
Abstract
Purpose
In the last 20 years, the number of fatalities due to road traffic accidents (RTA) in Germany has steadily decreased from 7503 to 2724 per year. Due to legal regulations, educational measures and the continuous development of safety technology the number of severe traumatic injuries and injury patterns are most likely to change. The aim of the study was to analyse severely injured motorcyclists (MC) and car occupants (CO) that were involved in RTAs in the last 15 years and investigate the development and changes of injury patterns, injury severity and hospital mortality.
Methods
We retrospectively evaluated data from the TraumaRegister DGU® (TR-DGU) considering all RTA-related injured MCs and COs (n = 19,225) that were registered in the TR-DGU from 2006 to 2020 with a primary admission to a trauma center with continuous participation (14 of 15 years) in the TR-DGU, an Injury Severity Score (ISS) ≥ 16 and aged between 16 and 79 years. The observation period was divided into three 5-year interval subgroups for further analysis.
Results
The mean age increased by 6.9 years and the ratio of severely injured MCs to COs changed from 1:1.92 to 1:1.45. COs were in 65.8% male and more often severely injured in the age groups under 30, while the majority of severely injured MCs were in the age group around 50 years and in 90.1% male.
The ISS (− 3.1 points) as well as the mortality of both groups (CO: 14.4% vs. 11.8%; MC: 13.2% vs. 10.2%) steadily decreased over time. Nevertheless, the standardized mortality ratio (SMR) hardly changed and stayed < 1. Regarding the injury patterns, the greatest decline of injuries with AIS 3 + were to the head (CO: − 11.3%; MC: − 7.1%), in addition, a decrease of injuries to extremities (CO: − 1.5%; MC: − 3.3%), to the abdomen (CO: − 2.6%; MC: − 3.6%), to the pelvis in COs (− 4.7%) and to the spine (CO: + 0.1%; MC: − 2.4%) were observed. Thoracic injuries increased in both groups (CO: + 1.6%; MC: + 3.2%) and, furthermore, pelvic injuries in MCs (+ 1.7%). Another finding was the increase of the utilization of whole body CTs from 76.6 to 95.15%.
Conclusion
The severity of injuries and their incidence, especially head injuries, have decreased over the years and seem to contribute to a decreasing hospital mortality of polytraumatized MCs and COs injured in traffic accidents.
Young drivers and an increasing number of seniors are the age groups at risk and require special attention and treatment.
Similar content being viewed by others


Introduction
According to the World Health Organization`s (WHO) Global Status Report On Road Safety 2018 (GSRORS 2018), about 1.35 million people from 175 different countries died in 2016 due to road traffic accidents (RTA), moreover, additional 20–50 million suffer yearly from non-fatal injuries. RTAs are worldwide the 8th leading cause of deaths in all age groups and the number one cause of death for the age group 5–29 years [1, 2]. In high-income countries, fatalities are more predominant with motorized vehicle users, whereas pedestrians and cyclists account for more than half of deaths in low-income countries [1, 3].
In Germany, which is considered a high-income country, the number of road traffic accidents (RTA) and RTA-related fatalities dropped in 2020 to its lowest level in more than 60 years. During the time period from 2000 to 2020, the number of fatalities caused by RTAs has decreased by about two thirds, from 7503 to 2719 per year [4]. It has to be mentioned that due to the COVID-19 pandemic situation with several lockdowns, home schooling and home-office in 2020 the number of travelled kilometers decreased in Germany [5].
The German police records about 6,135 RTAs, almost 900 injured road users and more than 7 fatalities per day. The 2020 RTA analysis of the German Federal Statistical Office has revealed that car occupants and motorcyclists, including scooter drivers with a registered license plate, make up the vast majority of RTA-related fatalities with 63.4% (car occupants 43% and motorized two-wheelers 18.4%) [4].
Former studies from different countries already showed in 1992 and in 2015/2016 that the majority of injuries due to motorized RTAs were to head, neck and thorax sustaining about 72% of all injuries in all age groups [6, 7]. There is scarce analysis of injury patterns for polytraumatized RTA victims in Germany before 2006 to compare to our study as data was limited.
