
Abstract
Background
Operative interventions are uncommonly required for penetrating pulmonary injuries. Similarly, because their incidence is low, few series appear sporadically in the literature. Objectives of this study are to identify predictors of outcome for patients requiring emergent thoracotomy for penetrating pulmonary injuries and evaluate the use of tissue sparing versus resective techniques for their management.
Study design
This is a retrospective 169-month study of all patients with penetrating pulmonary injuries requiring thoracotomy. The main outcome measures are: physiologic parameters, AAST-OIS injury grade, surgical procedures and mortality. Statistical analysis includes univariate and stepwise logistic regression.
Results
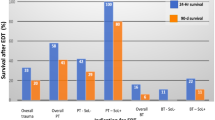
101 patients required thoracotomy for penetrating pulmonary injuries. Mechanism of injury includes: gunshot wounds (GSW)—73 (72%), stab wounds (SW)—28 (33%). Mean systolic BP 97 ± 47, mean HR 92 ± 47, and mean admission pH 7.22 ± 0.17. Mean RTS 6.25 ± 2.7, mean ISS 36 ± 22. The mean estimated blood loss (EBL) was 5277 ± 4955 mls. Predictors of outcome are: admission pH (p = 0.0014), admission base deficit (p < 0.0001), packed red blood cells (PRBCs) transfused (p = 0.023), whole blood transfused (p < 0.01). A total of 143 procedures were required in 101 patients: tissue sparing 114 (80%) versus resective procedures 29 (20%). Only pneumonectomy (p = 0.024) predicted outcome. Overall survival 64/101–64%. American Association for the Surgery of Trauma-Organ Injury Scale (AAST-OIS) injury grades I–III versus IV–VI predicts survival (p < 0.001). Stepwise logistic regression identified AAST-OIS injury grades IV–VI (p = 0.007; OR 6.38 [95% CI 1.64–24.78]), intraoperative dysrhythmias (p = 0.003; OR 17.38 [95% CI 2.59–116.49]) and associated cardiac injuries (p = 0.02; OR 8.74 [95% CI 1.37–55.79]) as independent predictors of outcome.
Conclusions
Predictors of outcome for penetrating pulmonary injuries requiring thoracotomy are identified and must be taken into account in their operative management. Tissue sparing techniques—stapled pulmonary tractotomy is once again validated, and it remains effective as the mainstay for their management; however, only pneumonectomy predicts outcome. AAST-OIS injury grades IV–VI predict outcome with higher injury grades requiring resective procedures.
Similar content being viewed by others


References
Karmy-Jones R, Jurkovich GJ, Shatz DV, Brundage S, Wall MJ Jr, Engelhardt S, Hoyt DB, Holcroft J, Knudson MM. Management of traumatic lung injury: a Western Trauma Association Multicenter review. J Trauma. 2001;51(6):1049–53.
Velmahos GC, Baker C, Demetriades D, Goodman J, Murray JA, Asensio JA. Lung-sparing surgery after penetrating trauma using tractotomy, partial lobectomy, and pneumonorrhaphy. Arch Surg. 1999;134(2):186–9.
Huh J, Wall MJ Jr, Estrera AL, Soltero ER, Mattox KL. Surgical management of traumatic pulmonary injury. Am J Surg. 2003;186(6):620–4.
Tominaga GT, Waxman K, Scannell G, Annas C, Ott RA, Gazzaniga AB. Emergency thoracotomy with lung resection following trauma. Am Surg. 1993;59(12):834–7.
Cothren C, Moore EE, Biffl WL, Franciose RJ, Offner PJ, Burch JM. Lung-sparing techniques are associated with improved outcome compared with anatomic resection for severe lung injuries. J Trauma. 2002;53(3):483–7.
Gasparri M, Karmy-Jones R, Kralovich KA, Patton JH Jr, Arbabi S. Pulmonary tractotomy versus lung resection: viable options in penetrating lung injury. J Trauma. 2001;51(6):1092–5.
Wiencek RG Jr, Wilson RF. Central lung injuries: a need for early vascular control. J Trauma. 1988;28(10):1418–24.
