
Abstract
Purpose
This research aimed to establish a scoring system for selecting candidates for urgent angioembolization (AE).
Methods
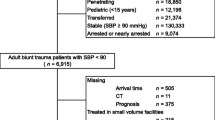
Patients with blunt trauma were retrospectively identified in a nationwide trauma registry. Patients aged ≥ 15 years with a systolic blood pressure of ≥90 mmHg were included. These individuals were then categorized into development and validation cohorts based on the date of admission. Next, an eight-point scaled system was developed using odds ratios obtained from the multivariate analysis of patients’ clinical factors on their arrival at the hospital, with the implementation of urgent AE as a dependent variable.
Results
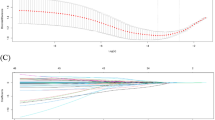
The development cohort and validation cohort included 158,192 and 116,941 patients, respectively, and 3296 (2.1%) patients in the development cohort and 2,550 (2.2%) patients in the validation cohort underwent urgent AE. The frequency of transfusion within 24 h after arrival and the Injury Severity Score were similar between the two cohorts (16,867 [10.7%] vs. 11,222 [9.6%] and 10 [9–18] vs. 10 [9–17], respectively). The number of patients who were discharged and hospital-free days were comparable between the two cohorts (139,436 [94.4%] vs. 106,107 [95.6%] and 72 [53–84] vs. 73 [57–84] days, respectively). The probabilities and the observed rates of urgent AE increased proportionally from 2% at a score of ≤ 3 to almost 15% at a score of ≥ 7. In terms of predictive factors, no significant interaction was noted.
Conclusion
The Trauma-Angio scoring system can be used as a trigger to suggest the possibility of urgent AE.
Trial Registration
20090087, 31st July 2009.


Similar content being viewed by others

References
World Health Organization. The global burden of disease 2004 update. Available at: https://apps.who.int/iris/handle/10665/43942. Accessed 16 June 2012.
Baker CC, Oppenheimer L, Stephens B, Lewis FR, Trunkey DD. Epidemiology of trauma deaths. Am J Surg. 1980;140:144–50.
Evans JA, van Wessem KJ, McDougall D, Lee KA, Lyons T, Balogh ZJ. Epidemiology of traumatic deaths: comprehensive population-based assessment. World J Surg. 2010;34:158–63.
Ierardi AM, Duka E, Lucchina N, Floridi C, De Martino A, Donat D, Fontana F, Carrafiello G. The role of interventional radiology in abdominopelvic trauma. Br J Radiol. 2016;89:20150866.
Stassen NA, Bhullar I, Cheng JD, Crandall M, Friese R, Guillamondegui O, Jawa R, Maung A, Rohs Jr TJ, Sangosanya A, Schuster K, Seamon M, Tchorz KM, Zarzuar BL, Kerwin A; Eastern Association for the Surgery of Trauma. Nonoperative management of blunt hepatic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73:S288–93.
Stassen NA, Bhullar I, Cheng JD, Crandall ML, Friese RS, Guillamondegui OD, Jawa RS, Maung AA, Rohs Jr TJ, Sangosanya A, Schuster KM, Seamon MJ, Tchorz KM, Zarzuar BL, Kerwin AJ; Eastern Association for the Surgery of Trauma. Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73:S294–300.
Cullinane DC, Schiller HJ, Zielinski MD, Bilaniuk JW, Collier BR, Como J, Holevar M, Sabater EA, Sems SA, Vassy WM, Wynne JL. Eastern Association for the Surgery of Trauma practice management guidelines for hemorrhage in pelvic fracture–update and systematic review. J Trauma. 2011;71:1850–68.
Virdis F, Reccia I, Di Saverio S, Tugnoli G, Kwan SH, Kumar J, Atzeni J, Podda M. Clinical outcomes of primary arterial embolization in severe hepatic trauma: A systematic review. Diagn Interv Imaging. 2019;100:65–75.