Nevertheless, the number of RTAs, severity of injuries and hospital mortality are most likely to decrease due to the implementation of legal regulations, the establishment and implementation of guidelines for trauma management of severely injured and the continuous development of active and passive safety technology systems [8, 9]. Furthermore, the advance of safety technology could have changed the energy impact on different body regions and thereby could have effected injury severity and patterns. Analyzing injury patterns is crucial for prevention efforts and interventions. Reducing the number of RTA-related injuries, the severity of injury patterns and eventually fatalities is an important issue.
The aim of the study is to analyze and compare possible changes in injury patterns, injury severity and in-hospital mortality rates for motorized two-wheelers and car occupants which were recorded in the TraumaRegister DGU® over a time period of 15 years. Our hypothesis is that the injury profile as well as injury severity have changed over time. The identification of changed injury patterns could be useful for pre-hospital trauma teams, in-hospital trauma teams and safety experts.
Methods
The study was designed as a retrospective, cross-sectional, multi-center study analyzing data submitted to the TraumaRegister DGU® in the time period from 2006 to 2020.
TraumaRegister DGU®
The TraumaRegister DGU® of the German Trauma Society (Deutsche Gesellschaft für Unfallchirurgie, DGU) was founded in 1993. The aim of this multicenter database is a pseudonymized and standardized documentation of severely injured patients.
Data are collected prospectively in four consecutive time phases from the site of the accident until discharge from hospital: (A) pre-hospital phase, (B) emergency room and initial surgery, (C) intensive care unit and (D) discharge.
The documentation includes detailed information on demographics, injury pattern, comorbidities, pre- and in-hospital management, course on intensive care unit, relevant laboratory findings including data on transfusion and outcome of each individual. The inclusion criterion is admission to hospital via emergency room with subsequent ICU/ICM care or reach the hospital with vital signs and die before admission to ICU.
The infrastructure for documentation, data management, and data analysis is provided by AUC—Academy for Trauma Surgery (AUC—Akademie der Unfallchirurgie GmbH), a company affiliated to the German Trauma Society. The scientific leadership is provided by the Committee on Emergency Medicine, Intensive Care and Trauma Management (Sektion NIS) of the German Trauma Society. The participating hospitals submit their data pseudonymized into a central database via a web-based application. Scientific data analysis is approved according to a peer review procedure laid down in the publication guideline of TraumaRegister DGU®.
The participating hospitals are primarily located in Germany (90%), but a rising number of hospitals in other countries contribute data as well (at the moment from Austria, Belgium, China, Finland, Luxembourg, Slovenia, Switzerland, The Netherlands, and the United Arab Emirates). Currently, almost 30,000 cases from almost 700 hospitals are entered into the database per year.
Participation in TR-DGU is voluntary. For hospitals associated with TraumaNetzwerk DGU®, however, the entry of at least a basic data set is obligatory for reasons of quality assurance.
The present study is in accordance with the publication guidelines of the TraumaRegister DGU® and registered as TR-DGU project ID 2021–014.
Study sample and statistical analysis
Included and excluded data are depicted in the flowchart (Fig. 1).

Flow chart demonstrating included and excluded data from the TraumaRegister DGU® from 2006 to 2020
We analyzed data that was submitted to the TraumaRegister DGU® of patients involved in traffic accidents as motorcyclists or car occupants between January 1st 2006 and December 31st 2020. Inclusion criteria were a primary admission to Trauma Center (TC) in Germany, Austria or Switzerland with a “continuous” participation in the TR-DGU. A participation was defined as “continuous” if the TC submitted data in at least 14 out of 15 years in the investigated time period. Further criteria were an Injury Severity Score (ISS) ≥ 16 and the age group 16 to 79.
Statistical analysis was performed with SPSS statistical software (Version 26, IBM Inc., Armonk NY, USA). Categorical variables are presented as percentages and metric data is presented as mean with standard deviation (SD). Formal statistical testing was avoided due to the huge sample size. Even differences of less than 1% would formally become statistically significant although being irrelevant.
11,917 car occupants and 7,208 motorcyclists were each divided into three 5-year interval subgroups (2006–2010, 2011–2015 and 2016–2020) and compared regarding age, sex, ISS, serious injuries with Abbreviated Injury Scale (AIS) 3 + to head, thorax, abdomen, and extremities/pelvic, initiated whole-body CT (WBCT), hospital mortality during inpatient stay and standardized mortality ratio. Furthermore, the frequency of injuries (AIS 3 +) to head, chest, abdomen and extremities over time were depicted graphically.