Graham JM, Mattox KL, Beall AC Jr. Penetrating trauma of the lung. J Trauma. 1979;19(9):665–9.
Robison PD, Harman PK, Trinkle JK, Grover FL. Management of penetrating lung injuries in civilian practice. J Thorac Cardiovasc Surg. 1988;95(2):184–90.
Stewart KC, Urschel JD, Nakai SS, Gelfand ET, Hamilton SM. Pulmonary resection for lung trauma. Ann Thorac Surg. 1997;63(6):1587–8.
Karmy-Jones R, Jurkovich GJ, Nathens AB, Shatz DV, Brundage S, Wall MJ Jr, Engelhardt S, Hoyt DB, Holcroft J, Knudson MM. Timing if urgent thoracotomy for hemorrhage after trauma: a multicenter study. Arch Surg. 2001;136(5):513–8.
Wall MJ Jr, Villavicencio RT, Miller CC 3rd, Aucar JA, Granchi TA, Liscum KR, Shin D, Mattox KL. Pulmonary tractotomy as an abbreviated thoracotomy technique. J Trauma. 1998;45(6):1015–23.
Asensio JA, Petrone P, Perez-Alonso A et al., Operative management of pulmonary injuries: Lung Sparing and formal resections. In: Asensio JA, Trunkey DD, editors. Current therapy of trauma and surgical critical care. 2nd ed. (6th ed), Chapter 39. Philadelphia: Elsevier/WB Saunders; 2015. p. 260–74.
Asensio JA, McFuffie L, Petrone P, et al. Reliable variables in the exsanguinated patient which indicate damage control and predict outcome. Am J Surg. 2001;182:743–51.
Asensio JA, Demetriades D, Berne JD, Velmahos G, Cornwell EE 3rd, Murray J, Gomez H, Falabella A, Chahwan S, Shoemaker W, Berne TV. Stapled pulmonary tractotomy: a rapid way to control hemorrhage in penetrating pulmonary injuries. J Am Coll Surg. 1997;185(5):486–7.
Moore EE, Malangoni MA, Cogbill TH, Shackford SR, Champion H, Jurkovich GJ, et al. Organ injury scaling IV: thoracic vascular, lung, cardiac, and diaphragm. J Trauma. 1994;36:299–300.
Breasted JH. The Edwin surgical papyrus, vol. 1. Chicago: University of Chicago Press; 1930. p. 369–73.
Menenakos E, Alexakis N, Leandros E, Laskaratos G, Nikiteas N, Bramis J, Fingerhut A. Fatal chest injury with lung evisceration during athletic games in ancient Greece. World J Surg. 2005;29(10):1348–51.
Galen (130–200 AD). Medicorum Graecorum Opera. vol VIII, Lipsiae Prostat in officina Libraria Car. Cuoblochii 1824, Le Locis Affectis. Edited by Kuhn DC: Tome VIII, lib V, chap 2, 304. As quoted by Beck CS. Wounds of the heart. Arch Surg. 1926;13:205–27.
Symbas PH. Cardiothoracic trauma. Curr Probl Surg. 1991;28:741–96.
Martin MJ, McDonald JM, Mullenix PS, Steele SR, Demetriades D. Operative management and outcomes of traumatic lung resection. J Am Coll Surg. 2006;203(3):336–44.
Asensio JA, Mazzini FN, Gonzalo R, Iglesias E, Vu T. Argon beam coagulator: an effective adjunct to stapled pulmonary tractotomy to control hemorrhage in penetrating pulmonary injuries. J Am Coll Surg. 2012;214(3):e9–12.
Zakharia AT. Thoracic battle injuries in the Lebanon War: review of the early operative approach in 1,992 patients. Ann Thorac Surg. 1985;40(3):209–13.
Petricevic A, Ilic N, Bacic A, Petricevic M, Vidjak V, Tanfara S. War injuries of the lungs. Eur J Cardiothorac Surg. 1997;11(5):843–7.
