index in obese youth from normal to prediabetes to diabetes: relationship to clamp disposition index. J Pediatr 161:51–57
Lorenzo C, Wagenknecht LE, Rewers MJ et al (2010) Disposition index, glucose effectiveness, and conversion to type 2 diabetes: the Insulin Resistance Atherosclerosis Study (IRAS). Diabetes Care 33:2098–2103
Giannini C, Weiss R, Cali A et al (2012) Evidence for early defects in insulin sensitivity and secretion before the onset of glucose dysregulation in obese youths: a longitudinal study. Diabetes 61:606–614
Kelstrup L, Damm P, Mathiesen ER et al (2013) Insulin resistance and impaired pancreatic beta-cell function in adult offspring of women with diabetes in pregnancy. J Clin Endocrinol Metab 98:3793–3801
Malcolm JC, Lawson ML, Gaboury I, Lough G, Keely E (2006) Glucose tolerance of offspring of mother with gestational diabetes mellitus in a low-risk population. Diabet Med 23:565–570
DeFronzo RA, Abdul-Ghani MA (2009) Oral disposition index predicts the development of future diabetes above and beyond fasting and 2-h glucose levels: response to Utzschneider et al. Diabetes Care 32:e86, author reply e87
Elbein SC, Sun J, Scroggin E, Teng K, Hasstedt SJ (2001) Role of common sequence variants in insulin secretion in familial type 2 diabetic kindreds: the sulfonylurea receptor, glucokinase, and hepatocyte nuclear factor 1alpha genes. Diabetes Care 24:472–478
Gjesing AP, Hornbak M, Allin KH et al (2014) High heritability and genetic correlation of intravenous glucose- and tolbutamide-induced insulin secretion among non-diabetic family members of type 2 diabetic patients. Diabetologia 57:1173–1181
Nolan CJ, Damm P, Prentki M (2011) Type 2 diabetes across generations: from pathophysiology to prevention and management. Lancet 378:169–181
Lingwood BE, Henry AM, d'Emden MC et al (2011) Determinants of body fat in infants of women with gestational diabetes mellitus differ with fetal sex. Diabetes Care 34:2581–2585
Pettitt DJ, Baird HR, Aleck KA, Bennett PH, Knowler WC (1983) Excessive obesity in offspring of Pima Indian women with diabetes during pregnancy. N Engl J Med 308:242–245
Weiss R, Dufour S, Taksali SE et al (2003) Prediabetes in obese youth: a syndrome of impaired glucose tolerance, severe insulin resistance, and altered myocellular and abdominal fat partitioning. Lancet 362:951–957
Acknowledgements
The authors are grateful to the patients and their families as well as to the Hospital Research Unit (HRU) personnel.
Funding
CG is funded by the European Society of Pediatric Endocrinology (ESPE Long-Term Research Fellowship 2011), NS is funded by the American Heart Association (AHA) (13SDG14640038), RW is funded by the Stephen Morse Diabetes Research Foundation, SC is funded by the National Institutes of Health (NIH) (grants R01-HD-40787, R01-HD-28016) and ADA (Distinguished Clinical Scientist Awards from the American Diabetes Association, DK-49230). This work was also made possible by the CTSA Grant Number UL1 RR024139 from the National Center for Advancing Translational Science (NCATS) and by DK045735 to the Yale Diabetes Endocrinology Research Center, a component of the NIH, and NIH roadmap for Medical Research. The contents of this scientific contribution are solely the responsibility of the authors and do not necessarily represent the official view of NIH.
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
TH: collected data, analysed the data and wrote the manuscript. CG and NS: collected data, analysed the data and reviewed the manuscript. BP, MS and ED: collected data, took part in clinical care and provided critical inputs to the text. SC and RW: designed the study, collected and analysed the data, and wrote the manuscript. All authors approved the manuscript in its final version. SC is the guarantor.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Holder, T., Giannini, C., Santoro, N. et al. A low disposition index in adolescent offspring of mothers with gestational diabetes: a risk marker for the development of impaired glucose tolerance in youth. Diabetologia 57, 2413–2420 (2014). https://doi.org/10.1007/s00125-014-3345-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-014-3345-2