Miller PR, Chang MC, Hoth JJ, Mowery NT, Hildreth AN, Martin RS, Holmes JH, Meredith JW, Requarth JA. Prospective trial of angiography and embolization for all grade III to V blunt splenic injuries: nonoperative management success rate is significantly improved. J Am Coll Surg. 2014;218:644–8.
Clarke JR, Trooskin SZ, Doshi PJ, Greenwald L, Mode CJ. Time to laparotomy for intra-abdominal bleeding from trauma does affect survival for delays up to 90 minutes. J Trauma. 2002;52:420–5.
Matsushima K, Piccinini A, Schellenberg M, Cheng V, Heindel P, Strumwasser A, Benjamin E, Inaba K, Demetriades D. Effect of door-to-angioembolization time on mortality in pelvic fracture: Every hour of delay counts. J Trauma Acute Care Surg. 2018;84:685–92.
Tanizaki S, Maeda S, Matano H, Sera M, Nagai H, Ishida H. Time to pelvic embolization for hemodynamically unstable pelvic fractures may affect the survival for delays up to 60 min. Injury. 2014;45:738–41.
American College of Surgeon. Resources for Optimal Care of the Injured Patient 6th edition. Available at: https://www.facs.org/quality-programs/trauma/tqp/center-programs/vrc/resources. 2014. Accessed 04 Nov 2021.
Jarvis S, Orlando A, Blondeau B, Banton K, Reynolds C, Berg GM, Patel N, Kelly M, Carrick M, Bar-Or D. Variability in the timeliness of interventional radiology availability for angioembolization of hemodynamically unstable pelvic fractures: a prospective survey among U.S. level I trauma centers. Patient Saf Surg. 2019;13:23.
Yamamoto R, Kurihara T, Sasaki J. A novel scoring system to predict the requirement for surgical intervention in victims of motor vehicle crashes: Development and validation using independent cohorts. PLoS ONE. 2019;14: e0226282.
Hamada SR, Rosa A, Gauss T, Desclefs JP, Raux M, Harrois A, Follin A, Cook F, Boutonnet M, Attias A, Ausset S, Boutonnet M, Dhonneur G, Duranteau J, Langeron O, Paugam-Burtz C, Pirracchio R, de St MG, Vigué B, Rouquette A, Duranteau J. Development and validation of a pre-hospital “Red Flag” alert for activation of intra-hospital haemorrhage control response in blunt trauma. Crit Care. 2018;22:113.
Peduzzi P, Concato J, Feinstein AR, Holford TR. Importance of events per independent variable in proportional hazards regression analysis II. Accuracy and precision of regression estimates. J Clin Epidemiol. 1995;48:1503–10.
Eastridge BJ, Salinas J, McManus JG, Blackburn L, Bugler EM, Cooke WH, Concertino VA, Wade CE, Holcomb JB. Hypotension begins at 110 mm Hg: redefining "hypotension" with data. J Trauma. 2007;63:291–7. discussion 7–9.
Kimbrell BJ, Velmahos GC, Chan LS, Demetriades D. Angiographic embolization for pelvic fractures in older patients. Arch Surg. 2004;139:728–32. discussion 32–3.
Sartorius D, Le Manach Y, David JS, Rancurel E, Smail N, Thicoïpé M, Wiel E, Ricard-Hibon A, Berthier F, Gueugniaud PY, Riou B. Mechanism, Glasgow coma scale, age, and arterial pressure (MGAP): a new simple prehospital triage score to predict mortality in trauma patients. Crit Care Med. 2010;38:831–7.
Shiraishi A, Otomo Y, Yoshikawa S, Morishita K, Roberts I, Matsui H. Derivation and validation of an easy-to-compute trauma score that improves prognostication of mortality or the Trauma Rating Index in Age, Glasgow Coma Scale, Respiratory rate and Systolic blood pressure (TRIAGES) score. Crit Care. 2019;23:365.