Results
Basic data
19,125 severely injured car occupants (11,917; 62.3%) and motorcyclists (7,208; 37.7%) matched the inclusion criteria and were filtered from 81 Trauma Centers (TC). 69.2% derived from 56 super-regional TCs, 24.7% from 20 regional TCs and 6.1% from 5 local TCs. On average, we included 1275 admissions per year.
In the investigated period, the severely injured motorcyclist (MC) to car occupant (CO) ratio decreased steadily from 1:1.92 in 2006–10 to 1:1.45 in 2016–20. The rate of males in the group of injured COs was on average 65.8% compared to 90.1% in the MC group. The overall mean age continuously increased from 36.9 years in 2006 to 43.8 years in 2020.
Serious injured COs and MCs are often noted in the younger ages around 20 years and MCs additional in the age group around 50 years.
ISS, hospital mortality and SMR
The average ISS decreased by a total of three points over 15 years, from 30.7 in 2006 to 27.6 in 2020. In addition, a decrease of overall hospital mortality was observed. Regarding the CO group mortality decreased from 14.4% (2006–10) to 11.8% (2016–20) and in the MC group from 13.2% (2006–10) to 10.2% (2016–20). The calculated SMRs for all groups and time intervals showed values < 1 with minor fluctuation (Table 1).
Injury patterns
The graphical overview (Fig. 2) illustrates the chronological development of severe injuries with AIS 3 + in the body regions head, thorax, abdomen and pelvis with extremities for both investigated groups.

Development of severe injuries with AIS 3 + to head, thorax, abdomen and extremities and pelvis for car occupants (CO) and motorcyclists (MC) from 2006 to 2020
A closer look at the different injury regions (Table 1) shows the greatest decrease of AIS 3 + injuries to the head. Head injuries decreased by 14.3%, from 46.9% in the subgroup 2006–10 to 35.6% in 2016–20, in the CO group. Similar findings were detected for MCs, where a decrease of 7.1% (38% in 2006–10 vs. 30.9% in 2016–20) was observed.
Further analysis showed a decrease of serious injuries to the abdomen, spine and extremities.
Abdominal injuries declined by 2.6% (22.5% in 2006–10 vs. 19.9% in 2016–20) in the CO group and by 3.6% in the MC group (21.8% in 2006–10 vs. 18.2% in 2016–20).
The incidence of extremity injuries dropped in the CO group by 1.5% (33.8% in 2006–10 vs. 32.3% in 2016–20) and by 3.3% (38.7% in 2006–10 vs. 35.4% in 2016–20) within the MC group. Spine injuries hardly changed in the CO group (+ 0.1%), but decreased in the MC group by 2.4% (17.3% in 2006–10 vs. 14.9% in 2016–20). Injuries to the pelvis decreased by 4.7% in the CO group and increased by 1.7% in the MC group.
Furthermore, an increase of severe injuries to the thorax was detected in both groups. Regarding COs, thoracal injuries increased by 1.6%, from 68.9% in 2006–10 to 70.5% in 2016–20, and for the MCs by 3.6% (66.3% in 2006–10 vs. 69.9% 2016–20).
Whole-body CT (WBCT)
An additional observation is the enormous increase of WBCT over time. In the investigated groups, WBCT rates are 95.15% (95.6% CO and 94.7% MC) in 2016–2020 versus 76.6% (77.4% CO and 75.8% MC) in 2006–2010.
Discussion
There are several studies analyzing road traffic accidents in European and non-European countries. As there are local differences regarding traffic regulations, distribution of road users, road quality and vehicle standards, a comparison of the studies is not effective. With the TraumaRegister DGU®, we have a local database that enables statistically valuable analyses with large case numbers over time.
The key findings of this study are a reduced injury severity and overall hospital mortality rate with a minor shift of injury patterns for car occupants and motorcyclists involved in RTAs. Secondly, we observed severely injured motorcyclists and car occupants more often in the age group around 20 years and motorcyclists, additionally, in the age group around 50 years while the mean age steadily increased over the analyzed time period. Besides, the whole-body CT utilization increased from 75 to 95% from 2006 to 2020.