Wall MJ Jr, Hirshberg A, Mattox KL. Pulmonary tractotomy with selective vascular ligation for penetrating injuries to the lung. Am J Surg. 1994;168(6):665–9.
Reul GJ, Mattox KL, Beall AC Jr, Jordan GL Jr. Recent advances in the operative management of massive chest trauma. Ann Thorac Surg. 1973;16(1):52–66.
Fisher RP, Geiger JP, Guernsey JM. Pulmonary resections for severe pulmonary contusions secondary to high-velocity missile wounds. J Trauma. 1974;14(4):293–302.
Hankins JR, McAslan TC, Shin B, Ayella R, Cowley RA, McLaughlin JS. Extensive pulmonary laceration caused by blunt trauma. J Thorac Cardiovasc Surg. 1977;74(4):519–27.
Grover FL, Ellestad C, Arom KV, Root HD, Cruz AB, Trinkle JK. Diagnosis and management of major tracheobronchial injuries. Ann Thorac Surg. 1979;28(4):384–91.
Jones WS, Mavroudis C, Richardson JD, Gray LA Jr, Howe WR. Management of tracheobronchial disruption resulting from blunt trauma. Surgery. 1984;95(3):319–23.
Bowling R, Mavroudis C, Richardson JD, Flint LM, Howe WR, Gray LA Jr. Emergency pneumonectomy for penetrating and blunt trauma. Am Surg. 1985;51(3):136–9.
Thompson DA, Rowlands BJ, Walker WE, Kuykendall RC, Miller PW, Fischer RP. Urgent thoracotomy for pulmonary or tracheobronchial injury. J Trauma. 1988;28(3):276–80.
Carrillo EH, Block EF, Zeppa R, Sosa JL. Urgent lobectomy and pneumonectomy. Eur J Emerg Med. 1994;1(3):126–30.
Baumgartner F, Omari B, Lee J, Bleiweis M, Snyder R, Robertson J, Sheppard B, Milliken J. Survival after trauma pneumonectomy: the pathophysiologic balance of shock resuscitation with right heart failure. Am Surg. 1996;62(11):967–72.
Kaseda S, Hangai N, Aoki T, Yamamoto S, Nagashima A, Harada N, Satoh K. Successful emergency right pneumonectomy for deep laceration of the lung: case report. J Trauma. 1998;44(5):918–9.
Matsumoto K, Noguchi T, Ishikawa R, Mikami H, Mukai H, Fujisawa T. The surgical treatment of lung lacerations and major bronchial disruptions caused by blunt thoracic trauma. Surg Today. 1998;28(2):162–6.
Deneuville M. Injury of the pulmonary artery and its branches due to penetrating chest trauma. Ann Vasc Surg. 2000;14(5):463–7.
Cryer HG, Mavroudis C, Yu J, Roberts AM, Cué JI, Richardson JD, Polk HC Jr. Shock, transfusion, and pneumonectomy. Death is due to right heart failure and increased pulmonary vascular resistance. Ann Surg. 1990;212(2):197–201.
Author information
Authors and Affiliations
Contributions
Study conception and design: JAA. Acquisition of data: PP, ALP, LMG. Analysis and interpretation of data: JAA, PP, AJP, LMG, FNM. Drafting of manuscript: JAA, OAO. Critical revision: JAA, OAO
Corresponding author
Ethics declarations
Conflict of interest
Juan A. Asensio, Oluwaseye Ayoola Ogun, Federico N. Mazzini, Alejandro J. Perez-Alonso, Luis M. Garcia-Núñez, and Patrizio Petrone declare that they have no conflict of interest.
Research involving human participants
Approval/Exempt was obtained from the Institutional Review Board (IRB).
Informed consent
Inform consent was not required as this is a retrospective study that used prospectively collected de-identified data.
Rights and permissions
About this article

Cite this article
Asensio, J.A., Ogun, O.A., Mazzini, F.N. et al. Predictors of outcome in 101 patients requiring emergent thoracotomy for penetrating pulmonary injuries. Eur J Trauma Emerg Surg 44, 55–61 (2018). https://doi.org/10.1007/s00068-017-0802-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-017-0802-x