Abhilash KPP, Tephilah R, Pradeeptha S, Gunasekaran K, Chandy GM. Injury patterns and outcomes of trauma in the geriatric population presenting to the emergency department in a tertiary care hospital of South India. J Emerg Trauma Shock. 2019;12:198–202.
Oakland K, Jairath V, Uberoi R, Guy R, Ayaru L, Mortensen N, Murphy MF, Collins GS. Derivation and validation of a novel risk score for safe discharge after acute lower gastrointestinal bleeding: a modelling study. Lancet Gastroenterol Hepatol. 2017;2:635–43.
Yeh DD, Chang Y, Tabrizi MB, Yu L, Cropano C, Fagenholz P, King DR, Kaafarani HM, de Moya M, Velmahos G. Derivation and validation of a practical Bedside Score for the diagnosis of cholecystitis. Am J Emerg Med. 2019;37:61–6.
Janssen KJ, Donders AR, Harrell FE Jr, Vergouwe Y, Chen Q, Grobbee DE, Moons KG. Missing covariate data in medical research: to impute is better than to ignore. J Clin Epidemiol. 2010;63:721–7.
Little RJ, D’Agostino R, Cohen ML, Dickersin K, Emerson SS, Farrar JT, Frangakis C, Hogan JW, Molenberghs G, Murphy SA, Neaton JD, Rotnitzky A, Scharfstein D, Shih WJ, Siegel JP, Stern H. The prevention and treatment of missing data in clinical trials. N Engl J Med. 2012;367:1355–60.
Yonge JD, Bohan PK, Watson JJ, Connelly CR, Eastes L, Schreiber MA. The respiratory rate: a neglected triage tool for pre-hospital identification of trauma patients. World J Surg. 2018;42:1321–6.
Bagley SC, White H, Golomb BA. Logistic regression in the medical literature: standards for use and reporting, with particular attention to one medical domain. J Clin Epidemiol. 2001;54:979–85.
Schluter PJ, Nathens A, Neal ML, Goble S, Cameron CM, Davey TM, McClure RJ. Trauma and Injury Severity Score (TRISS) coefficients 2009 revision. J Trauma. 2010;68:761–70.
American College of Surgeons. Advanced Trauma Life Support student course manual. 9th ed. Chicago, IL: American College of Surgeons; 2012.
Haider AH, Chang DC, Haut ER, Cornwell EE 3rd, Efron DT. Mechanism of injury predicts patient mortality and impairment after blunt trauma. J Surg Res. 2009;153:138–42.
Huber-Wagner S, Lefering R, Qvick LM, Körner M, Kay MV, Pfeifer KJ, Reiser M, Mutschler W, Kanz KG, Working Group on Polytrauma of the German Trauma Society. Effect of whole-body CT during trauma resuscitation on survival: a retrospective, multicentre study. Lancet. 2009;373:1455–61.
Sierink JC, Treskes K, Edwards MJ, Beuker BJ, den Hartog D, Hohmann J, Dijkgraaf MG, Luitse JS, Beenen LF, Hollmann MW, Goslings JC; REACT-2 study group. Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): A randomised controlled trial. Lancet. 2016;388:673–83.
Funding
The authors received no financial support for the preparation of this article for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest and received no financial support for the preparation of this article for publication.
Ethics approval
This study was approved by the local institutional review board for the Conduct of Human Research of all collaborating hospitals. It was approved by the ethics committee of Keio University of Medicine (approval number: 20090087). The need for informed consent was waived because anonymized data were used.
Rights and permissions
About this article

Cite this article
Maeshima, K., Yamamoto, R. & Sasaki, J. Trauma-Angio score as a predictor of urgent angioembolization for blunt trauma: development and validation using independent cohorts. Eur J Trauma Emerg Surg 48, 4837–4845 (2022). https://doi.org/10.1007/s00068-022-02008-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-022-02008-8