The number of road traffic accidents in Germany has been decreasing for years. Comparing the years from 2006 to 2020, RTAs with personal injury decreased from 327,984 to 264,499 and RTA-related deaths dropped from 5091 to 2719 [10]. According to our findings, severe traumatic injuries (depicted as ISS) and overall mortality likewise decreased continuously in the last fifteen years (see Fig. 3). We assumed that, most likely, severity and mortality decreased due to multiple reasons including legal regulations, improvement of safety gear, vehicle technology and an optimization of pre- and in-hospital treatment of polytraumatized patients throughout the past decades [4, 11], but the SMR calculation showed no comparable development in contrast to the pure mortality values.
In 2018, Germany ranked 11th place in an international comparison of road fatalities per 10,000 registered motorized vehicles of 36 countries. 50% of the participating countries reduced their fatality rate by more than two thirds between 2000 and 2018. The leading countries with the lowest mortality rates were Norway, Switzerland, Japan and the United Kingdom. Germany is ranked in the upper midfield—there is a continuous process to achieve this goal, nevertheless, an analysis and comparison to Norway and Switzerland could be useful to reduce our mortality rate even more [12].
Our findings showed a great decrease of severe head injuries for car occupants (− 14.3%) and motorcyclists (− 7.1%). The mortality of traumatic brain injuries (TBI) has declined over years, nevertheless, mortality rate for TBI is still about 30–40% [13]. The reduction of severe head injuries in our investigated subgroups could have had the greatest effect on the yearly mortality reduction in our study. Certainly, severe extremity and pelvic injuries and, especially, abdominal injuries with internal bleeding have impact on mortality too and their decrease in our findings should not be neglected. Despite, traumatic head injuries are the number one cause of death with cardio-respiratory failure after RTAs [14].
A further finding is the increase of thoracic injuries in both study groups (+ 1.6% COs, + 3.6% MCs). Surprisingly, the incidence of severe thoracic injuries is about the same for COs as for MCs and represent the highest incidence (~ 70%) of all injuries in our investigated population (Table 1). A few studies have shown that thoracic injuries significantly contribute to the mortality of polytrauma patients [15,16,17] and with the greatest focus on preventing severe head injuries, the problem of thoracic injuries are rarely addressed [18]. The slight increase of thoracic injuries in our findings could be explained through the demographic shift in German society. Brockamp et al. [19] observed that the amount of severe injuries to the thorax increases with age. The mean age of severely injured increased in our analysis by 6.9 years. The German Federal Statistical Office analyzed that inhabitants aged over 67 years increased by 54% from 1990 to 2018 in Germany and the Office estimates an increase by another 9% from 2019 to 2040 [20], subsequently, it could be estimated that thoracic injuries could increase even more.
Another reason could be the increasing utilization of WBCT (75–95%). The increasing number of CT-Traumascans during the study period might have led to a more thorough diagnosis of chest injuries. An explicit cause for the overall increase of thoracic injuries or the increase of pelvic injuries in the MC group cannot be derived from this study—this requires a more in-depth analysis.
Concerning CT-Traumascans, Caputo et al. [21] confirmed the findings of Huber-Wagner et al. [22] and demonstrated in a meta-analysis with 25,782 trauma patients who received CT scan following trauma that in terms of overall mortality WBCT scan is preferable to selective scanning. In our study population, we analysed RTA-related polytraumatized COs and MCs—it is very likely that WBCT has made a contribution to the hospital mortality reduction as the probability to overlook injuries is thereby reduced. The standard utilization of WBCTs for suspected severely injured trauma patients is an ongoing scientific debate.

Hospital mortality and ISS in the investigated years from 2006 to 2020
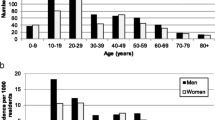
Figure 4 depicts the age distribution of severely injured COs and MCs and, furthermore, the ratio of severely injured COs per one MC. In our study population, the most COs are in the age group under 30 years and the majority of MCs are severely injured in the age group around 50 years. The age distribution of the MCs could be explained by the overall distribution of motorbike users in Germany. 79.4% of all MCs are aged between 30 and 59 years, when adding the age group 60–69 years the percentage increases to 90.8% [23]. Considering the bottom graphic of Fig. 4, severely injured COs are significantly more often represented in all age groups, especially, in the age groups over 60 years.

Percentage age distribution in the car occupant (CO) and motorcycle group (MC) and ratio of CO and MC patients presented as number of seriously injured COs per one MC patient
However, an age peak around 18–20 years can be observed in the MC and CO group. The peaks could be explained by the classic inexperienced drivers overestimating their driving skills with lack of risk-awareness and lack of foresighted driving. Youth-related lifestyles also include driving without helmets, speeding, using mobile phones while driving or even drinking and driving—a well-known and already addressed issue [24].
The 2020 international road safety report demonstrated that the overall number of young people killed in road traffic crashes had declined since 2010. But in the vast majority of countries, the age group 18–20 still had an above average mortality rate in 2018. In some countries like Switzerland, Belgium or Portugal, the young population is now less at risk than the general population, especially, less than senior citizens with 75 + years who showed a higher risk in 2018. In Germany the positive effect could not be observed, the 18–20 year old’s are still the second leading group at high risk, after the 75 + year old’s [12]. Multiple former studies demonstrated that geriatric trauma patients (75 +) are at high risk and associated with increased rate of severe injuries, higher mortality rates and are often undertriaged [25,26,27,28,29].
Limitations and methodological strength
By using the TraumaRegister DGU® for our retrospective multicenter study, it was only possible to include hospitalized patients that were presented in the emergency trauma rooms. Thus, we are missing data from fatalities occurring at RTA scenes or in the ambulance. It has to be noted that not all ISS ≥ 16 from the TR are included as we used specific filters to match our inclusion criteria. Furthermore, data from early years are not always complete as the TR-DGU is continuously in development.
To simplify the analysis we divided the time period into three subgroups with 5-year intervals. To get a more specific analysis, each year could have been analysed separately and statistical outliers could have been diminished. This might be a further limitation in our dataset. In addition, we cannot differentiate between car drivers or car occupants.
It cannot be neglected that due to the COVID-19 pandemic situation with lockdown, homeschooling and home-office, the number of travelled kilometers decreased extremely [5] and, therefore, the number of RTAs in 2020 decreased even more.
Our inclusion criteria with the continuously participation and about 94% of super-regional and regional TCs with over 1100 entries yearly (except 2006) makes the large data set objectively comparable over a long time period.
We are analysing polytraumatized victims (ISS > 15)—this study is representative for all hospitals with a high standard of trauma management in Germany, victims that are brought to a non-TC hospital are not included and not comparable.
Conclusion
The incidence of serious injuries, as well as the severity of injuries, especially head injuries, have decreased over the years and seem to contribute to the decreasing mortality in Germany.
Even though mortality is decreasing, the demographic shift and an increasing life expectancy associated with an increasing mobility of older people and new mobility forms such as E-scooters or E-bikes, we will be facing new challenges. Young drivers and an increasing number of seniors remain the age groups at risk and require special attention, diagnostic and treatment. Despite the continuously increasing average age, the long-term goal of the EU is to reduce the number of road deaths to almost zero by 2050 ("Vision Zero") [30].
Availability of data and materials
The dataset generated and analyzed during the current study is not publicly accessible.
References
World Health Organization (2022) Global status report on road safety 2018. Geneva: World Health Organization, 2018. Zugegriffen: 16. Januar 2022. [Online]. Verfügbar unter: https://apps.who.int/iris/handle/10665/276462
World Health Organization (2022) Global status report on road safety: time for action. Geneva, World Health Organization, Bd. 93. WGO, 2009. Zugegriffen: 16. Januar 2022. [Online]. Verfügbar unter: https://apps.who.int/iris/handle/10665/271751
Naci H, Chisholm D, Baker TD. Distribution of road traffic deaths by road user group: a global comparison. Inj Prev J Int Soc Child Adolesc Inj Prev. 2009;15(1):55–9. https://doi.org/10.1136/ip.2008.018721.
Verkehr-Verkehrsunfälle, Statistisches Bundesamt (Destatis), Wiesbaden, Press release Fachserie 8 Reihe 7 .Nr. 321, Juli 2021. Zugegriffen: 16. Januar 2022. [Online]. Verfügbar unter: https://www.destatis.de/DE/Presse/Pressemitteilungen/2021/07/PD21_321_46241.html
Verkehr in Deutschland - Fahrleistung von Pkw bis 2020, Statista. https://de.statista.com/statistik/daten/studie/2984/umfrage/entwicklung-der-fahrleistung-von-pkw/. zugegriffen 23. Mai 2022
Bradbury A, Robertson C. Prospective audit of the pattern, severity and circumstances of injury sustained by vehicle occupants as a result of road traffic accidents. Emerg Med J. 1993;10(1):15–23. https://doi.org/10.1136/emj.10.1.15.
Leijdesdorff HA, Gillissen S, Schipper IB, Krijnen P. Injury pattern and injury severity of in-hospital deceased road traffic accident victims in The Netherlands: Dutch Road traffic accidents fatalities. World J Surg. 2020;44(5):1470–7. https://doi.org/10.1007/s00268-019-05348-6.
Lubbe N, Jeppsson H, Ranjbar A, Fredriksson J, Bärgman J, Östling M (2018) Predicted road traffic fatalities in Germany: the potential and limitations of vehicle safety technologies from passive safety to highly automated driving, p 36
S3–Leitlinie Polytrauma/Schwerverletzten-Behandlung“. Deutsche Gesellschaft für Unfallchirurgie (DGU), 2016
Verkehrsunfälle - Zeitreihen (2019), p. 250, 2020.
Östling M, Lubbe N, Jeppsson H, Puthan P Passenger car safety beyond ADAS: defining remaining accident configurations as future priorities, S. 20
International Traffic Safety Data and Analysis Group, ROAD SAFETY ANNUAL REPORT (2020) OECD/International transport forum
Rosenfeld JV, Maas AI, Bragge P, Morganti-Kossmann MC, Manley GT, Gruen RL. Early management of severe traumatic brain injury. Lancet Lond Engl. 2012;380(9847):1088–98. https://doi.org/10.1016/S0140-6736(12)60864-2.
Ahmed A. A retrospective analysis of the pattern and severity of injuries in victims of road traffic accidents in Karachi, Pakistan during 2010–2011. Emerg Med Open Access. 2013. https://doi.org/10.4172/2165-7548.1000144.
Bayer J. Thoracic trauma severity contributes to differences in intensive care therapy and mortality of severely injured patients: analysis based on the TraumaRegister DGU®. World J Emerg Surg WJES. 2017;12:43. https://doi.org/10.1186/s13017-017-0154-1.
Ostermann RC. Thoracic injuries in pediatric polytraumatized patients: epidemiology, treatment and outcome. Injury. 2021;52(6):1316–20. https://doi.org/10.1016/j.injury.2021.02.033.
Chrysou K, Halat G, Hoksch B, Schmid RA, Kocher GJ. Lessons from a large trauma center: impact of blunt chest trauma in polytrauma patients—still a relevant problem? Scand J Trauma Resusc Emerg Med. 2017;25(1):42. https://doi.org/10.1186/s13049-017-0384-y.
Bambach MR, Mitchell RJ. The rising burden of serious thoracic trauma sustained by motorcyclists in road traffic crashes. Accid Anal Prev. 2014;62:248–58. https://doi.org/10.1016/j.aap.2013.10.009.
Brockamp T. Comparison of transportation related injury mechanisms and outcome of young road users and adult road users, a retrospective analysis on 24,373 patients derived from the TraumaRegister DGU®. Scand J Trauma Resusc Emerg Med. 2017. https://doi.org/10.1186/s13049-017-0401-1.
Statistisches Bundesamt Wiesbaden (2019) Bevölkerung im Wandel; Statistisches Bundesamt Wiesbaden: Wiesbaden, Germany
Caputo ND, Stahmer C, Lim G, Shah K. Whole-body computed tomographic scanning leads to better survival as opposed to selective scanning in trauma patients: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2014;77(4):534–9. https://doi.org/10.1097/TA.0000000000000414.
Huber-Wagner S. Effect of whole-body CT during trauma resuscitation on survival: a retrospective, multicentre study. Lancet Lond Engl. 2009;373(9673):1455–61. https://doi.org/10.1016/S0140-6736(09)60232-4.
Verivox GmbH, Motorrad-Studie: Easy Rider sind über 50, presseportal.de, 17. Januar 2020. https://www.presseportal.de/pm/19139/4494491. Zugegriffen 3. Juni 2022
Sethi D, Racioppi F, Mitis F. Youth and road safety in Europe policy briefing. Copenhagen: WHO Regional Office for Europe; 2007.
Fröhlich M. Do elderly trauma patients receive the required treatment? Epidemiology and outcome of geriatric trauma patients treated at different levels of trauma care. Eur J Trauma Emerg Surg. 2020;46(6):1463–9. https://doi.org/10.1007/s00068-019-01285-0.
Cuevas-Østrem M, Røise O, Wisborg T, Jeppesen E. Epidemiology of geriatric trauma patients in Norway: a nationwide analysis of Norwegian Trauma Registry data, 2015–2018. A retrospective cohort study. Injury. 2021. https://doi.org/10.1016/j.injury.2020.11.007.
Hagebusch P, Faul P, Klug A, Gramlich Y, Hoffmann R, Schweigkofler U. Elevated serum lactate levels and age are associated with an increased risk for severe injury in trauma team activation due to trauma mechanism. Eur J Trauma Emerg Surg. 2021. https://doi.org/10.1007/s00068-021-01811-z.
Kodadek LM, Selvarajah S, Velopulos CG, Haut ER, Haider AH. Undertriage of older trauma patients: is this a national phenomenon? J Surg Res. 2015;199(1):220–9. https://doi.org/10.1016/j.jss.2015.05.017.
Hashmi A. Predictors of mortality in geriatric trauma patients: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2014. https://doi.org/10.1097/TA.0b013e3182ab0763.
Mitteilung der Kommision an das europäische Parlament, den Rat, den auropäischen Wirtschafts- und Sozialausschuss und den Ausschuss der Regionen EUROPA IN BEWEGUNG. Nachhaltige Mobilität für Europa: sicher, vernetzt und umweltfreundlich. 2018. Zugegriffen, Verfügbar unter https://eurlex.europa.eu/legal-content/DE/TXT/?uri=CELEX:52018DC0293. Accessed 22 May 2022
Funding
Prof. Dr. Lefering’s institute receives funding from an ongoing service contract with AUC GmbH, the holder of the TraumaRegister DGU®. This includes statistical consultations relating to scientific evaluations.
Author information
Authors and Affiliations
Consortia
Contributions
DAK (BG Unfallklinik Frankfurt am Main—Department of Trauma and Orthopedic Surgery) is the corresponding author. PH (BG Unfallklinik Frankfurt am Main—Department of Trauma and Orthopedic Surgery) made substantial contributions to the conception, the design of the work, the interpretation of data and was a contributor in writing the manuscript. RL (University of Witten/Herdecke—Institute for Research in Operative Medicine (IFOM)) made substantial contributions to the conception, the design of the work, the analysis and interpretation of data and substantively revised it. PF (BG Unfallklinik Frankfurt am Main—Department of Trauma and Orthopedic Surgery) made substantial contributions to the conception, the design of the work and substantively revised it. RH (BG Unfallklinik Frankfurt am Main—Department of Trauma and Orthopedic Surgery) made substantial contributions to the conception and design of the work and substantively revised it. US (BG Unfallklinik Frankfurt am Main—Department of Trauma and Orthopedic Surgery) made substantial contributions to the conception, the design of the work, the analysis and interpretation of data and substantively revised it. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The remaining authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Ethics approval
Participation in TraumaRegister DGU® and analysis of data are approved by the participants’ institutional ethical review boards. This study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Consent for publication
The TR-DGU gave permission for publication. All authors read and approved the final manuscript and gave permission for publication.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Koch, D.A., Hagebusch, P., Lefering, R. et al. Changes in injury patterns, injury severity and hospital mortality in motorized vehicle accidents: a retrospective, cross-sectional, multicenter study with 19,225 cases derived from the TraumaRegister DGU®. Eur J Trauma Emerg Surg 49, 1917–1925 (2023). https://doi.org/10.1007/s00068-023-02257-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-023-02257-1